


ņä£ ļĪĀ
Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØĆ Ļ░äļ¼Ėļ¦ź ļé┤ļČĆņŚÉ ĒśłņĀäņØ┤ ĒśĢņä▒ļÉśļŖö Ļ▓āņ£╝ļĪ£ ņĀĢņØśļÉśļ®░, ņĄ£ĻĘ╝ Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉņŚÉņä£ ņżæņÜöĒĢ£ ļ¼ĖņĀ£ļĪ£ ĻĖēļČĆņāüĒĢśĻ│Ā ņ׳ļŗż. Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØĆ ļ¼┤ņ”ØņāüņØś ļČĆļČä ĒÅÉņāēļČĆĒä░ Ļ░äĻĖ░ļŖź ļČĆņĀäņŚÉ ņØśĒĢ£ ņĀĢļ¦źļźś ņČ£Ēśł, ņן Ļ┤┤ņé¼Ļ╣īņ¦Ć ņĢ╝ĻĖ░ĒĢĀ ņłś ņ׳ļŖö ņÖäņĀä ĒÅÉņāēĻ╣īņ¦Ć ļŗżņ¢æĒĢ£ ĒśĢĒā£ļĪ£ ļéśĒāĆļéĀ ņłś ņ׳ļŗż. Ļ░äĻ▓Įļ│Ćņ”Ø ņÖĖņŚÉļÅä ņäĀņ▓£ņĀü Ēś╣ņØĆ Ēøäņ▓£ņĀü ņØæĻ│Ā ņ¦łĒÖś, ļ│ĄļČĆ Ļ░ÉņŚ╝, ņłśņłĀņØ┤ļéś ņÖĖņāüņ£╝ļĪ£ ņØĖĒĢ£ ĒśłĻ┤Ć ļé┤Ēö╝ņäĖĒżņØś ņåÉņāüļÅä Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØä ņØ╝ņ£╝Ēé¼ ņłś ņ׳ļŗż[1]. ļśÉĒĢ£ Ļ░äņäĖĒżņĢö ļ░Å ņĀäņØ┤ņĢö ļō▒ņØś ĒśłĻ┤Ć ņ╣©ņ£żļÅä Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ļŗż[2,3]. Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉņŚÉņä£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØ┤ Ļ░äĻ▓Įļ│Ćņ”ØņØś ņĢģĒÖöļĪ£ ļ░£ņāØĒĢśļŖöņ¦Ć, ņĢäļŗłļ®┤ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ Ļ░äĻĖ░ļŖźņØ┤ ņĢģĒÖöļÉśļŖöņ¦Ć ĻĘĖ ņØĖĻ│╝Ļ┤ĆĻ│äļŖö ļ¬ģĒÖĢĒĢśņ¦Ć ņĢŖņ¦Ćļ¦ī, ņĄ£ĻĘ╝ ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤ Ļ░äĻĖ░ļŖź ņĢģĒÖöņŚÉ ļö░ļØ╝ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØ┤ ļ░£ņāØĒĢ£ļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ļŗż[2,4,5]. ņØ┤Ļ▓āņØĆ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØ┤ Ļ░äĻĖ░ļŖź ņĢģĒÖöņØś ņøÉņØĖņØ┤ļØ╝ĻĖ░ļ│┤ļŗżļŖö Ļ░äĻĖ░ļŖź ņĢģĒÖöļź╝ ļéśĒāĆļé┤ļŖö ņżæņ”ØļÅä ņ¦ĆĒæ£Ļ░Ć ļÉĀ ņłś ņ׳ļŗżļŖö Ļ▓āņØä ņØśļ»ĖĒĢ£ļŗż. ļīĆņ▓┤ļĪ£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś 30-50% ņĀĢļÅäļŖö ņ×ÉņŚ░ņĀüņ£╝ļĪ£ ĒśĖņĀäļÉśņ¦Ćļ¦ī, ņØ╝ļČĆ ņŚ░ĻĄ¼ņŚÉņä£ ņÖäņĀäĒĢ£ ĒÅÉņćäņä▒ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ ņØ┤ņŗØ Ēøä ņé¼ļ¦ØļźĀņØ┤ ņ”ØĻ░ĆĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż[5]. ļö░ļØ╝ņä£ Ļ░ä ņØ┤ņŗØņØ┤ ĒĢäņÜöĒĢ£ ĒÖśņ×ÉĻ░Ć ņÖäņĀäĒĢ£ ĒÅÉņćäņä▒ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ ņŗĀņåŹĒĢ£ ņ×¼Ļ┤Ćļźś ņĀäļץņØ┤ ĒĢäņÜöĒĢśļŗż[6]. ĻĘĖļ¤¼ļéś ņĢäņ¦ü Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØä ņ¢┤ļ¢ż ņŗ£ņłĀļĪ£ ņ¢ĖņĀ£ ņ╣śļŻīĒĢ┤ņĢ╝ ĒĢśļŖöņ¦Ć, ĒĢŁņØæĻ│ĀņĀ£ņØś ņóģļźśņÖĆ ņé¼ņÜ® ĻĖ░Ļ░ä ļō▒ņŚÉ ļīĆĒĢśņŚ¼ ņØ╝ņ╣śļÉ£ Ļ▓░ļĪĀņØ┤ ņŚåļŖö ņāüĒā£ņØ┤ļŗż. ļ│Ė ļģ╝ļ¼ĖņŚÉņä£ļŖö ņØ┤ņŚÉ ļīĆĒĢ£ ĻĖ░ņĪ┤ ņŚ░ĻĄ¼ļōżņØä ņé┤ĒÄ┤ļ│┤ļĀżĻ│Ā ĒĢ£ļŗż.
ļ│Ė ļĪĀ
ņ£Āļ│æļźĀ ļ░Å ņ×äņāü ņ”Øņāü
Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉņŚÉņä£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś ļ╣łļÅäļŖö 0.6-26%ļĪ£ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳Ļ│Ā, ļ╣äļīĆņāüņä▒ Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉņŚÉņä£ ļ╣łļÅäĻ░Ć ļŹöņÜ▒ ņ”ØĻ░ĆĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[7,8]. ņŚ¼ļ¤¼ ņŚ░ĻĄ¼ļōżņŚÉņä£ ļÅÖņ¢æņŚÉņä£ņØś ņĀäņ▓┤ Ļ░äļ¼Ėļ¦ź Ļ│ĀĒśłņĢĢņØś ņøÉņØĖ ņżæ 1/3ņØ┤ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”Øņ£╝ļĪ£ ņØĖĒĢ£ Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉ£ ļ░ö ņ׳ņ£╝ļ®░, ņä£ņ¢æņŚÉņä£ļŖö ļīĆņ▓┤ļĪ£ Ļ░äļ¼Ėļ¦ź Ļ│ĀĒśłņĢĢņØś ņøÉņØĖ ņżæ 5-10% ņĀĢļÅäļź╝ ņ░©ņ¦ĆĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż[9,10].
ņØ┤ļ¤░ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś ņ×äņāü ņ”ØņāüņØĆ ļ╣äĒŖ╣ņØ┤ņĀüņ£╝ļĪ£, ļīĆļץ 1/3 ņĀĢļÅäņØś ĒÖśņ×ÉļōżņØĆ ļ¼┤ņ”Øņāüņ£╝ļĪ£ ņÜ░ņŚ░Ē׳ Ļ▓Ćņ¦äņŚÉņä£ ļ░£Ļ▓¼ļÉśĻ│ż ĒĢ£ļŗż. Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØĆ ņŗ£Ļ░ä Ļ▓ĮĻ│╝ņŚÉ ļö░ļØ╝ ņ”Øņāü ļ░£Ēśä 60ņØ╝ņØä ĻĖ░ņżĆņ£╝ļĪ£ ĻĖēņä▒Ļ│╝ ļ¦īņä▒ņ£╝ļĪ£ ĻĄ¼ļČäĒĢ£ļŗż. ņ”ØņāüņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ ĒśłņĀäņØś ņ£äņ╣śļéś ņĀĢļÅä, ĒÖśņ×ÉņØś ļéśņØ┤ņŚÉ ļö░ļØ╝ņä£ ņ×äņāü ņ¢æņāüņØ┤ ļŗ¼ļØ╝ņ¦ł ņłś ņ׳ļŗż. ĻĖēņä▒ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņŚÉņä£ļŖö Ļ░äļ¼Ėļ¦ź Ļ│ĀĒśłņĢĢņØ┤ļéś ņĖĪļČĆ ĒśłĒ¢ēņØä Ļ┤Ćņ░░ĒĢĀ ņłś ņŚåĻ│Ā, Ļ░äĻĖ░ļŖźļÅä ņØ╝ļ░śņĀüņ£╝ļĪ£ ņĀĢņāüņØ┤ļŗż. ņ”ØņāüņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ ļ│ĄĒåĄ, ļ░£ņŚ┤, ņśżņŗ¼ ļō▒ņØś ņ”ØņāüņØä ĒśĖņåīĒĢĀ ņłś ņ׳ļŗż. ĒĢśņ¦Ćļ¦ī ĻĖēņä▒ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØ┤ ņāüņןĻ░äļ¦ēņĀĢļ¦źņŚÉ ņ׳ļŖö Ļ▓ĮņÜ░ ļ│ĄĒåĄ, ņäżņé¼ļéś ņןļ¦łļ╣äņØś ĒśĢĒā£ļĪ£ ļéśĒāĆļéĀ ņłś ņ׳ņ£╝ļ®░ ņŗ¼ĒĢĀ Ļ▓ĮņÜ░ ļ│Ąļ¦ēņŚ╝Ļ│╝ ĒĢ©Ļ╗ś Ēī©Ēśłņ”Ø, ļŗżņןĻĖ░ ļČĆņĀäĻ╣īņ¦ĆļÅä ņś¼ ņłś ņ׳ļŗż[11]. ĒŖ╣Ē׳ ļ¼Ėļ¦źņĢĢĒĢŁņ¦äņ”ØņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ņŚÉļŖö ļ¼Ėļ¦źņ£ä ļ│æņ”Øņ£╝ļĪ£ ņØĖĒĢ£ ņ£äņןĻ┤Ć ņČ£ĒśłņØś ņ£äĒŚśļÅä ņ”ØĻ░ĆĒĢĀ ņłś ņ׳ļŗż. ĻĖēņä▒ ņāüņןĻ░äļ¦ēņĀĢļ¦ź ĒśłņĀäņ”ØņØ┤ļéś ĒĢśņןĻ░äļ¦ēņĀĢļ¦ź ĒśłņĀäņ”ØņØĆ ĒŚłĒśłņ”ØņØ┤ ļÅÖļ░śļÉ£ ĻĖēņä▒ ļ│ĄĒåĄņ£╝ļĪ£ ļ░£ĒśäļÉĀ ņłś ņ׳ļŗż. ļīĆĻ░£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņŚÉņä£ ĻĖēņä▒ ņןĻ░äļ¦ē ĒŚłĒśłņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░Ļ░Ć 6-15% ņĀĢļÅä ļÉ£ļŗż[12,13].
ļ¦īņä▒ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØĆ ņØ╝ļ░śņĀüņ£╝ļĪ£ ņŗØļÅä ļ░Å ņ£äņĀĢļ¦źļźś ļśÉļŖö Ļ░äļ¼Ėļ¦źņ£ä ļ│æņ”ØņŚÉ ļö░ļźĖ ņāüļČĆņ£äņןĻ┤Ć ņČ£Ēśł, ļ▓öĒśłĻĄ¼ Ļ░Éņåīņ”ØņØä ļÅÖļ░śĒĢ£ ļ╣äņן ņóģļīĆ, ļ│Ąņłś ļō▒ņØś ņ”ØņāüņØä ļéśĒāĆļé┤ļŖö Ļ░äļ¼Ėļ¦ź Ļ│ĀĒśłņĢĢņØś ņ¦ĢĒøäļź╝ ļ│┤ņØ┤ļ®░, ļō£ļ¼╝Ļ▓ī Ļ░äļ¼Ėļ¦ź ĒĢ┤ļ®┤ ļ│ĆĒśĢņ£╝ļĪ£ ņØĖĒĢ£ ļ¼Ėļ¦źņä▒ ļŗ┤ņ”Öņ”Ø(portal cholangiopathy)ļÅä ļéśĒāĆļéĀ ņłśļÅä ņ׳ļŗż. ļśÉĒĢ£ ņØ╝ļČĆņŚÉņä£ļŖö ļ¼┤ņ”ØņāüņØ┤ĻĖ░ļÅä ĒĢśņ¦Ćļ¦ī ņØ╝ļČĆņŚÉņä£ļŖö ĒÖ®ļŗ¼ņØ┤ļéś ļŗ┤Ļ┤ĆņŚ╝, ļ│ĄĒåĄ ļō▒ņØś ņ”ØņāüņØ┤ ņāØĻĖĖ ņłś ņ׳ļŗż[14,15].
ļČäļźś ņ▓┤Ļ│ä
Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś ļČäļźś ņ▓┤Ļ│äļŖö ļŗżņ¢æĒĢśļ®░ ļīĆļČĆļČä Ļ░ä ņØ┤ņŗØ ĒÖśņ×ÉņŚÉņä£ ņśłĒøäļź╝ ņśłņĖĪĒĢśĻĖ░ ņ£äĒĢ┤ Ļ░£ļ░£ļÉśņŚłļŗż[16]. Ēśäņ×¼Ļ╣īņ¦Ć ļ│┤Ļ│ĀļÉ£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”Ø ļČäļźś ņ▓┤Ļ│äļŖö Ēæ£ 1ņŚÉ ņÜöņĢĮļÉśņ¢┤ ņ׳ļŗż[17-26]. Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØä ĻĖ░ņłĀĒĢśĻĖ░ ņ£äĒĢ£ ņŚ¼ļ¤¼ ņóģļźśņØś ļČäļźś ņ▓┤Ļ│ä ņżæ Ļ░Ćņן ņ×ÉņŻ╝ ņé¼ņÜ®ļÉśļŖö ļČäļźś ņ▓┤Ļ│ä ņżæ ĒĢśļéśņØĖ Yerdel ļČäļźśļŖö Ļ░ä ņØ┤ņŗØ ļō▒ņØś ņłśņłĀņØä ĒĢśļŖö ļÅÖņĢłņØś ņ╣śļŻī ļ░®ļ▓ĢņØä ņĀĢĒĢśļŖö ļŹ░ ņØ┤ņÜ®ļÉ£ļŗż[20]. ĒĢśņ¦Ćļ¦ī ņØ┤ ļČäļźś ņ▓┤Ļ│äļŖö ĒĢ┤ļČĆĒĢÖņĀü ļČäļźś ņ▓┤Ļ│äņØ╝ ļ┐ÉņØ┤ļ®░, ĒśłņĀäņØś ĻĖ░Ļ░äņØ┤ļéś ĒÖśņ×ÉņØś ņ”Øņāü ļō▒ņØś ņĀĢļ│┤ļŖö ņĀ£Ļ│ĄĒĢśņ¦Ć ņĢŖļŖöļŗż. ņØ┤ņŚÉ Yerdel ļČäļźśņØś ĒĢ£Ļ│äļź╝ Ļ│ĀļĀżĒĢśņŚ¼ ĒÖśņ×ÉņØś ĻĖ░ļŖźņĀü ņĀĢļ│┤ļź╝ ĒżĒĢ©ĒĢśļŖö ņāłļĪ£ņÜ┤ ļČäļźś ņ▓┤Ļ│äĻ░Ć ņĀ£ņĢłļÉśņ¢┤ ņÖöļŗż. 2016ļģä SarinņØ┤ ņĀ£ņĢłĒĢ£ ĒĢ┤ļČĆ-ĻĖ░ļŖźņĀü ļČäļźś ņ▓┤Ļ│äļŖö ĒśłņĀäņØś ņ£äņ╣śļ┐É ņĢäļŗłļØ╝ ĒÅÉņāēņØś ņĀĢļÅä, ĻĖ░Ļ░ä, ĒÖśņ×ÉņØś ņ”Øņāü, ĒśłņĀäņØś ņĀĢļÅäņÖĆ ĻĖ░ņĀĆ Ļ░ä ņ¦łĒÖśņØś ņ£Āļ¼┤ļÅä Ļ│ĀļĀżĒĢśļ®░, 2019ļģä BhanguiĻ░Ć ņĀ£ņĢłĒĢ£ ļČäļźś ņ▓┤Ļ│äņŚÉņä£ļŖö Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØä ļ│ĄĒĢ®ņä▒(complex type)Ļ│╝ ļ╣äļ│ĄĒĢ®ņä▒(non-complex type) Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ£╝ļĪ£ ļČäļźśĒĢśļ®░, ĻĖ░ļŖźņĀü, ĒśłņŚŁĒĢÖņĀü Ļ┤ĆņĀÉņŚÉņä£ ņśłĒøäļź╝ ņśłņĖĪĒĢśļŖö ļŹ░ ņØ┤ņÜ®ļÉ£ļŗż[25,26].
ļ│æĒā£ ņāØļ”¼ņÖĆ ņøÉņØĖ
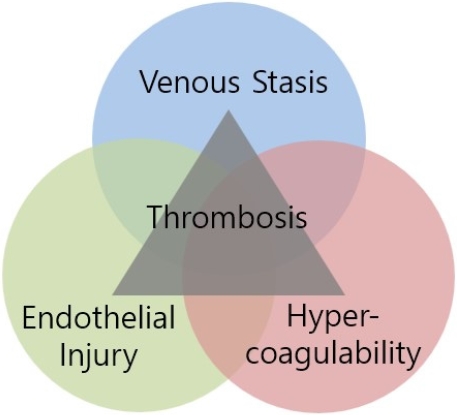
ļ╣äļīĆņāüņä▒ Ļ░äĻ▓Įļ│Ć ĒÖśņ×ÉņŚÉņä£ Ļ│╝ņØæĻ│Āņä▒, Ēśłļźś ņĀĢņ▓┤ ĻĘĖļ”¼Ļ│Ā ļé┤Ēö╝ ņäĖĒż ņåÉņāüņŚÉ ĒĢ┤ļŗ╣ĒĢśļŖö VirchowņØś ņäĖ Ļ░Ćņ¦Ć ņÜöņåīļŖö ļ¼Ėļ¦źĻ│äņÖĆ ņןĻ░äļ¦ēņĀĢļ¦źĻ│äņŚÉņä£ ĒśłņĀäņ”ØņØä ņ£Āļ░£ĒĢśļŖö ņŻ╝ņÜö ņøÉņØĖņØ┤ ļÉ£ļŗż(Table 2, Fig. 1) [27]. Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉļŖö ĻĖ░ļ│ĖņĀüņ£╝ļĪ£ Ļ│╝ņØæĻ│Ā ņāüĒā£ņŚÉ ņ׳ļŖöļŹ░, ņØ┤ļŖö ņ¦ĆĒśł ĻĘĀĒśĢņØś ļ│ĆĒÖöļĪ£ ņØĖĒĢ┤ ņ”ØĻ░ĆļÉ£ ĒŖĖļĪ¼ļ╣ł ņłśņ╣śļĪ£ ļéśĒāĆļéśļ®░, ņØæĻ│ĀņØĖņ×É ĒĢ®ņä▒ ļČĆņĪ▒ņ£╝ļĪ£ ņČ£Ēśł Ļ▓ĮĒ¢źņØ┤ ņ׳ņ£╝ļéś ņŗżņĀ£ ĒĢŁņØæĻ│ĀņØĖņ×ÉņØś ĒĢ®ņä▒ļÅä ļČĆņĪ▒ĒĢśĻĖ░ ļĢīļ¼ĖņŚÉ ņČ£Ēśł-ĒśłņĀä Ļ▓ĮĒ¢źņØĆ ĻĘĀĒśĢņØä ņØ┤ļŻ©Ļ│Ā ņ׳ļŗż[28]. ĒÖśņ×ÉļōżņØĆ ņĢłĒŗ░ĒŖĖļĪ¼ļ╣łĻ│╝ ļŗ©ļ░▒ņ¦ł CņÖĆ Ļ░ÖņØĆ ĒĢŁņØæĻ│ĀņØĖņ×É ņłśņ╣śĻ░Ć Ļ░ÉņåīĒĢ┤ ņ׳ņ£╝ļéś factor VIIIĻ│╝ von Willebrand factorņÖĆ Ļ░ÖņØĆ ņØæĻ│Āņ┤ēņ¦äņØĖņ×É ņłśņ╣śļŖö ņ”ØĻ░ĆĒĢ┤ ņ׳ļŗż. ņØ┤ Ļ▓ĮņÜ░ ĒśłņåīĒīÉ Ļ░Éņåīņ”ØņØ┤ ņØ╝ļ░śņĀüņØ┤ņ¦Ćļ¦ī ADAMTS-13ņØś Ļ░ÉņåīļĪ£ ņØĖĒĢ┤ ĒśłņåīĒīÉņØś ĒśłņĀä ņāØņä▒ ļŖźļĀźņØ┤ ņ”ØĻ░ĆĒĢśĻ▓ī ļÉ£ļŗż[1,29,30]. ņØ┤ļ¤░ Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉņŚÉņä£ ņןņĀÉļ¦ēņØś Ļ░ÉņŚ╝ ļĢīļ¼ĖņŚÉ ļ¼Ėļ¦źĻ│äļĪ£ ņäĖĻĘĀņØ┤ ņØ┤ļÅÖĒĢśņŚ¼ ņØ┤ņ░©ņĀüņ£╝ļĪ£ ļ░£ņāØĒĢśļŖö ļé┤ļÅģņåīĒśłņ”Ø ņŚŁņŗ£ ĒśłņĀäņ”ØņØä ņ£Āļ░£ĒĢśĻĖ░ļÅä ĒĢ£ļŗż[1,2,31].
Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉņŚÉņä£ļŖö ņŗżņ¦ł ĻĄ¼ņĪ░ņØś ĻĄ¼ņĪ░ņĀü ļ│ĆĒśĢņ£╝ļĪ£ ņØĖĒĢ┤ Ēśłļźś ĒØÉļ”äņØ┤ Ļ░ÉņåīĒĢśĻ│Ā ĒśłĻ┤Ć ņĀĆĒĢŁņØ┤ ņ”ØĻ░ĆĒĢśĻ▓ī ļÉ£ļŗż. ļśÉĒĢ£ ļ¼Ėļ¦źņĀäņŗĀ ņĖĪļČĆ ņł£ĒÖś ļ░Å ļé┤ņןĒśłĻ┤ĆņØś ĒÖĢņןņ£╝ļĪ£ ĒśłļźśĻ░Ć ņĀĢņ▓┤ĒĢśĻ▓ī ļÉ£ļŗż. ļ¼Ėļ¦źĻ│äņØś ņØ┤ļ¤¼ĒĢ£ ļ│ĆĒÖöļŖö Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØĻ│╝ Ļ┤ĆļĀ©ņØ┤ ņ׳ņ£╝ļ®░, ĒŖ╣Ē׳ Ļ░äļ¼Ėļ¦źņŚÉņä£ 15 cm/s ļ»Ėļ¦īņØś Ēśłļźś ņåŹļÅäļŖö ĒśłņĀäņ”ØņØś ļ░£ņāØ ņ£äĒŚśņØä ņ”ØĻ░Ćņŗ£ĒéżļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[7,32]. Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉņØś ļé┤Ēö╝ņäĖĒż ņåÉņāüņØĆ ņ×Éļ░£ņĀü ņäĖĻĘĀņä▒ ļ│Ąļ¦ēņŚ╝, ņĀäņŗĀ Ļ░ÉņŚ╝, Ļ░ä ņĀłņĀ£ņłĀ, ļé┤ņŗ£Ļ▓Į ņĀĢļ¦źļźś Ļ▓ĮĒÖö ņÜöļ▓Ģ, Ļ▓ĮņĀĢļ¦ź Ļ░ä ļé┤ ļ¼Ėļ¦źņĀäņŗĀļŗ©ļØĮ(transjugular intrahepatic portosystemic shunt, TIPS) ļ░░ņ╣ś ļśÉļŖö ĻĖ░ĒāĆ ĒśłĻ┤Ć ļé┤ ļ¼Ėļ¦ź-ņĀĢļ¦ź ņżæņ×¼ļĪ£ ņØĖĒĢ£ Ļ▓āņØ╝ ņłś ņ׳Ļ│Ā, ņØ┤ļ¤¼ĒĢ£ ņÜöņåīļōżņØ┤ Ļ░äļ¼Ėļ¦ź ĒśłņĀä ĒśĢņä▒ņŚÉ ĻĖ░ņŚ¼ĒĢĀ ņłś ņ׳ļŗż.
ņ×ÉņŚ░ Ļ▓ĮĻ│╝
Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØĆ ļŗżļźĖ ņĀĢļ¦ź ĒśłņĀäņ”ØĻ│╝ļŖö ļŗ¼ļ”¼ ņ×ÉņŚ░ Ļ▓ĮĻ│╝ņŚÉ ņ׳ņ¢┤ņä£ļÅä ļŗżņ¢æĒĢ£ Ļ▓ĮĻ│╝ļź╝ ļ│┤ņØĖļŗż[33]. Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØĆ Ļ░äĻ▓Įļ│Ćņ”ØņØ┤ ļÅÖļ░śļÉ£ Ļ▓ĮņÜ░ņÖĆ ļÅÖļ░śļÉśņ¦Ć ņĢŖņØĆ Ļ▓ĮņÜ░ņŚÉ ļö░ļØ╝ ņśłĒøäĻ░Ć ļŗżļźĖ Ļ▓ĮĻ│╝ļź╝ ļ│┤ņØ┤ļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż. Ļ░äĻ▓Įļ│Ćņ”ØņØ┤ ļÅÖļ░śļÉ£ ņØ╝ļČĆ Ļ▓ĮņÜ░ņŚÉņä£ļŖö Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś ņ×ÉņŚ░ Ļ┤ĆĒĢ┤Ļ░Ć Ļ┤Ćņ░░ļÉśĻĖ░ļÅä ĒĢ£ļŗż. ņĄ£ĻĘ╝ņØś ļ®öĒāĆļČäņäØņŚÉņä£ļŖö ĒĢŁņØæĻ│Ā ņ╣śļŻīļź╝ ļ░øņØĆ ĒÖśņ×ÉņÖĆ ļ░øņ¦Ć ņĢŖņØĆ ĒÖśņ×É ņżæ Ļ░äĻ▓Įļ│Ćņ”ØņŚÉņä£ ļÅÖļ░śļÉ£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”Ø ĒÖśņ×ÉņŚÉņä£ ĒĢŁņØæĻ│Ā ņ╣śļŻī ņŚåņØ┤ 42%ņØś ņ×¼Ļ┤Ćļźśņ£©ņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż[34]. ņØ┤ļĀćĻ▓ī ņ×ÉņŚ░ Ļ┤ĆĒĢ┤ļÉśļŖö ļ╣äņ£©ņØĆ ļīĆņāüņä▒ Ļ░äĻ▓Įļ│Ćņ”Ø, ļČĆļČä Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś Ļ▓ĮņÜ░ņŚÉņä£ ļ╣äļīĆņāüņä▒ Ļ░äĻ▓Įļ│Ćņ”Ø, Ļ░ä ņØ┤ņŗØ ļīĆĻĖ░ ĒÖśņ×Éļōżļ│┤ļŗż ļŹö ļåÆņĢśļŗż[35]. ņØ┤ļ¤░ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś Ļ┤ĆĒĢ┤ņŚÉļŖö ĻĘĖ ņÖĖņŚÉļÅä ņłśļ¦ÄņØĆ ņÜöņØĖļōżņØ┤ Ļ┤ĆĻ│äļÉśĻĖ░ ļĢīļ¼ĖņŚÉ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś ņ×¼Ļ┤Ćļźśņ£©ņŚÉ ļīĆĒĢ£ Ļ░ØĻ┤ĆņĀüņØĖ ĒÅēĻ░ĆļŖö ņēĮņ¦Ć ņĢŖļŗż. ĒĢŁņØæĻ│ĀņĀ£ ņé¼ņÜ® ņŚåņØ┤ ņ×ÉņŚ░ Ļ┤ĆĒĢ┤Ļ░Ć ļÉśļŖö Ļ▓ĮņÜ░ļÅä ņ׳ņ¦Ćļ¦ī ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ļīĆņāüņä▒ Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×Éļōż ņżæ ņ╣śļŻīļź╝ ļ░øņ¦Ć ņĢŖņØĆ ĒÖśņ×Éļōż Ļ░ĆņÜ┤ļŹ░ 33%ņŚÉņä£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØ┤ ņ¦äĒ¢ēļÉśļŖö Ļ▓░Ļ│╝ļź╝ ļ│┤ņŚ¼ņŻ╝ņŚłļŗż[34]. ļ░śļ®┤ ĒĢŁņØæĻ│Ā ņ╣śļŻī ņØ┤ĒøäņØś Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”Ø Ļ┤ĆĒĢ┤ņ£©ņØĆ ļŗżļźĖ ņĀĢļ¦ź ĒśłņĀäņ”ØņŚÉ ļ╣äĒĢ┤ ļé«ņØĆ Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśņŚłļŗż[33].
ņ¦äļŗ©
Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉņŚÉņä£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØä ņśłņĖĪĒĢśļŖö Ēśłņ▓ŁĒĢÖņĀü ņ¦ĆĒæ£ņØś ņŚŁĒĢĀņØĆ ļČłļČäļ¬ģĒĢśļŗż. D-dimerņÖĆ ļŗ©ļ░▒ņ¦ł C, ļŗ©ļ░▒ņ¦ł SņØś ņłśņ╣śĻ░Ć ņ×Āņ×¼ņĀüņØĖ ņśłņĖĪ ņØĖņ×ÉļĪ£ ņĀ£ņĢłļÉśņ¦Ćļ¦ī, ņŚ¼ļ¤¼ ņŚ░ĻĄ¼ļōżņØä ļ│┤ņĢśņØä ļĢī ņØ╝ļ░śĒÖöĻ░Ć Ļ░ĆļŖźĒĢ£ Ļ▓░ļĪĀņØä ļé┤ļ”┤ ņłśļŖö ņŚåņŚłļŗż[36,37]. ņØ┤ņĀäņŚÉ 10Ļ░Ćņ¦Ć ĻĖ░ņżĆņ£╝ļĪ£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņŚÉ ļīĆĒĢ£ ņé¼ņĀä ĒÅēĻ░ĆĻ░Ć ņĀ£ņĢłļÉ£ ņĀü ņ׳ļŖöļŹ░, ņäĖ Ļ░Ćņ¦Ć ņŻ╝ņÜö ĻĖ░ņżĆņØĆ Child-Pugh B/C, Ļ░äļ¼Ėļ¦ź ĒśłņĀä Ļ│╝Ļ▒░ļĀź ļ░Å ņĀäĒśłņĀäņä▒ ņ£äĒŚś ņØĖņ×É(factor V leiden mutation, prothrombin gene mutation, MTHFR mutation)ļź╝ ĒżĒĢ©ĒĢśĻ│Ā, ļéśļ©Ėņ¦Ć ņØ╝Ļ│▒ Ļ░Ćņ¦Ć ļČĆĻ░ĆņĀüņØĖ ĻĖ░ņżĆņŚÉļŖö ļ¼Ėļ¦źņĀäņŗĀ ļŗ©ļØĮ, ņ£äņĀĢļ¦źļźś, Ļ░äņĢö, ņĀäņŗĀņĀĢļ¦ź ĒśłņĀäņ”ØņØś ņ£Āļ¼┤, ņ£Āņé░, ĻĖēņä▒ ļ│ĄĒåĄ, Ļ░äļ¼Ėļ¦ź Ļ│ĀĒśłņĢĢ ĒĢ®ļ│æņ”ØņØś ļ░£ļ│æņØ┤ļéś ņĢģĒÖö, ņĄ£ĻĘ╝ ļé┤ņŗ£Ļ▓ĮņĀü/ņÖĖĻ│╝ņĀü/ļ░®ņé¼ņäĀ ņżæņ×¼ņłĀ ĻĖ░ņÖĢļĀź ļ░Å ļ¼Ėļ¦ź ņ£ĀņåŹņØ┤ 15 cm/s ļ»Ėļ¦īņØĖ Ļ▓ĮņÜ░ļź╝ ĒżĒĢ©ĒĢ£ļŗż. Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”Ø ņśłņĖĪņØä ņ£äĒĢ┤ ņĀ£ņĢłļÉ£ ņØ┤ 10ņĀÉ ĒÅēĻ░ĆļŖö ĒżĻ┤äņĀüņØĖ Ļ▓āņ£╝ļĪ£ ļ│┤ņØ┤ņ¦Ćļ¦ī ņĢäņ¦ü ņĀäĒ¢źņĀü ņŚ░ĻĄ¼ņŚÉņä£ Ļ▓Ćņ”ØļÉ£ ļ░öĻ░Ć ņŚåļŗż[25].
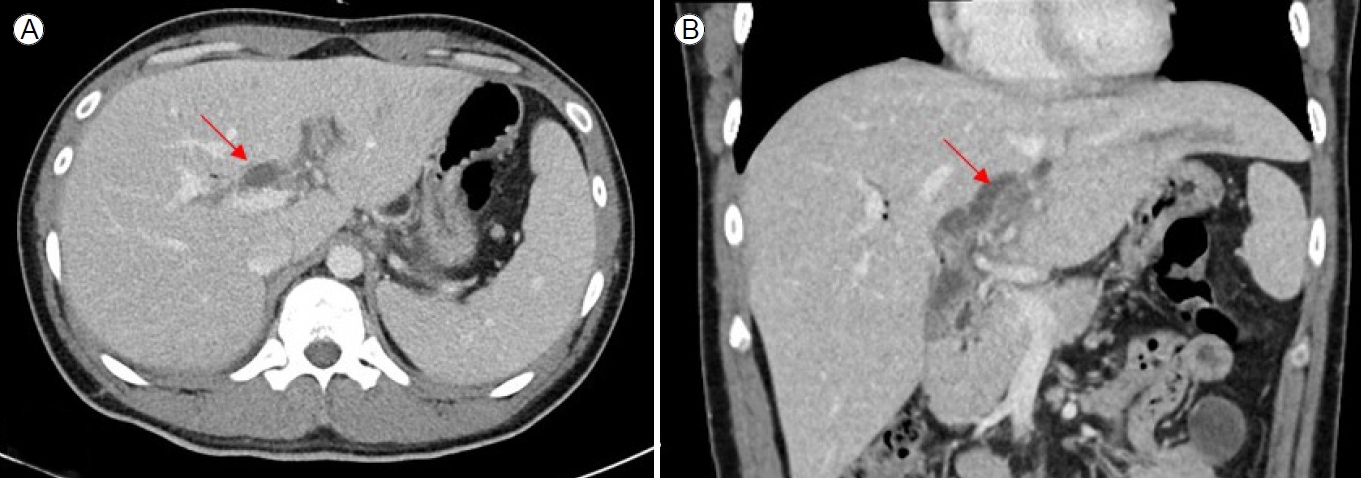
ņóģņóģ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØ┤ Ļ░äņĢö ņĀĢĻĖ░ Ļ▓Ćņ¦äņØä ļ░øļŖö Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉņŚÉņä£ ņÜ░ņŚ░Ē׳ ļ░£Ļ▓¼ļÉśĻĖ░ļÅä ĒĢ£ļŗż. ļÅäĒöīļ¤¼ ĒÅēĻ░Ćļź╝ ņØ┤ņÜ®ĒĢ£ Ļ░ä ņ┤łņØīĒīī Ļ▓Ćņé¼ļŖö Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØä ĒÖĢņØĖĒĢĀ ļĢī ņé¼ņÜ®ļÉśļŖö ņ┤łĻĖ░ Ļ▓Ćņé¼ņØ┤ļ®░, 89%ņØś ļ»╝Ļ░ÉļÅäņÖĆ 92%ņØś ĒŖ╣ņØ┤ļÅäļź╝ ļ│┤ņØĖļŗż. ĒśłĻ┤ĆņĪ░ņśü computed tomography (CT) ļ░Å ĒśłĻ┤ĆņĪ░ņśü magnetic resonance imaging (MRI)ņØĆ 90%ņØś ļ»╝Ļ░ÉļÅäņÖĆ 99%ņØś ĒŖ╣ņØ┤ļÅäļź╝ ļ│┤ņŚ¼(Fig. 2) ņ┤łņØīĒīī ļÅäĒöīļ¤¼ļ│┤ļŗż ļŹö ļ»╝Ļ░ÉĒĢśĻ│Ā ĒŖ╣ņØ┤ņĀüņØ┤ļ®░, ĒśłņĀäņØś ĻĖ░Ļ░äĻ│╝ ļ▓öņ£äņŚÉ ļīĆĒĢ£ ņĀĢļ│┤ļÅä ņĀ£Ļ│ĄĒĢ£ļŗż. ļśÉĒĢ£ ņāüļČĆ ņןĻ░äļ¦ēĻ│╝ ļ╣äņן ņĀĢļ¦źņŚÉņä£ ĒśłņĀäņØ┤ ņ׳ļŖöņ¦Ćļź╝ ĒÖĢņØĖĒĢśĻ│Ā, ņןĻ░äļ¦ēĻ│╝ Ļ░ÖņØĆ ĒśłĻ┤Ć ņÖĖ ĻĄ¼ņĪ░ņŚÉ ļ»Ėņ╣śļŖö ņśüĒ¢źņŚÉ ļīĆĒĢ£ ņĀĢļ│┤ļÅä ņĀ£Ļ│ĄĒĢśļ®░, ņĖĪļČĆ ļ░Å ļ¼Ėļ¦ź ņĀäņŗĀ ļŗ©ļØĮ ņ£Āļ¼┤ļÅä ņĢī ņłś ņ׳ļŗż[12,38]. ņØ╝ļ░śņĀüņ£╝ļĪ£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØ┤ ņØśņŗ¼ļÉśļŖö Ļ▓ĮņÜ░ Ļ░ä ļÅäĒöīļ¤¼ ņ┤łņØīĒīīļź╝ ļ©╝ņĀĆ ņŗ£Ē¢ēĒĢśļ®░, ĒśłņĀäņ”ØņØ┤ ĒÖĢņØĖļÉśļ®┤ ĒśłĻ┤ĆņĪ░ņśü CTļéś MRIļź╝ ņŗ£Ē¢ēĒĢśņŚ¼ ĒśłņĀäņØś ļ▓öņ£äņÖĆ ĒśłĻ┤Ć ņÖĖ ĻĄ¼ņĪ░ļź╝ ĒīīņĢģĒĢśļŖö Ļ▓āņØ┤ ĒĢäņÜöĒĢśļŗż.
ņØ┤ ļ░¢ņŚÉļÅä ņ¢æņä▒(bland thrombosis)Ļ│╝ ņĢģņä▒(portal vein tumor thrombosis, PVTT)ņØä ĻĄ¼ļ│äĒĢśļŖö Ļ▓āņØĆ ļ¦żņÜ░ ņżæņÜöĒĢśļŗż. Ļ░äņŗżņ¦ł ļé┤ņŚÉ Ļ░äņäĖĒżņĢöņØ┤ļéś ļŗ┤Ļ┤ĆņĢö ļō▒ņØś ņóģņ¢æņØ┤ ņ׳ņ£╝ļ®░ ņØ┤ ņóģņ¢æņØ┤ Ļ░äļ¼Ėļ¦źņØä ņ¦üņĀæ ņ╣©ļ▓öĒĢśļŖö Ļ▓ĮņÜ░ PVTTļĪ£ ņ¦äļŗ©ĒĢĀ ņłś ņ׳Ļ▓Āņ¦Ćļ¦ī, ļ¢©ņ¢┤ņĀĖ ņ׳ņ£╝ļ®┤ dynamic CTļéś MRI Ēś╣ņØĆ ļÅäĒöīļ¤¼ ņ┤łņØīĒīī ļō▒ņØś ņśüņāü ņ¦äļŗ©ņ£╝ļĪ£ ĻĄ¼ļ│äĒĢ┤ņĢ╝ ĒĢ£ļŗż. ņĢäņ¦üĻ╣īņ¦Ć ņ▓┤Ļ│äĒÖöļÉ£ ĻĄ¼ļ│äļ▓ĢņØĆ ņŚåļŖö ņāüĒÖ®ņ£╝ļĪ£ ļ¼Ėļ¦źņØś ĒÖĢļīĆ ņŚ¼ļČĆ, ļ¼Ėļ¦ź ļé┤ļČĆņŚÉ ņĀäļ░śņĀüņØĖ ņĪ░ņśüņ”ØĻ░Ģ ņŚ¼ļČĆ, ļ¼Ėļ¦ź ļé┤ ņŗĀņāØĒśłĻ┤Ć(neovascularity) ņŚ¼ļČĆ ļō▒ņØä ņóģĒĢ®ĒĢśņŚ¼ ĒīÉļŗ©ĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż. ņØ┤ņĀäņØś CTļź╝ ņØ┤ņÜ®ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ ņĢģņä▒Ļ│╝ ņ¢æņä▒ ĒśłņĀäņ”ØņŚÉņä£ ļ¼Ėļ¦ź ĒÅēĻĘĀ ņ¦üĻ▓ĮņØ┤ Ļ░üĻ░ü 23.4 mmņÖĆ 16 mmļĪ£ ņĢģņä▒ņŚÉņä£ ņ£ĀņØśĒĢśĻ▓ī ļŹö ļäōņ¢┤ņĀĖ ņ׳ļŖö Ļ▓āņØä ļ│┤Ļ│ĀĒĢ£ ļ░ö ņ׳ļŗż[39].
ĻĖēņä▒ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś ņ╣śļŻī
Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉņŚÉņä£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØ┤ ļ░£ņāØĒ¢łņØä ļĢī ņĄ£ņĀüņØś ņ╣śļŻīļŖö ņĢäņ¦ü ļ¬ģĒÖĢĒĢ£ ĻČīņן ņé¼ĒĢŁņØ┤ ņŚåņ¢┤ ļČłļČäļ¬ģĒĢśņ¦Ćļ¦ī ĒĢŁņØæĻ│Ā ņÜöļ▓ĢņØĆ ĒśłņĀäņØś ĒÖĢņן ļśÉļŖö ņ×¼ļ░£ ļ░®ņ¦Ć, ĒśłĻ┤Ć Ļ░£ĒåĄņä▒ņØś ĒÖĢļ”Į, Ļ░äļ¼Ėļ¦ź Ļ│ĀĒśłņĢĢ ļ░Å ņן ĒŚłĒśłĻ│╝ Ļ░ÖņØĆ ĒĢ®ļ│æņ”Ø ņśłļ░®ņØä ņ£äĒĢ£ ņĄ£ņäĀņØś ņ╣śļŻīņØĖ Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż.
ĒĢŁņØæĻ│Ā ņÜöļ▓Ģ
Ļ░äĻ▓Įļ│Ćņ”ØņŚÉņä£ ļÅÖļ░śļÉ£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņŚÉ ĒĢŁņØæĻ│ĀņĀ£ļź╝ ņé¼ņÜ®ĒĢśĻĖ░ ņĀä Ļ░äļ¼Ėļ¦ź Ļ│ĀĒśłņĢĢņ£╝ļĪ£ ņØĖĒĢ£ ņČ£Ēśł ņ£äĒŚśļÅä, Ļ░äĻ▓Įļ│Ćņ”ØņØś ņżæņ”ØļÅä, ĒÅÉņāēļÉ£ ĒśłĻ┤Ć ņ×¼Ļ┤ĆļźśņØś ņØ┤ņĀÉņØä ņŗĀņżæĒĢśĻ▓ī Ļ│ĀļĀżĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż. ĻĖ░ņĪ┤ ņŚ░ĻĄ¼ļōżņŚÉņä£ ĒĢŁņØæĻ│ĀņĀ£ ņé¼ņÜ®ņØś ņĀüņĀłĒĢ£ ņŗ£ĻĖ░ļéś ņĀüņØæņ”ØņŚÉ ļīĆĒĢ┤ņä£ļŖö ĻĄ¼ņ▓┤ņĀüņ£╝ļĪ£ ņĀĢĒĢ┤ņ¦ä ĒĢ®ņØśļŖö ņŚåņ£╝ļéś ļ╣äĻĄÉņĀü ņĢłņĀäĒĢśļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ļŗż. ĒĢ£ ĒøäĒ¢źņĀü ņŚ░ĻĄ¼ņŚÉņä£ ĒĢŁņØæĻ│ĀņĀ£ļź╝ Ēł¼ņŚ¼ļ░øņØĆ ļ¼Ėļ¦źņĢĢĒĢŁņ¦äņ”Ø ĒÖśņ×ÉņŚÉņä£ļŖö ņ×¼ņČ£ĒśłļźĀ, ņ×ģņøÉ ĻĖ░Ļ░ä, 6ņŻ╝ ņé¼ļ¦ØļźĀ ļśÉļŖö TIPS ņéĮņ×ģĻ│╝ Ļ░ÖņØĆ ĻĄ¼ņĪ░ ņÜöļ▓ĢņØś ĒĢäņÜöņä▒ņØ┤ ņ”ØĻ░ĆĒĢśņ¦Ć ņĢŖņĢśļŗż[6]. ļśÉ ļŗżļźĖ ņŚ░ĻĄ¼ņŚÉņä£ļŖö 52ļ¬ģņØś ĒĢŁņØæĻ│Ā ņ╣śļŻīļź╝ ļ░øļŖö ĒÖśņ×ÉņÖĆ 104ļ¬ģņØś ĒĢŁņØæĻ│Ā ņ╣śļŻīļź╝ ļ░øņ¦Ć ņĢŖļŖö ĒÖśņ×Éļź╝ ļ╣äĻĄÉĒĢśņśĆļŖöļŹ░ ļæÉ ĻĄ░ņŚÉņä£ ņČ£ĒśłņØś ļ░£ņāØļźĀņØĆ ĒĢŁņØæĻ│ĀņĀ£ ņŚ¼ļČĆņŚÉ Ļ┤ĆĻ│äņŚåņØ┤ ļÅÖņØ╝Ē¢łĻ│Ā, ņØ┤ņÖĆ ņ£Āņé¼ĒĢ£ Ļ▓░Ļ│╝Ļ░Ć ļŗżļźĖ ņŚ░ĻĄ¼ņŚÉņä£ļÅä ļéśĒāĆļé¼ļŗż[40,41].
Ļ░äļ¼Ėļ¦źņØś ņ×¼Ļ┤Ćļźśņ£©ņØĆ ĒĢŁņØæĻ│Ā ņ╣śļŻīļź╝ ļ░øņØĆ ĒÖśņ×ÉļōżņŚÉņä£ ļ░øņ¦Ć ņĢŖņØĆ ņé¼ļ×īļōżļ│┤ļŗż ļŹö ļåÆņĢśĻ│Ā(51.4% vs. 18.8%; p= 0.005) [34], ņ▓┤Ļ│äņĀü ļ¼ĖĒŚī Ļ│Āņ░░ņŚÉņä£ļÅä ņØ┤ņÖĆ ļ╣äņŖĘĒĢ£ Ļ▓░Ļ│╝Ļ░Ć ļ│┤Ļ│ĀļÉśņŚłļŗż(33-75%) [6,34,41]. ĒĢ£ ļŗżļ│Ćļ¤ē ļČäņäØņŚÉņä£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņØś ņ¦äļŗ© ļŗ╣ņŗ£ņØś model for end-stage liver disease (MELD) ņĀÉņłśĻ░Ć Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉņŚÉņä£ ĒĢŁņØæĻ│Ā ņ╣śļŻīņØś ņ×¼Ļ┤Ćļźśņ£©ņØä ņ£ĀņØśĒĢśĻ▓ī ņśłņĖĪĒĢĀ ņłś ņ׳ņØīņØ┤ ļ│┤Ļ│ĀļÉ£ ļ░ö ņ׳ļŗż(hazard ratio, 1.105; 95% confidence interval, 1.012-1.207; p= 0.027) [6]. ņ×¼ĒśłņĀäņ”ØņØś ļ░£ņāØļźĀņØĆ ĒĢŁņØæĻ│ĀņĀ£ļź╝ ņżæļŗ©ĒĢ£ ĒÖśņ×ÉņŚÉņä£ 35.3%ņśĆĻ│Ā ņØ┤ļŖö ņØ┤ņĀäņØś ļŗżļźĖ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ņÖĆļÅä ļ╣äņŖĘĒĢśņśĆļŗż[6,42,43]. ņØ┤ļ¤¼ĒĢ£ ņŚ░ĻĄ¼ļōżņØĆ ņ¦ĆņåŹņĀüņØĖ ĒśłņĀäņ”ØņØ┤ Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉņØś ļ¼Ėļ¦źĻ│äņŚÉ ņĪ┤ņ×¼ĒĢśļŖö Ļ▓āņØä ņŗ£ņé¼ĒĢ£ļŗż. ļö░ļØ╝ņä£ ĻĖłĻĖ░ņé¼ĒĢŁņØ┤ ņŚåļŖö ĒĢ£ ĒĢŁņØæĻ│ĀņĀ£ļź╝ ņ¦ĆņåŹņĀüņ£╝ļĪ£ ņ£Āņ¦ĆĒĢśļŖö Ļ▓āņØś ĻĘ╝Ļ▒░Ļ░Ć ļÉĀ ņłś ņ׳ļŗż[44].
ĒĢŁņØæĻ│ĀņĀ£ņØś ņŗ£ņ×æ ņŗ£ņĀÉņØĆ ņ×¼Ļ┤Ćļźśņ£©ņØś ņżæņÜöĒĢ£ ņØĖņ×ÉļĪ£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”Ø ņ¦äļŗ© ņØ┤Ēøä 6Ļ░£ņøö ņØ┤ļé┤ņŚÉ ĒĢŁņØæĻ│ĀņĀ£ļź╝ ņŗ£ņ×æĒĢśļŖö Ļ▓āņØĆ ļŹö ļåÆņØĆ ņ×¼Ļ┤Ćļźśņ£©Ļ│╝ ņŚ░Ļ┤Ćņä▒ņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż[43,45,46]. ĻĘĖļ¤¼ļéś ĒĢŁņØæĻ│ĀņĀ£ņØś ņ£Āņ¦Ć ĻĖ░Ļ░äņØĆ ņé¼ņÜ®ĒĢśļŖö ĒĢŁņØæĻ│ĀņĀ£ņØś ņóģļźśņŚÉ ļö░ļØ╝ ļŗżņ¢æĒĢśļ®░ ņŚ░ĻĄ¼ļōżļ¦łļŗż ļööņ×ÉņØĖņØ┤ ļŗżļź┤ĻĖ░ ļĢīļ¼ĖņŚÉ ļ¬ģĒÖĢĒĢśĻ▓ī ĒĢ®ņØśļÉ£ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņØĆ ņŚåļŗż.
Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØĆ ņØ┤ņŗØ ļīĆĻĖ░ņ×É ļ¬ģļŗ© ņé¼ļ¦ØļźĀņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣śņ¦Ć ņĢŖņ¦Ćļ¦ī Ļ░ä ņØ┤ņŗØ ņłśņłĀ ņŗ£ņŚÉ ņłśĒśł ņÜöĻĄ¼ļ¤ē ņ”ØĻ░Ć, ĻĖ┤ ņłśņłĀ ņŗ£Ļ░ä, ņØ┤ņŗØ Ēøä ņé¼ļ¦ØļźĀ ņ”ØĻ░Ć, ņØ┤ņŗØ Ēøä ņżæņ×¼ņĀü ņ╣śļŻī ņ”ØĻ░ĆņÖĆ ņŚ░Ļ┤ĆļÉśņ¢┤ ņ׳ļŗż. ĻĘĖļ¤¼ļ»ĆļĪ£ Ļ░äĻ▓Įļ│Ćņ”ØĻ│╝ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØ┤ ļÅÖļ░śļÉ£ ĒÖśņ×ÉņŚÉņä£ Ļ░ä ņØ┤ņŗØ ļīĆĻĖ░ ņŗ£ ĒĢŁņØæĻ│ĀņĀ£ ņé¼ņÜ®ņØ┤ ņČöņ▓£ļÉ£ļŗż[47].
ņĢäņ¦üĻ╣īņ¦ĆļŖö ņĀ£ĒĢ£ļÉ£ ņ×äņāü ļŹ░ņØ┤Ēä░ļĪ£ ņØĖĒĢ┤ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņŚÉ ļīĆĒĢ£ ņØ┤ņāüņĀüņØĖ ĒĢŁņØæĻ│ĀņĀ£ ņé¼ņÜ®ņŚÉ ļīĆĒĢśņŚ¼ ĒĢ®ņØśĻ░Ć ļČĆņĪ▒ĒĢ£ ņāüĒÖ®ņØ┤ļŗż[48]. ĒĢŁņØæĻ│Ā ņÜöļ▓Ģņ£╝ļĪ£ ņō░ņØ┤ļŖö ņĢĮļ¼╝ļĪ£ļŖö ļ╣äĒāĆļ»╝K ĻĖĖĒĢŁņĀ£(ņÖĆĒīīļ”░), ļ»ĖļČäĒÜŹ ĒŚżĒīīļ”░(unfractionated heparin), ņĀĆļČäņ×Éļ¤ē ĒŚżĒīīļ”░, fondaparinux, direct oral anticoagulants (DOAC) ļō▒ ļŗżņ¢æĒĢ£ ņśĄņģśņØ┤ ņĪ┤ņ×¼ĒĢ£ļŗż. ĻĖ░ņĪ┤ ņŚ░ĻĄ¼ņŚÉņä£ ņÖĆĒīīļ”░Ļ│╝ ņĀĆļČäņ×Éļ¤ē ĒŚżĒīīļ”░ņØä ņØ┤ņÜ®ĒĢ£ Ļ▓ĮņÜ░ ļ╣äņŖĘĒĢ£ ņ╣śļŻī ņä▒ņĀüņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż[34]. ņØ╝ļ░śņĀüņ£╝ļĪ£ ņ×ģņøÉ ĒÖśņ×ÉļōżņŚÉĻ▓īļŖö Ļ┤æļ▓öņ£äĒĢ£ Ļ░ĆņÜ®ņä▒Ļ│╝ ņ¦¦ņØĆ ļ░śĻ░ÉĻĖ░ļź╝ Ļ░Ćņ¦Ćļ®░ Ļ░ĆņŚŁņä▒ņØä Ļ│ĀļĀżĒĢśņŚ¼ ņ▓┤ņżæ ĻĖ░ļ░ś ņĀĢļ¦ź ļé┤ ĒŚżĒīīļ”░ņØ┤ ņ▓śļ░®ļÉśļ®░ ņÖĖļל ĒÖśņ×ÉņØś Ļ▓ĮņÜ░ ņÖĆĒīīļ”░ņØ┤ļéś ņĀĆļČäņ×Éļ¤ē ĒŚżĒīīļ”░, DOAC ņĀ£ņĀ£ ļō▒ņØś ļŗżņ¢æĒĢ£ ņśĄņģśņØä ņé¼ņÜ®ĒĢśĻ│ż ĒĢ£ļŗż[14].
ļ»ĖļČäĒÜŹ ĒŚżĒīīļ”░
Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś ņ╣śļŻīņŚÉ ņ׳ņ¢┤ņä£ ļ»ĖļČäĒÜŹ ĒŚżĒīīļ”░ņØĆ ņŗĀĻĖ░ļŖźņØ┤ ļČłļ¤ēĒĢ£ ĒÖśņ×Éļéś ņן ĒŚłĒśłņØś Ļ░ĆļŖźņä▒ņØ┤ ņ׳ļŖö ĒÖśņ×ÉņŚÉņä£ ļ╣ĀļźĖ ĒĢŁņØæĻ│Ā ņŚŁĒĢĀņØä ņ£äĒĢ┤ ņ┤łĻĖ░ ņ╣śļŻīņĀ£ļĪ£ ņé¼ņÜ®ļÉĀ ņłś ņ׳ļŗż. ĒĢśņ¦Ćļ¦ī ļ»ĖļČäĒÜŹ ĒŚżĒīīļ”░ņØĆ ņĀĢļ¦ź ļé┤ Ēł¼ņŚ¼ĒĢśļŖö ļ░®ņŗØņ£╝ļĪ£, ņןĻĖ░Ļ░ä ņ╣śļŻīĒĢśļŖö ļŹ░ņŚÉļŖö ņĀüĒĢ®ĒĢśņ¦Ć ņĢŖņĢä ņé¼ņÜ®ņØ┤ ņĀ£ĒĢ£ņĀüņØ┤ļŗż[49].
ņĀĆļČäņ×Éļ¤ē ĒŚżĒīīļ”░
ņĀĆļČäņ×Éļ¤ē ĒŚżĒīīļ”░ņØĆ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś ņ┤łĻĖ░ ņ╣śļŻīņĀ£ļĪ£ ļ¦ÄņØĆ Ļ▓ĮņÜ░ņŚÉ ņé¼ņÜ®ļÉśļéś, Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś ņ╣śļŻīļŖö ņןĻĖ░ņĀüņ£╝ļĪ£ ĒĢśļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äņ£╝ļ»ĆļĪ£ ĒÖśņ×ÉņØś ņł£ņØæļÅäņÖĆ Ļ┤ĆļĀ©ĒĢ┤ Ļ▓░ĻĄŁ ņÖĆĒīīļ”░Ļ│╝ DOAC ņĀ£ņĀ£ļź╝ ņé¼ņÜ®ĒĢśĻĖ░ ņĀä ļĖīļ”┐ņ¦Ć ņ╣śļŻī(bridge therapy)ņŚÉ ņé¼ņÜ®ļÉ£ļŗż. ņé¼ņÜ®ļÉśļŖö ļ░®ļ▓ĢņØĆ ĻĖ░Ļ┤Ćļ¦łļŗż ņāüņØ┤ĒĢĀ ņłś ņ׳ņ¦Ćļ¦ī ņÖĆĒīīļ”░Ļ│╝ ļÅÖņŗ£ņŚÉ Ēł¼ņĢĮņØä ņŗ£ņ×æĒĢśņŚ¼ INRņØ┤ ņ╣śļŻī ļ▓öņ£äņØĖ 2-3ņŚÉ ļÅäļŗ¼ĒĢśļ®┤ ņĀĆļČäņ×Éļ¤ē ĒŚżĒīīļ”░ņØä ņżæļŗ©ĒĢśĻ│ż ĒĢ£ļŗż[50]. ĻĘĖļ¤¼ļéś ņØ╝ļČĆ ĒÖśņ×Éļōż(ņ×¼ļ░£ņä▒ ļ│ĄļČĆļĪ£ ņØĖĒĢ┤ ņ¦ĆņåŹņĀüņØĖ ļ│Ąņłś ņ▓£ņ×Éļź╝ ĒĢäņÜöĒĢśļŖö ĒÖśņ×É, INRņØ┤ ņ¦ĆņåŹņĀüņ£╝ļĪ£ ļåÆņØĆ ĒÖśņ×É ļō▒)ņŚÉņä£ļŖö ņĀĆļČäņ×Éļ¤ē ĒŚżĒīīļ”░ņØ┤ ņÖĆĒīīļ”░ļ│┤ļŗż ļŹö ņĀüĒĢ®ĒĢĀ ņłś ņ׳ļŗż. ņÜ®ļ¤ēĻ│╝ Ļ┤ĆļĀ©ļÉ£ ņŚ░ĻĄ¼ņŚÉņä£ enoxaparinņØä 1 mg/kg ņé¼ņÜ®ĒĢ£ ĻĘĖļŻ╣ņØ┤ 1.5 mg/kg ņé¼ņÜ®ĒĢ£ ĻĘĖļŻ╣ļ│┤ļŗż ļ╣äņŖĘĒĢ£ ĒÜ©Ļ│╝ļź╝ ļ│┤ņØ┤ļ®┤ņä£ ĒĢ®ļ│æņ”ØņØĆ ņĀüņŚłļŗżļŖö ļ│┤Ļ│ĀĻ░Ć ņ׳ļŗż[51]. ņĀĆļČäņ×Éļ¤ē ĒŚżĒīīļ”░ņØä Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś ņ╣śļŻīņŚÉ ņé¼ņÜ®ĒĢ£ ĻĖ░ņĪ┤ņØś ļ¬ćļ¬ć ņŚ░ĻĄ¼ņŚÉņä£ļŖö ĒÅēĻĘĀ 6Ļ░£ņøöņØś ĻĖ░Ļ░ä ļÅÖņĢł ņé¼ņÜ® Ēøä ņ×¼Ļ┤Ćļźś ņŚ¼ļČĆļź╝ ĒÅēĻ░ĆĒĢśņśĆļŗż[43,51].
ņÖĆĒīīļ”░
ņÖĆĒīīļ”░ņØĆ ņĀĆļČäņ×Éļ¤ē ĒŚżĒīīļ”░Ļ│╝ ļ╣äĻĄÉĒĢśņśĆņØä ļĢī ļ╣äņŖĘĒĢ£ ņ×¼Ļ┤Ćļźśņ£© ņä▒ņĀüĻ│╝ ļ╣äņŖĘĒĢ£ ļČĆņ×æņÜ® ļ╣äņ£©ņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż[52,53]. ĒĢśņ¦Ćļ¦ī ņóüņØĆ ņ╣śļŻī ļ▓öņ£äļĪ£ ņØĖĒĢśņŚ¼ ņŻ╝ĻĖ░ņĀüņ£╝ļĪ£ ļ¬©ļŗłĒä░ļ¦üņØä ĒĢ┤ņĢ╝ ĒĢĀ ĒĢäņÜöņä▒Ļ│╝ Ļ░äĻ▓Įļ│Ćņ”ØņŚÉņä£ ĻĖ░ļ│ĖņĀüņ£╝ļĪ£ ņāüņŖ╣ļÉśņ¢┤ ņ׳ļŖö ĻĖ░ņĀĆ INR ņłśņ╣śļĪ£ ņØĖĒĢ┤ Ļ│╝ņåī Ēł¼ņŚ¼ļÉĀ Ļ░ĆļŖźņä▒ņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ļŗż. Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś ņ╣śļŻīņĀ£ļĪ£ ņÖĆĒīīļ”░ņØä ņØ┤ņÜ®ĒĢ£ ĻĖ░ņĪ┤ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ĒÅēĻĘĀ 3Ļ░£ņøöļČĆĒä░ 2ļģäĻ╣īņ¦Ć ņé¼ņÜ® Ēøä ņ×¼Ļ┤Ćļźś ņŚ¼ļČĆļź╝ ĒÅēĻ░ĆĒĢśņśĆļŗż[54-56].
Direct oral anticoagulants
ņĄ£ĻĘ╝ direct thrombin inhibitor (dabigatran) ļ░Å factor Xa inhibitor (rivaroxaban, apixaban, and edoxaban)ļź╝ ĒżĒĢ©ĒĢ£ DOACĻ░Ć Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”Ø ņ╣śļŻīņŚÉ ņé¼ņÜ®ļÉśĻ│Ā ņ׳ļŗż. DOACļŖö ņÖĆĒīīļ”░Ļ│╝ ļ╣äĻĄÉĒĢśņŚ¼ Ļ│ĀņĀĢļÉ£ ņÜ®ļ¤ēņ£╝ļĪ£ ņé¼ņÜ®ņØ┤ Ļ░ĆļŖźĒĢśļ®░ ĻĄ¼Ļ░Ģ Ēł¼ņŚ¼Ļ░Ć Ļ░ĆļŖźĒĢśĻ│Ā ļŗżļźĖ ņĢĮļ¼╝Ļ│╝ņØś ņāüĒśĖņ×æņÜ®ņØ┤ Ļ▒░ņØś ņŚåļŗżļŖö ņןņĀÉņØ┤ ņ׳ļŗż. ņĄ£ĻĘ╝ ļ│┤Ļ│ĀļÉ£ ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤ Child-Pugh Aļŗ©Ļ│äņØś ĒÖśņ×ÉņŚÉņä£ DOAC ņé¼ņÜ®ņŚÉ ļīĆĒĢ£ ņĢłņĀäņä▒ ļ¼ĖņĀ£ļŖö ņŚåņŚłņ¦Ćļ¦ī Child-Pugh Cļŗ©Ļ│äņØś ĒÖśņ×ÉņŚÉņä£ļŖö DOAC ņé¼ņÜ®ņØ┤ ĻČīņ£ĀļÉśņ¦Ć ņĢŖņĢśļŗż[57]. ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ rivaroxabanņØ┤ ņÖĆĒīīļ”░ļ│┤ļŗż ņ×¼Ļ┤Ćļźśņ£©, Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØś ņ×¼ļ░£ ņĖĪļ®┤ņŚÉņä£ ļŹö ĒÜ©Ļ│╝ņĀüņØ┤ņŚłļŗżļŖö Ļ▓░Ļ│╝ļź╝ ļ│┤ņŚ¼ņżĆ ļ░ö ņ׳Ļ│Ā, edoxaban, dabigatranņØä ņØ┤ņÜ®ĒĢ£ ņĀäĒ¢źņĀü ņŚ░ĻĄ¼ņŚÉņä£ļÅä ņØ┤ņÖĆ ņ£Āņé¼ĒĢ£ Ļ▓░Ļ│╝Ļ░Ć ļéśĒāĆļé¼ļŗż[55,58,59]. ņĢłņĀäņä▒ ņĖĪļ®┤ņŚÉņä£ļŖö ņĄ£ĻĘ╝ņØś ĒĢ£ ļ®öĒāĆļČäņäØņŚÉņä£ Ļ░äĻ▓Įļ│Ćņ”ØņŚÉ ļÅÖļ░śļÉ£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”Ø ĒÖśņ×ÉņŚÉņä£ DOACĻ░Ć ņÖĆĒīīļ”░ņŚÉ ļ╣äĒĢ┤ ņČ£Ēśł ĒĢ®ļ│æņ”Ø ņĖĪļ®┤ņŚÉņä£ ņ£Āņé¼ĒĢśĻ▒░ļéś ļŹö ļéśņØĆ ņĢłņĀäņä▒ņØä ļ│┤ņŚ¼ņżĆļŗżĻ│Ā ĒĢśņśĆļŗż[60]. ĒĢśņ¦Ćļ¦ī ņĢäņ¦üĻ╣īņ¦ĆļŖö ĻĖ░ņĪ┤ņØś ĒŚżĒīīļ”░ņØ┤ļéś ņÖĆĒīīļ”░ ņĀ£ņĀ£ņŚÉ ļ╣äĒĢ┤ ĻĘ╝Ļ▒░ ņłśņżĆņØ┤ ļ╣łņĢĮĒĢśĻ│Ā, ļ╣äņÜ® ļČĆļČäņŚÉ ņ׳ņ¢┤ ĒÖśņ×É ļČĆļŗ┤ņØ┤ ņ׳ņ¢┤ ņé¼ņÜ®ņŚÉ ņØ╝ļČĆ ņĀ£ĒĢ£ņØ┤ ņ׳ļŖö ņāüĒā£ļŗż. DOAC ņĀ£ņĀ£ ņżæņŚÉņä£ rivaroxabanņØä 10 mg ĒĢśļŻ© ļæÉ ļ▓ł ņé¼ņÜ®ĒĢśņśĆļŹś ņĀäĒ¢źņĀü ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņĄ£ļīĆ 6Ļ░£ņøöĻ╣īņ¦Ć ņé¼ņÜ® Ēøä ņ×¼Ļ░£ĒåĄ ņŚ¼ļČĆļź╝ ĒÅēĻ░ĆĒĢ£ ļ░ö ņ׳ļŗż[55].
ĒĢŁņØæĻ│ĀņĀ£ņØś ļČĆņ×æņÜ®
ņČ£ĒśłņØĆ ĒĢŁņØæĻ│ĀņĀ£ ņé¼ņÜ®ņØś Ļ░Ćņן ĒØöĒĢ£ ļČĆņ×æņÜ®ņ£╝ļĪ£ ņĀĢļ¦źļźś ņČ£ĒśłņØ┤ļéś ļ╣äņĀĢļ¦źļźś ņČ£Ēśł ļō▒ ļŗżņ¢æĒĢ£ ņ¢æņāüņØś ņČ£ĒśłņØ┤ ņ׳ļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ņ¦Ćļ¦ī, ĻĖ░ņĪ┤ ņŚ░ĻĄ¼ļōżņŚÉņä£ ņČ£ĒśłņØś ņĀĢņØśĻ░Ć ņŚ░ĻĄ¼ļ¦łļŗż ņāüņØ┤ĒĢśĻ│Ā ņØśļ»ĖĻ░Ć ĒÖĢļ”ĮļÉśņ¢┤ ņ׳ņ¦Ć ņĢŖņĢä ņĀĢĒÖĢĒĢ£ ļ╣äĻĄÉļŖö ņ¢┤ļĀĄļŗż.
ņĄ£ĻĘ╝ņØś ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ ĒĢŁņØæĻ│Ā ņ╣śļŻīļź╝ ļ░øļŖö Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉļōżņØä ĒĢŁņØæĻ│Ā ņ╣śļŻīļź╝ ļ░øņ¦Ć ņĢŖļŖö Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉļōżņØä ļ╣äĻĄÉĒĢśņśĆņØä ļĢī, ĒĢŁņØæĻ│Ā ņ╣śļŻīļź╝ ļ░øņ¦Ć ņĢŖļŖö ĒÖśņ×ÉļōżņŚÉņä£ ņČ£ĒśłņØś ņĀĢļÅäļéś ņé¼ļ¦ØļźĀņØ┤ ņ”ØĻ░ĆĒĢśņ¦Ć ņĢŖņĢśļŗż[40]. ļö░ļØ╝ņä£ ĒÖśņ×ÉņØś ĻĖ░ņĀĆ ņ¦łĒÖśņØ┤ļéś ĒśłņĢĪĒĢÖņĀü Ļ▓Ćņé¼ ņåīĻ▓¼ņØä ņ░ĖĻ│ĀĒĢśņŚ¼ ņØ┤ņĀÉ ļ░Å ņ£äĒŚśņä▒ņØä ĒÅēĻ░ĆĒĢśĻ│Ā ĒĢŁņØæĻ│ĀņĀ£ļź╝ ņé¼ņÜ®ĒĢśļŖö Ļ▓āņØä Ļ│ĀļĀżĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż.
ņżæņ×¼ņĀü ņŗ£ņłĀ
ĻĖēņä▒ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņŚÉņä£ ĒĢŁņØæĻ│ĀņĀ£ ņÖĖņŚÉ ņżæņ×¼ņĀü ņŗ£ņłĀļÅä ĒĢśļéśņØś ņ╣śļŻī ļ░®ļ▓ĢņØ┤ļŗż. ņĢäņ¦üĻ╣īņ¦Ć ņĀĢĒÖĢĒĢ£ ņĀüņØæņ”ØņØĆ ĒĢ®ņØśļÉ£ ļ░öĻ░Ć ņŚåņ¦Ćļ¦ī, ņØ┤ļ¤¼ĒĢ£ ņżæņ×¼ņĀü ņŗ£ņłĀņŚÉļŖö ĻĖ░Ļ│äņĀü ĒśłņĀä ņĀ£Ļ▒░ņłĀ ļ░Å ņ╣┤ĒģīĒä░ ņ£ĀļÅä ĒśłņĀä ņÜ®ĒĢ┤ņłĀ, ņŗØļÅä ļ░Å ņ£äņĀĢļ¦źļźś ņ╣śļŻīļź╝ ņ£äĒĢ£ TIPS ļ░░ņ╣ś ļō▒ņØ┤ ņ׳ļŗż. ņØ┤ļ¤¼ĒĢ£ ņ╣śļŻīļōżņØĆ ņä£ļĪ£ ļ│æņÜ®ļÉśņ¢┤ ņé¼ņÜ®ļÉśĻĖ░ļÅä ĒĢśļ®░ ņŗ£ņłĀ Ēøä ĒĢŁņØæĻ│ĀņĀ£ ņé¼ņÜ®ņØä ļ│æĒ¢ēĒĢ£ļŗż.
ĻĖ░Ļ│äņĀü ĒśłņĀä ņĀ£Ļ▒░ņłĀ
ĻĖ░Ļ│äņĀü ĒśłņĀä ņĀ£Ļ▒░ņłĀņØś ņĀĢĒÖĢĒĢ£ ņĀüņØæņ”ØņØ┤ ņ׳ņ¦ĆļŖö ņĢŖņ¦Ćļ¦ī, ĻĖ░Ļ│äņĀü ĒśłņĀä ņĀ£Ļ▒░ņłĀņØĆ ĒĢŁņØæĻ│ĀņĀ£ ņé¼ņÜ®ņØ┤ ĻĖłĻĖ░ļÉ£ Ļ▓ĮņÜ░ļéś ņןĻ░äļ¦ē ĒŚłĒśłņØ┤ ļÅÖļ░śļÉ£ Ļ▓ĮņÜ░ Ēś╣ņØĆ ņĀüņĀłĒĢ£ ĒĢŁņØæĻ│ĀņĀ£ ņé¼ņÜ®ņŚÉļÅä ĒśłņĀäņ”ØņØ┤ ņ¦äĒ¢ēļÉĀ Ļ▓ĮņÜ░ņŚÉ ņŗ£ļÅäļź╝ Ļ│ĀļĀżĒĢ┤ ļ│╝ ņłś ņ׳ļŗż. ņØ╝ļ░śņĀüņ£╝ļĪ£ ĻĖ░Ļ│äņĀü ĒśłņĀä ņĀ£Ļ▒░ņłĀņØĆ ņ╣┤ĒģīĒä░ ņ£ĀļÅä ĒśłņĀä ņÜ®ĒĢ┤ņĀ£ņÖĆ ĒĢ©Ļ╗ś ņŗ£Ē¢ēļÉśļŖöļŹ░, ņØ┤ļŖö ņØ┤ļĪĀņĀüņ£╝ļĪ£ ĒśłņĀäņØś ņ¢æņØä ņżäņŚ¼ ĒśłņĀä ņÜ®ĒĢ┤ņĀ£ ņÜöĻĄ¼ļ¤ēņØ┤ Ļ░ÉņåīļÉśĻ│Ā ņØ┤ļĪ£ ņØĖĒĢ┤ ņČ£Ēśł ņ£äĒŚśņØ┤ Ļ░ÉņåīĒĢśĻĖ░ ļĢīļ¼ĖņØ┤ļŗż. ĒØöĒ׳ ņØ┤ņÜ®ļÉśļŖö ĻĖ░Ļ│äņĀü ĒśłņĀä ņĀ£Ļ▒░ņłĀņŚÉļŖö ņ£Āņ▓┤ņŚŁĒĢÖņĀü ĒśłņĀä ņĀ£Ļ▒░ņłĀ(ĒØĪņØĖņØä ĒåĄĒĢ£ ĒśłņĀä ņÜ®ĒĢ┤)Ļ│╝ ĒÆŹņäĀ ĒśłņĀä ņĀ£Ļ▒░ņłĀ, ĒØĪņØĖ ņןņ╣śļź╝ ĒåĄĒĢ£ ĒśłņĀä ņĀ£Ļ▒░ņłĀņØ┤ ņ׳ļŗż. ĒśłņĀä ņĀ£Ļ▒░ņłĀņØä ņ£äĒĢ┤ ļ¼Ėļ¦ź ņĀĢļ¦źĻ│äļĪ£ ņĀæĻĘ╝ĒĢśĻĖ░ ņ£äĒĢ£ ļ░®ļ▓Ģņ£╝ļĪ£ļŖö Ļ▓ĮĻ▓ĮņĀĢļ¦ź Ļ▓ĮļĪ£, Ļ▓ĮĻ░äņĀü Ļ▓ĮļĪ£ Ēś╣ņØĆ Ļ▓ĮĒö╝ņĀü Ļ▓ĮļĪ£ ĻĘĖļ”¼Ļ│Ā Ļ▓Įļ╣äņĀü Ļ▓ĮļĪ£ļĪ£ ņĀæĻĘ╝ĒĢśļŖö ļ░®ļ▓ĢņØ┤ ņ׳ļŗż[61,62].
ņØ╝ļ░śņĀüņ£╝ļĪ£ ĻĖ░Ļ│äņĀü ĒśłņĀä ņĀ£Ļ▒░ņłĀņŚÉ ņé¼ņÜ®ļÉśļŖö ĒśłņĀä ņĀ£Ļ▒░ ņןņ╣ś ņżæ ĒĢśļéśļŖö AngioJet (Boston Scientific, Marlborough, MA, USA)ņ£╝ļĪ£, ņØ┤ļŖö ĒśłņĀäņØä ņŚ░ĒÖöņŗ£ĒéżĻ│Ā ņ£ĀļÅÖņä▒ ĒÜ©Ļ│╝ļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ņĀ£Ļ▒░ĒĢśļŖö ņĢĮļ”¼ĒĢÖņĀü ĒśłņĀä ņĀ£Ļ▒░ ņןņ╣śņØ┤ļŗż. ļ¼Ėļ¦źņØś Ēü¼ĻĖ░ļź╝ Ļ│ĀļĀżĒĢĀ ļĢī 8 FrĻ░Ć ņĀ£ņØ╝ ļ¦ÄņØ┤ ņō░ņØĖļŗż. ĒśłņĀä ņĪ░Ļ░üņØĆ ņ╣┤ĒģīĒä░ ļé┤Ļ░ĢņØä ĒåĄĒĢ┤ Ļ│ĀņåŹļÅäļĪ£ ĒØĪņ×ģļÉśņ¢┤ ļ░░ņČ£ļÉ£ļŗż[63,64]. ņØ┤ļ¤░ ĒśłņĀä ņĀłņĀ£ņłĀņØä ņŗ£Ē¢ēĒĢśĻĖ░ ņĀäņŚÉ tPAļź╝ ņé¼ņÜ®ĒĢśĻ▒░ļéś AngioJetņØä power pulse modeņŚÉņä£ ņé¼ņÜ®ĒĢśņŚ¼ ĒśłņĀä ļé┤ ĒśłņĀä ņÜ®ĒĢ┤ņĀ£ļź╝ ļČäņé¼ĒĢĀ ņłś ņ׳ļŗż. ņØ┤ļ¤¼ĒĢ£ ĻĖ░Ļ│äņĀü ĒśłņĀä ņĀ£Ļ▒░ļŖö ĒøäņåŹ ĒśłņĀä ņÜ®ĒĢ┤ņŚÉ ĒĢäņÜöĒĢ£ ņÜ®ĒĢ┤ņĀ£ņØś ņÜ®ļ¤ēĻ│╝ ņŻ╝ņ×ģ ņŗ£Ļ░äņØä ņżäņŚ¼ ņČ£Ēśł ņ£äĒŚśņØä ņżäņŚ¼ ĒÖśņ×ÉņØś ĒÜīļ│ĄņŚÉ ļÅäņøĆņØä ņżĆļŗż[64,65].
ĒØĪņØĖ ĒśłņĀä ņĀłņĀ£ņłĀņØĆ ļīĆņÜ®ļ¤ēņØś Ļ│ĀņĢĢ ņŻ╝ņé¼ĻĖ░ņÖĆ ĻĄ¼ļ®ŹņØ┤ Ēü░ ņ╣┤ĒģīĒä░ļź╝ ņé¼ņÜ®ĒĢśļŗżĻ░Ć ņ¦äĻ│Ą ļ│┤ņĪ░ ņŗ£ņŖżĒģ£ņ£╝ļĪ£ ļ░£ņĀäĒĢśņśĆļŗż. Indigo ĒØĪņØĖ ĒśłņĀä ņĀłņĀ£ņłĀ ņŗ£ņŖżĒģ£(Penumbra, Alameda, CA, USA)ņØĆ ņŗĀĻ▓ĮĒśłĻ┤Ć ļ░Å ļ¦Éņ┤ł ņØæņÜ® ļČäņĢ╝ņŚÉņä£ ņ×ÉņŻ╝ ņé¼ņÜ®ļÉśļŖö ņŚ░ņåŹ ĒØĪņ×ģ ņןņ╣śļĪ£ 8 FrĻ░Ć ļ¼Ėļ¦ź ņĀĢļ¦źĻ│äņŚÉņä£ Ļ░Ćņן ņØ╝ļ░śņĀüņ£╝ļĪ£ ņé¼ņÜ®ļÉ£ļŗż. ņØ┤ ņןņ╣śļź╝ ņé¼ņÜ®ĒĢśļ®┤ ņ╣┤ĒģīĒä░ ĒīüņØ┤ ĒśłņĀäĻ│╝ ļ¦×ļ¼╝ļ”¼ņ¦Ć ņĢŖņ£╝ļ®┤ņä£ ļŗ©ĻĖ░Ļ░äņŚÉ ņāüļŗ╣ĒĢ£ ņ¢æņØś ĒśłņĢĪ ņåÉņŗżņØ┤ ļ░£ņāØĒĢĀ ņłś ņ׳ņ¦Ćļ¦ī ņ×ÉļÅÖ ļ░ĖļĖī ņĀ£ņ¢┤ļź╝ ņé¼ņÜ®ĒĢśļ®┤ ĒśłņĀä ĒØĪņØĖņØ┤ ņĄ£ņĀüĒÖöļÉśĻ│Ā ĒśłņĢĪ ņåÉņŗż ņ£äĒŚśņØ┤ ņżäņ¢┤ļōĀļŗż. ņØ┤ļ¤░ ņ╣┤ĒģīĒä░ ņŗ£ņŖżĒģ£ņŚÉļŖö Ēü░ ņĀæĻĘ╝ ļŹ«Ļ░£Ļ░Ć ĒĢäņÜöĒĢśļ®░ ļ¼Ėļ¦ź ņĀĢļ¦źĻ│äņŚÉ ļīĆĒĢ£ ņĀæĻĘ╝ņ£╝ļĪ£ TIPSļź╝ ņé¼ņÜ®ĒĢĀ ņłś ņŚåļŖö Ļ▓ĮņÜ░ļŖö ņé¼ņÜ®ĒĢĀ ņłś ņŚåļŗż[66].
ņ╣┤ĒģīĒä░ ņ£ĀļÅä ĒśłņĀä ņÜ®ĒĢ┤ņłĀ
ņ╣┤ĒģīĒä░ ņ£ĀļÅä ĒśłņĀä ņÜ®ĒĢ┤ņłĀņØĆ ĻĖ░Ļ│äņĀü ĒśłņĀä ņĀ£Ļ▒░ņłĀĻ│╝ ļ│æĒ¢ēĒĢśņŚ¼ ņŗ£Ē¢ēļÉśļ®░ ĒśłņĀä ņÜ®ĒĢ┤ ņĢĮļ¼╝ņØä ĒśłņĀäņØ┤ ņ׳ļŖö ĒśłĻ┤ĆņŚÉ ņ¦üņĀæ ņŻ╝ņ×ģĒĢśņŚ¼ ņŗ£Ē¢ēĒĢ£ļŗż. Ļ░äļ¼Ėļ¦źņŚÉļŖö Ļ▓ĮĻ▓ĮņĀĢļ¦ź Ļ▓ĮļĪ£ļéś Ļ▓ĮĒö╝ņĀü Ļ▓ĮļĪ£ ĻĘĖļ”¼Ļ│Ā Ļ▓ĮĻ░ä Ļ▓ĮļĪ£ļź╝ ĒåĄĒĢ┤ ņĀæĻĘ╝ĒĢśņŚ¼ ĒśłņĀäņØ┤ ņ׳ļŖö Ļ││ņŚÉ ņŻ╝ņ×ģ ņ╣┤ĒģīĒä░ļź╝ ļ░░ņ╣śĒĢ£ļŗż. ņØ┤Ēøä ĒśłņĀäņØ┤ ņ׳ļŖö ĒśłĻ┤ĆņŚÉ ĒŖ╣ņĀĢ ņåŹļÅäļĪ£ ņä¼ņ£Āņåī ņÜ®ĒĢ┤ņĀ£(alteplase)ļź╝ ļČäņé¼ĒĢśļŖöļŹ░, ņŻ╝ņ×ģ ņåŹļÅäņÖĆ ņŻ╝ņ×ģ ņŗ£Ļ░äņØĆ ĒśłņĀäļ¤ēņŚÉ ļö░ļØ╝ ļŗżļź┤ņ¦Ćļ¦ī, ņØ╝ļ░śņĀüņ£╝ļĪ£ ņĄ£ļīĆ 24ņŗ£Ļ░ä ļÅÖņĢł 1 mg/hrņØś ņåŹļÅäļĪ£ ņŻ╝ņ×ģļÉ£ļŗż. ĻĘĖ ļÅÖņĢł ĒÖśņ×ÉļŖö ņżæĒÖśņ×ÉņŗżņŚÉņä£ ņČ£Ēśł ņ¦ĢĒøäĻ░Ć ņ׳ļŖöņ¦Ć ļ¬©ļŗłĒä░ļ¦üĒĢśļ®░ ņä¼ņ£Āņåī ņÜ®ĒĢ┤ņĀ£ļź╝ ņŻ╝ņ×ģĒĢ£ļŗż. ņØ┤ļĢī Ēśłņ▓Ł fibrinogen level, coagulation factor, hemoglobin ņłśņ╣śņŚÉ ļīĆĒĢ£ ĒśłņĢĪĒĢÖņĀü ļ¬©ļŗłĒä░ļ¦üļÅä ļ│æĒ¢ēĒĢ£ļŗż. ĻĖ░Ļ│äņĀü ĒśłņĀä ņĀłņĀ£ņłĀĻ│╝ ĒśłņĀä ņÜ®ĒĢ┤ņłĀ ņŗ£Ē¢ē ņØ┤Ēøä ĒÖśņ×ÉļŖö ĒĢŁņØæĻ│ĀņĀ£ļź╝ ņé¼ņÜ®ĒĢ┤ņĢ╝ ĒĢśļ®░, ĒśłņĀäņ”ØņØś ņ×¼ļ░£ ņŚ¼ļČĆļź╝ ĒÅēĻ░ĆĒĢśĻĖ░ ņ£äĒĢ┤ ņŻ╝ĻĖ░ņĀüņ£╝ļĪ£ ņśüņāü Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢ┤ņĢ╝ ĒĢ£ļŗż[67].
TIPS ļ░░ņ╣ś
TIPS ļ░░ņ╣śļŖö ņŻ╝ļĪ£ ĻĖ░Ļ│äņĀü ĒśłņĀä ņĀ£Ļ▒░ņłĀņØ┤ļéś ĒÖöĒĢÖņĀü ĒśłņĀä ņÜ®ĒĢ┤ņłĀ ņØ┤ĒøäņŚÉ ņŗ£Ē¢ēļÉ£ļŗż. ĒśłņĀä ņĀ£Ļ▒░ņłĀĻ│╝ ņÜ®ĒĢ┤ņłĀņØ┤ ĻĖēņä▒ĻĖ░ ĒśłņĀäņØĆ ņÜ®ĒĢ┤ĒĢśņ¦Ćļ¦ī ĻČüĻĘ╣ņĀüņ£╝ļĪ£ Ļ░ä ļé┤ ĒśłĻ┤ĆņĀĆĒĢŁņØä ņ”ØĻ░Ćņŗ£ĒéżĻ│Ā ĻĘ╝ļ│ĖņĀüņØĖ ļ¼ĖņĀ£ņØĖ ņŻ╝ ļ¼Ėļ¦źņØś ļŖÉļĀżņ¦ä ĒśłļźśļŖö ĒĢ┤Ļ▓░ĒĢśņ¦Ć ļ¬╗ĒĢśĻĖ░ ļĢīļ¼ĖņŚÉ TIPSļź╝ ļ░░ņ╣śĒĢśņŚ¼ ņŻ╝ ļ¼Ėļ¦źņØś ņĢĢļĀźņØä Ļ░Éņåīņŗ£ĒéżĻ│Ā ņĀĢņ▓┤ņŚåņØ┤ ĒśłņĢĪņØ┤ ĒØÉļź┤Ļ▓ī ĒĢ£ļŗż[68]. ĻĖ░Ļ│äņĀü ĒśłņĀä ņĀ£Ļ▒░ņłĀņØ┤ļéś ĒÆŹņäĀ ņĀĢļ¦ź ņä▒ĒśĢņłĀņØĆ TIPS ļ░░ņ╣ś ņĀäņŚÉ ņŗ£Ē¢ēĒĢśļÅäļĪØ ĻČīņ£ĀļÉ£ļŗż. TIPS ļ░░ņ╣ś ĒøäņŚÉļŖö Ļ░äļ¼Ėļ¦źņ£╝ļĪ£ ņĀüņĀłĒĢ£ ņ£ĀņåŹņØ┤ ņ£Āņ¦ĆļÉśļŖöņ¦Ć ĒÖĢņØĖĒĢśĻ│Ā, ļ╣äņן-ļ¼Ėļ¦ź ņĀĢļ¦ź ņĪ░ņśüņłĀņØä ņŗ£Ē¢ēĒĢśņŚ¼ ņĀĢļ¦źļźś ņ£Āļ¼┤ļź╝ ĒÅēĻ░ĆĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż. ļ¦īņĢĮņŚÉ TIPS ļ░░ņ╣śļź╝ ĒĢśņŚ¼ ņĀüņĀłĒĢ£ ļ¼Ėļ¦ź-ņĀäņŗĀ ņĢĢļĀźņØ┤ ĒśĢņä▒ļÉ£ ņØ┤ĒøäņŚÉļÅä ņĀĢļ¦źļźśĻ░Ć ņ׳ņ£╝ļ®┤ ņāēņĀäņłĀņØä ņŗ£Ē¢ēĒĢśļŖö Ļ▓āļÅä Ļ│ĀļĀżĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż.
ņĄ£ĻĘ╝ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉ ļö░ļź┤ļ®┤ Ļ░äĻ▓Įļ│Ćņ”ØĻ│╝ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØ┤ ļÅÖļ░śļÉśņ¢┤ ņ׳ļŖö ĒÖśņ×ÉņŚÉņä£ ļŗżņØīĻ│╝ Ļ░ÖņØĆ Ļ▓ĮņÜ░ņŚÉ TIPS ļ░░ņ╣śļź╝ ĒĢśļŖö Ļ▓āņØä Ļ│ĀļĀżĒĢśļÅäļĪØ ņČöņ▓£ĒĢśĻ│Ā ņ׳ļŗż[57]: (1) ĒĢŁņØæĻ│ĀņĀ£ņØś ĒÜ©Ļ│╝Ļ░Ć ņŚåĻ▒░ļéś ĒĢŁņØæĻ│ĀņĀ£ ņé¼ņÜ®ņØ┤ ĻĖłĻĖ░ņŗ£ļÉ£ Ļ▓ĮņÜ░, (2) ļé┤Ļ│╝ņĀü ņ╣śļŻīņŚÉ ļ░śņØæĒĢśņ¦Ć ņĢŖļŖö ļ¼Ėļ¦ź Ļ│ĀĒśłņĢĢĻ│╝ Ļ┤ĆļĀ©ļÉ£ ĒĢ®ļ│æņ”ØņØä ļÅÖļ░śĒĢ£ ļ¦īņä▒ Ļ░äļ¼Ėļ¦ź ĒśłņĀä/ĒĢ┤ļ®┤ņāü ļ│ĆĒśĢ, (3) ņØ┤ņŗØļÉ£ Ļ░äņĀĢļ¦ź ņé¼ņØ┤ņŚÉ ņāØļ”¼ņĀü ļ¼ĖĒĢ®ļČĆņØś ĒØÉļ”äņØä ļ░®ĒĢ┤ĒĢśļŖö ļ¦īņä▒ Ļ░äļ¼Ėļ¦ź ĒśłņĀä.
TIPS ļ░░ņ╣śņÖĆ ĒĢŁņØæĻ│ĀņĀ£ņØś ĒÜ©ņÜ®ņä▒ņŚÉ ļīĆĒĢ£ ļ®öĒāĆļČäņäØņØä ļ│┤ļ®┤ 179ļ¬ģņØś ĒĢŁņØæĻ│ĀņĀ£ ņé¼ņÜ® ĒÖśņ×ÉĻĄ░Ļ│╝ 148ļ¬ģņØś TIPS ļ░░ņ╣ś ĒÖśņ×ÉĻĄ░ ļ¬©ļæÉ ļīĆņĪ░ĻĄ░ņŚÉ ļ╣äĒĢ┤ņä£ ļåÆņØĆ ņ×¼Ļ┤Ćļźśņ£©ņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż[69]. ĻĘĖļ¤¼ļéś TIPS ļ░░ņ╣śĻĄ░ņŚÉņä£ ĒĢŁņØæĻ│ĀņĀ£ ņé¼ņÜ®ĻĄ░ļ│┤ļŗż ņé¼ļ¦ØļźĀ Ļ░£ņäĀņØś ĒÜ©Ļ│╝ļŖö ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż. ņØ┤Ļ▓āņ£╝ļĪ£ ļ│┤ņĢśņØä ļĢī, Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØ┤ ņ׳ļŖö ĒÖśņ×ÉņŚÉņä£ ņĀĢļ¦źļźś ņśłļ░®ņØä ņ£äĒĢ┤ņä£ 1ņ░©ņĀüņ£╝ļĪ£ ĒĢŁņØæĻ│ĀņĀ£ļź╝ Ēł¼ņŚ¼ļ░øļŖö Ļ▓āņØ┤ ĒĢäņÜöĒĢśļ®░, ņØ┤ļ¤░ ĒĢŁņØæĻ│ĀņĀ£ ņ╣śļŻīņŚÉ ĒÜ©Ļ│╝Ļ░Ć ņŚåĻ▒░ļéś ĻĖłĻĖ░ņé¼ĒĢŁņØĖ Ļ▓ĮņÜ░ 2ņ░© ņ╣śļŻīļĪ£ TIPSļź╝ Ļ│ĀļĀżĒĢ┤ ļ│╝ ņłś ņ׳ļŖö Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż[38,70].
Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņŚÉņä£ TIPS ļ░░ņ╣śņØś ņĢłņĀäņä▒Ļ│╝ ĒÜ©ņÜ®ņä▒ņØä ĒÅēĻ░ĆĒĢśļŖö ļīĆĻĘ£ļ¬© ĒøäĒ¢źņĀü ņŚ░ĻĄ¼ņŚÉņä£ TIPS ļ░░ņ╣śņØś 100% ĻĖ░ņłĀņĀü ņä▒Ļ│ĄļźĀņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż. TIPSļź╝ ņŗ£Ē¢ēĒĢ£ ĒÖśņ×É 70ļ¬ģ ņżæ 40ļ¬ģ(57%)ņŚÉņä£ ļ¼Ėļ¦źņØś ņÖäņĀä Ļ░£ĒåĄņØ┤ ņØ┤ļŻ©ņ¢┤ņĪīĻ│Ā ļČĆļČä Ļ░£ĒåĄņØ┤ 21ļ¬ģ(30%)ņŚÉņä£ Ļ┤Ćņ░░ļÉśņŚłņ£╝ļ®░ Ļ░£ņäĀļÉśņ¦Ć ņĢŖņØĆ ĒÖśņ×ÉļŖö 9ļ¬ģ(13%)ņØ┤ņŚłļŗż. ĒÅēĻĘĀ 20.7Ļ░£ņøöņØś ņČöņĀü Ļ┤Ćņ░░ ĻĖ░Ļ░ä ļÅÖņĢł 38ļ¬ģ(95%)ņŚÉņä£ ļ¼Ėļ¦ź Ļ░£ĒåĄņØ┤ ņ£Āņ¦ĆļÉśņŚłņ£╝ļ®░, 6Ļ░£ņøö ļÅÖņĢł 2ļ¬ģ(5%)Ļ│╝ 26Ļ░£ņøö ļÅÖņĢł 1ļ¬ģņŚÉĻ▓īņä£ ņ×¼ĒśłņĀäņ”ØņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż. 38ļ¬ģņØś ĒÖśņ×É ņżæ 17ļ¬ģ(45%)ņŚÉņä£ ņäĀņ▓£ņä▒ ĒśłņĀäņØĖņ×ÉņØś ļåÆņØĆ ļ░£ņāØļźĀņŚÉ ļö░ļźĖ Ļ│╝ņØæĻ│Ā ņāüĒā£ņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā ļåÆņØĆ Ļ░£ĒåĄļźĀĻ│╝ Ļ░£ĒåĄņä▒ņØ┤ ņ£Āņ¦ĆļÉśņŚłļŗż. ņØ┤ļ¤¼ĒĢ£ Ļ▓░Ļ│╝ļź╝ ĒåĄĒĢ┤ ļåÆņØĆ Ļ░ä ļé┤ ļ¼Ėļ¦źņĢĢņØä ņÜ░ĒÜīĒĢśņŚ¼ ĒØÉļ”äņØä Ļ░£ņäĀĒĢ©ņ£╝ļĪ£ņŹ© ļ¼Ėļ¦ź Ļ░£ĒåĄņä▒ņØä ņ£Āņ¦ĆĒĢśĻĖ░ ņ£äĒĢ£ TIPS ļ░░ņ╣śņØś ĒÜ©ņÜ®ņä▒ņØä ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłļŗż[68].
ĻĘĖļ¤¼ļéś ņĢäņ¦ü TIPS ļ░░ņ╣śļź╝ ņ×äņāüņĀü ņ”ØņāüņØ┤ ņŚåļŖö Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņŚÉņä£ ņŗ£Ē¢ēĒĢ┤ņĢ╝ ĒĢśļŖöņ¦ĆņŚÉ ļīĆĒĢ£ ļīĆļŗĄņØĆ ĒÖĢņŗżņ╣ś ņĢŖņØĆ ņāüĒÖ®ņØ┤ļŗż. ņŚ¼ļ¤¼ ĒøäĒ¢źņĀü ņŚ░ĻĄ¼ņŚÉņä£ TIPSņØś ņĢłņĀĢņä▒Ļ│╝ ĒÜ©ņÜ®ņä▒ņØ┤ ņ”Øļ¬ģļÉ£ ļ░ö ņ׳ņ¦Ćļ¦ī, ļīĆņĪ░ĻĄ░ņØś ļČĆņ×¼ļĪ£ ņØĖĒĢ┤ ņĀĢĒÖĢĒĢ£ ļ╣äĻĄÉļŖö ņŗ£Ē¢ēļÉśņ¦Ć ņĢŖņĢśĻĖ░ ļĢīļ¼ĖņØ┤ļŗż.
TIPSņØś ļČĆņ×æņÜ®ņ£╝ļĪ£ Ļ░äņä▒ļćīņ”ØņØś ņ£äĒŚśņØ┤ ņ”ØĻ░ĆĒĢ£ļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ļŗż. ĻĘĖļ¤¼ļéś Ļ░äĻ▓Įļ│Ćņ”ØņŚÉņä£ ļÅÖļ░śļÉ£ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”Ø ĒÖśņ×ÉņŚÉņä£ ņĀĢļ¦źļźś ņČ£ĒśłņØś ņśłļ░®ņØä ņ£äĒĢ£ TIPS ļ░░ņ╣śņŚÉ Ļ┤ĆĒĢ£ ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤ ĻĖ░ņĪ┤ņØś ņ╣śļŻīņŚÉ ļ╣äĒĢ┤ TIPS ļ░░ņ╣śĻ░Ć ņé¼ļ¦ØļźĀņŚÉ ņ׳ņ¢┤ ņ£ĀņØśĒĢ£ Ļ░£ņäĀņØä ļ│┤ņØ┤ņ¦ä ļ¬╗Ē¢łņ¦Ćļ¦ī Ļ░äņä▒ļćīņ”ØņØś ņ£äĒŚśņä▒ņØä ņ”ØĻ░Ćņŗ£Ēéżņ¦Ć ņĢŖņĢśļŗżļŖö ļ│┤Ļ│ĀĻ░Ć ņ׳ņŚłļŗż[71,72].
ĒĢ┤ļ®┤ņāü ļ│ĆĒśĢņØ┤ ņ׳ļŖö ļ¦īņä▒ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”Ø
ļ¦īņĢĮ ĻĖēņä▒ĻĖ░ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØä ņ╣śļŻīĒĢśņ¦Ć ņĢŖĻ│Ā ļ░®ņ╣śĒĢśļ®┤ ļ¦ī ņä▒ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØ┤ ļÉĀ ņłś ņ׳ņ£╝ļ®░, ļŹö ņ¦äĒ¢ēļÉśļ®┤ ĒĢ┤ļ®┤ņāü ļ│ĆĒśĢņŚÉ ņØ┤ļź┤Ļ▓ī ļÉ£ļŗż. ĒśłņĀä ļČĆņ£ä ņØ┤ņĀäņØś ļ¼Ėļ¦źĒśłļźśļź╝ Ļ░äņ£╝ļĪ£ ņÜ┤ļ░śĒĢśĻĖ░ ņ£äĒĢśņŚ¼ ļ¼Ėļ¦ź ņŻ╝ļ│ĆņØś ņĖĪļČĆ ĒśłĻ┤ĆļōżņØś ņ¦üĻ▓ĮņØ┤ ĒÖĢņןļÉśĻ│Ā ĒÅÉņāēļÉ£ ļ¼Ėļ¦ź ņŻ╝ļ│Ćņ£╝ļĪ£ ņÜ░ĒÜīĒĢśņŚ¼ ņŻ╝Ē¢ēĒĢśĻ▓ī ļÉśļŖöļŹ░, ņØ┤ļ¤¼ĒĢ£ ļ│ĆĒśĢ ļÉ£ ĻĄ¼ņĪ░ ņĀäņ▓┤ļź╝ ĒĢ┤ļ®┤ņāü ļ│ĆĒśĢņØ┤ļØ╝Ļ│Ā ĒĢ£ļŗż. ņØ┤ Ļ▓ĮņÜ░ ņ×äņāüņĀüņ£╝ļĪ£ ņŗØļÅäļéś ņ£äņĀĢļ¦źļźśņØś ļīĆļ¤ē ņČ£ĒśłņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ņ£╝ļ®░ ļČłņØæņä▒ ļ│Ąņłśļéś ĒØēņłś ļśÉĒĢ£ ņāØĻĖĖ ņłś ņ׳ļŗż. ĻĘĖļ¤¼ļéś ņĀüņĀłĒĢ£ ņÜ░ĒÜī ņł£ĒÖśņØ┤ ņ׳ļŖö ĒÖśņ×ÉļōżņØś Ļ▓ĮņÜ░ ļ¼┤ņ”Øņāüņ£╝ļĪ£ ļéśĒāĆļéĀ ņłś ņ׳ļŗż.
ņØ┤ļ¤░ ļ¦īņä▒ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”Ø ĒÖśņ×ÉļōżņŚÉĻ▓ī ņŻ╝ļĪ£ Ļ▓Įļ╣äņĀü Ļ▓ĮļĪ£ļéś Ļ▓ĮĻ░äņĀü Ļ▓ĮļĪ£ļź╝ ĒåĄĒĢ£ Ļ░äļ¼Ėļ¦źņØś ņ×¼Ļ┤ĆļźśņÖĆ TIPS ļ░░ņ╣śĻ░Ć ņØ┤ņÜ®ļÉśĻ│ż ĒĢ£ļŗż. Ļ░ä ņØ┤ņŗØ ĒøäņŚÉ ļ¦īņä▒ņĀüņ£╝ļĪ£ Ļ░äļ¼Ėļ¦źņØ┤ ļ¦ēĒ×ī ĒÖśņ×ÉņŚÉĻ▓īļŖö ņ×¼Ļ┤Ćļźśļź╝ ņ£äĒĢ┤ TIPS ļ░░ņ╣śļź╝ ĒĢĀ Ļ▓ĮņÜ░ ļ¼Ėļ¦źĻ│ä ĒśłĻ┤Ć ņł£ĒÖśņØä ļ│ĄĻĄ¼ĒĢśļŖö Ļ▓āĻ│╝ Ļ░ä-ņĀäņŗĀ ļ¼ĖĒĢ®ļČĆ ĻĖ░ļŖźņØä ņĀĢņāüņ▓śļ¤╝ ņ£Āņ¦ĆĒĢśĻ▓ī ĒĢśļŖö ļŹ░ņŚÉ ļÅäņøĆņØä ņżä ņłś ņ׳ļŗż[38].
Ļ▓░ ļĪĀ
Ļ░äĻ▓Įļ│Ćņ”Ø ĒÖśņ×ÉņØś Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”ØņØĆ ņĄ£ĻĘ╝ ļōżņ¢┤ ņĀÉņĀÉ ļŹö ļ¦ÄņØ┤ ņØĖņŗØļÉśĻ│Ā ņ׳ņ£╝ļéś ņłśļ¦ÄņØĆ ļ│ĆņłśĻ░Ć ņ׳ņ¢┤ ņ╣śļŻī ļ░®ļ▓ĢņØ┤ ļ│Ąņ×ĪĒĢ£ ĒÄĖņØ┤ļŗż. ĻĘĖņżæ ĒĢŁņØæĻ│Ā ņÜöļ▓ĢņØĆ ĻĖēņä▒ Ļ░äļ¼Ėļ¦ź ĒśłņĀäņ”Ø ĒÖśņ×ÉņŚÉņä£ ņĀĢļ¦źļźś ņČ£ĒśłņØ┤ļéś ņןĻ░äļ¦ē ĒŚłĒśłņØ┤ ņŚåļŖö Ļ▓ĮņÜ░ 1ņ░© ņ╣śļŻīļĪ£ ņō░ņØ╝ ņłś ņ׳ņØä Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż. ņé¼ņÜ® Ļ░ĆļŖźĒĢ£ ņĄ£ņåī ņ╣©ņŖĄ ņ╣śļŻīļ▓ĢņŚÉļŖö ĻĖ░Ļ│äņĀü ĒśłņĀä ņĀ£Ļ▒░ņłĀ, ĒÖöĒĢÖņĀü ĒśłņĀä ņÜ®ĒĢ┤ņłĀ ļ░Å TIPS ļ░░ņ╣ś ļō▒ņØś ļ░®ļ▓ĢņØ┤ ņ׳ļŗż. ĻĘĖļ¤¼ļéś ņĢäņ¦ü ļ¼┤ņ×æņ£ä ļīĆņĪ░ ņŚ░ĻĄ¼ ņłśņżĆņØś ĻĘ╝Ļ▒░Ļ░Ć ļČĆņĪ▒ĒĢśĻ│Ā, ņŚ░ĻĄ¼ ļŹ░ņØ┤Ēä░ļōżņØś ņāüņØ┤ĒĢ©ņ£╝ļĪ£ ņØĖĒĢ┤ ĒĢ®ņØśļÉ£ Ļ░ĆņØ┤ļō£ ļØ╝ņØĖņØä ļ¦īļōż ņłś ņŚåĻĖ░ ļĢīļ¼ĖņŚÉ ĒĢŁņØæĻ│ĀņĀ£ņÖĆ ņżæņ×¼ņĀü ņ╣śļŻīļ▓ĢņØś ņé¼ņÜ®ļ▓ĢĻ│╝ ĒāĆņØ┤ļ░ŹņØä ĒÅēĻ░ĆĒĢśĻĖ░ ņ£äĒĢ┤ņä£ ļŗżĻĖ░Ļ┤Ć ļ¼┤ņ×æņ£ä ņŚ░ĻĄ¼Ļ░Ć ĒĢäņÜöĒĢ£ ņŗżņĀĢņØ┤ļŗż.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






