


ņä£ ļĪĀ
Ļ┤ĆļÅÖļ¦źņ¦łĒÖśņ£╝ļĪ£ ĒĢŁĒśłņåīĒīÉņĀ£ļź╝ ņé¼ņÜ®ĒĢśļŖö ĒÖśņ×Éļōż ņżæ ņĢĮ 10%ļŖö ņŗ£ņłĀ Ēøä 1ļģä ļé┤ņŚÉ ļ╣äņŗ¼ņןņä▒ ņłśņłĀņØ┤ ĒĢäņÜöĒĢ£ Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[1,2]. ņØ┤ļōż ĒÖśņ×ÉņŚÉņä£ ņłśņłĀ ņĀäĒøä ĒĢŁĒśłņåīĒīÉņĀ£ļź╝ ņĪ░ĻĖ░ ņżæļŗ©ĒĢĀ Ļ▓ĮņÜ░ ĒĢäņŚ░ņĀüņ£╝ļĪ£ ņŗ¼ĒśłĻ┤Ćņ¦łĒÖś ļ░£ņāØņØś ņ£äĒŚśļÅäĻ░Ć ņāüņŖ╣ĒĢśĻ▓ī ļÉśļ»ĆļĪ£ ņŻ╝ņØśļź╝ ņÜöĒĢ£ļŗż[3-5]. ņØ┤ļŖö ĒĢŁĒśłņĀäņĀ£ ņżæļŗ©ņŚÉ ļö░ļźĖ ļ░śļÅÖ ĒÜ©Ļ│╝(rebound effect)ņŚÉ ņØśĒĢ£ ĒśłņĀä ņ£äĒŚś(thrombotic risk) ņ”ØĻ░ĆĻ░Ć ņŻ╝ ņøÉņØĖņØ┤ņ¦Ćļ¦ī ņłśņłĀ ņ×Éņ▓┤ļĪ£ ņØĖĒĢ£ ņŖżĒŖĖļĀłņŖżļéś ĻĄÉĻ░ÉņŗĀĻ▓ĮņØś ĒĢŁņ¦ä, ĒśłĻ┤Ć Ļ▓ĮļĀ© ļ░Å ņŻĮņāüĻ▓ĮĒÖöļ░śņŚÉ Ļ░ĆĒĢ┤ņ¦ĆļŖö ņĀäļŗ© ņØæļĀź(shear stress) ļō▒ņ£╝ļĪ£ ņØĖĒĢ┤ ĒśłņĀä ļ░£ņāØņØś ņ£äĒŚśļÅäĻ░Ć ļåÆņĢäņ¦äļŗż. ļśÉĒĢ£ ņłśņłĀ ņ×Éņ▓┤ļÅä ņŚ╝ņ”ØņØś ļ░£ņāØņØ┤ļéś ņØæĻ│ĀĻ│äņØś ĒÖ£ņä▒ĒÖöļź╝ ņĪ░ņןĒĢśĻ▓ī ļÉśļ»ĆļĪ£ ņŖżĒģÉĒŖĖĻ░Ć ņéĮņ×ģļÉ£ ĒśłĻ┤ĆĻ│╝ ņŖżĒģÉĒŖĖĻ░Ć ņéĮņ×ģļÉśņ¦Ć ņĢŖņØĆ ĒśłĻ┤Ć ļ¬©ļæÉņŚÉņä£ ĒśłņĀä ņé¼Ļ▒┤(thrombotic event)ņØ┤ ņ”ØĻ░ĆĒĢśĻ▓ī ļÉ£ļŗż[6-8].
Ēśäņ×¼ ĻĄŁĻ░Ćļ│ä ļ░Å ņ£ĀĻ┤Ć ĒĢÖĒÜī ļ│äļĪ£ ĒĢŁĒśłņĀäņĀ£ ņé¼ņÜ®ņ×ÉļōżņØś ļ╣äņŗ¼ņןņä▒ņłśņłĀ ņĀä ņ╣śļŻīņ¦Ćņ╣©ņØä ņĀ£ņŗ£ĒĢśĻ│Ā ņ׳ņ¦Ćļ¦ī ļŗżņØīĻ│╝ Ļ░ÖņØĆ ņĀ£ĒĢ£ņĀÉņØ┤ ņ׳ļŗż[9-14]. ņ▓½ņ¦Ė, ņŗ¼ņןļé┤Ļ│╝ņØś, ņÖĖĻ│╝ņØś ļ░Å ļ¦łņĘ©Ļ│╝ņØś ļ¬©ļæÉņØś Ļ│ĄĒåĄļÉ£ ņØśĻ▓¼ņØ┤ ļ░śņśüļÉ£ Ļ▓āņØ┤ ņĢäļŗłļ»ĆļĪ£ ņĀäĻ│ĄļČäņĢ╝ ļ│äļĪ£ ņ╣śļŻīņØś ĒåĄņØ╝ņØä ņØ┤ļŻ©ĻĖ░ Ēלļōżļŗż. ļæśņ¦Ė, ņłśņłĀ ņóģļ│äļĪ£ Ēæ£ņżĆĒÖöļÉ£ ĒśłņĀä ņ£äĒŚśņØä ņĀ£ņŗ£ĒĢśņ¦Ć ņĢŖĻ│Ā ņ׳ļŗż. ņģŗņ¦Ė, ĒÖśņ×É Ļ░£Ļ░£ņØĖņØś ņČ£Ēśł ņ£äĒŚś(bleeding risk)ņØä Ēæ£ņżĆĒÖöĒĢśņŚ¼ ņĀ£ņŗ£ĒĢśņ¦Ć ņĢŖĻ│Ā ņ׳ļŗż. ļäĘņ¦Ė, ņłśņłĀņØä ņŚ░ĻĖ░ĒĢĀ ņłś ņŚåņØä Ļ▓ĮņÜ░ļéś ņČ£Ēśł ņ£äĒŚśņØ┤ ļåÆņØĆ ņłśņłĀņØä ņŗ£Ē¢ē ĒĢ┤ņĢ╝ ĒĢĀ Ļ▓ĮņÜ░ ĒĢŁĒśłņĀäņĀ£ ņĪ░ņĀłņŚÉ Ļ┤ĆĒĢ£ ĻČīĻ│ĀņĢłņØ┤ ņŚåļŗż.
ļīĆļČĆļČäņØś Ēæ£ņżĆņ╣śļŻīņ¦Ćņ╣©ļōżņØĆ ļ╣äņŗ¼ņןņłśņłĀ ņŗ£ ņĢäņŖżĒö╝ļ”░ņØä ņżæļŗ©ņŚåņØ┤ ņé¼ņÜ®ĒĢĀ Ļ▓āņØä ĻČīņ£ĀĒĢśĻ│Ā ņ׳ņ¦Ćļ¦ī ņŗżņĀ£ ņ×äņāüņŚÉņä£ļŖö ņĢäņŖżĒö╝ļ”░ņØś ņżæļŗ©ņØ┤ ļ╣łļ▓łĒ׳ ņØ┤ļŻ©ņ¢┤ņ¦ĆĻ│Ā ņ׳ļŗż[15]. ļśÉĒĢ£ perioperative ischemic evaluation 2 (POISE-2) ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņŗ¼ĒśłĻ┤ĆĻ│ä ņ¦łĒÖśņØś ņ£äĒŚśņØ┤ ļåÆņØĆ ĒÖśņ×ÉņŚÉņä£ ļ╣äņŗ¼ņןņłśņłĀ ņĀä ņĢäņŖżĒö╝ļ”░ņØä ņé¼ņÜ®ĒĢśļŹöļØ╝ļÅä ņŻ╝ņÜöņŗ¼ņןņé¼Ļ▒┤(major adverse cardiovascular event, MACE)ņØś Ļ░Éņåī ĒÜ©Ļ│╝ ņŚåņØ┤ ņČ£Ēśł ņé¼Ļ▒┤(bleeding event)ļ¦ī ņ£ĀņØśĒĢśĻ▓ī ņ”ØĻ░Ćņŗ£Ēé©ļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż[16]. ļ░śļ®┤ņŚÉ, ņØ┤ ņŚ░ĻĄ¼ņØś ĒĢśņ£ä ļČäņäØņŚÉņä£ļŖö Ļ┤ĆļÅÖļ¦źņżæņ×¼ņłĀņØä ņŗ£Ē¢ēĒĢ£ ļ│æļĀźņØ┤ ņ׳ļŖö ĒÖśņ×ÉņŚÉņä£ ņĢäņŖżĒö╝ļ”░ņØä ņé¼ņÜ®ĒĢĀ Ļ▓ĮņÜ░ ņłśņłĀ Ēøä ņŗ¼ĻĘ╝Ļ▓Įņāēņ”Ø ļ░£ņāØņØä ņ£ĀņØśĒĢśĻ▓ī ņżäņØ┤ļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļéś ņŻ╝ ņŚ░ĻĄ¼ņÖĆļŖö ņāüļ░śļÉ£ Ļ▓░Ļ│╝ļź╝ ļ│┤ņŚ¼ņŻ╝Ļ│Ā ņ׳ļŗż[17]. ļśÉĒĢ£, ĒĢśļéś ņØ┤ņāüņØś ņŗ¼ĒśłĻ┤ĆĻ│ä ņ£äĒŚśņØĖņ×Éļź╝ Ļ░Ćņ¦ä 220ļ¬ģņØä ļīĆņāüņ£╝ļĪ£ ņŗ£Ē¢ēļÉ£ ļ¼┤ņ×æņ£ä ņŚ░ĻĄ¼ņŚÉņä£ ņłśņłĀ ņĀä ņĀĆņÜ®ļ¤ē ņĢäņŖżĒö╝ļ”░ņØä ņé¼ņÜ®ĒĢĀ Ļ▓ĮņÜ░ ņ£äņĢĮĻĄ░Ļ│╝ ļ╣äĻĄÉĒĢĀ ļĢī MACE ļ░£ņāØņØś ņāüļīĆņ£äĒŚśļÅäļź╝ 80% Ļ░Éņåīņŗ£ĒéżļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼Ļ│Ā ņČ£Ēśł ņ£äĒŚśņØĆ ņ”ØĻ░Ćņŗ£Ēéżņ¦Ć ņĢŖņĢśļŗż[18]. ņĢ×ņä£ ņ¢ĖĻĖēĒĢ£ ņāüļ░śļÉ£ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļōżļĪ£ ņØĖĒĢ┤ Ļ┤ĆļÅÖļ¦źņ¦łĒÖśņ£╝ļĪ£ ĒĢŁĒśłņåīĒīÉņĀ£ļź╝ ņé¼ņÜ® ņżæņØĖ ĒÖśņ×ÉņŚÉņä£ ļ╣äņŗ¼ņןņłśņłĀņØ┤ ĒĢäņÜöĒĢ£ Ļ▓ĮņÜ░ ņĢäņŖżĒö╝ļ”░ņØś ņé¼ņÜ®ņØä ļ░śļō£ņŗ£ ņ£Āņ¦ĆĒĢ┤ņĢ╝ ĒĢśļŖöņ¦ĆņŚÉ ļīĆĒĢ┤ņä£ļŖö ņŚ¼ņĀäĒ׳ ļģ╝ļ×ĆņØ┤ ņ¦ĆņåŹļÉśĻ│Ā ņ׳ļŗż.
ļīĆĒĢ£ņŗ¼ĒśłĻ┤Ćņżæņ×¼ĒĢÖĒÜī ņé░ĒĢś ĒśłņåīĒīÉ-ĒśłņĀä ņŚ░ĻĄ¼ĒÜīņŚÉņä£ļŖö ĒĢŁĒśłņĀäņĀ£ļź╝ ņé¼ņÜ® ņżæņØĖ ĒÖśņ×ÉņŚÉņä£ ļ╣äņŗ¼ņןņłśņłĀņØ┤ ĒĢäņÜöĒĢ£ Ļ▓ĮņÜ░ ņ×äņāüņŚÉņä£ ļ¦łņŻ╝ņ╣śĻ▓ī ļÉśļŖö ļ│Ąņ×ĪĒĢ£ ņāüĒÖ®ņŚÉ ļÅäņøĆņØä ņŻ╝ĻĖ░ ņ£äĒĢ┤ ņĢĮņĀ£ ņĪ░ņĀłņŚÉ Ļ┤ĆĒĢ£ ņĄ£ņŗĀ ņ¦ĆĻ▓¼Ļ│╝ ņŚ░ĻĄ¼ĒÜīņØś ņ×ģņןņØä ļīĆĒæ£ņĀüņØĖ ņ×äņāü ņ”ØļĪĆņÖĆ ĒĢ©Ļ╗ś ĻĖ░ņłĀĒĢśļĀż ĒĢ£ļŗż. ļ╣äņŖżĒģīļĪ£ņØ┤ļō£ ņåīņŚ╝ņĀ£ļź╝ ļ╣äļĪ»ĒĢ£ ļŗżņ¢æĒĢ£ ņĢĮņĀ£ļōżņØ┤ ņłśņłĀ ņĀäĒøä ĒśłņĀä ļ░Å ņČ£Ēśł ņ£äĒŚśļÅäņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣śņ¦Ćļ¦ī Ļ┤ĆļĀ© ņŚ░ĻĄ¼Ļ░Ć ņČ®ļČäĒĢśņ¦Ć ņĢŖņĢä ļ│Ė ĒĢ®ņØśļ¼ĖņŚÉņä£ļŖö ņāØļץĒĢśļÅäļĪØ ĒĢśĻ▓Āļŗż.
ļ│Ė ļĪĀ
ļ╣äņŗ¼ņןņłśņłĀĻ│╝ ņŚ░Ļ┤ĆļÉ£ ņ£äĒŚśļÅäņØś ĒÅēĻ░Ć
ĒĢŁĒśłņĀäņĀ£ļź╝ ņé¼ņÜ®ĒĢśļŖö ĒÖśņ×ÉļōżņØś ņłśņłĀ ņĀäĒøä ņ£äĒŚśļÅäļź╝ ĒÅēĻ░ĆĒĢśļŖö Ļ▓āņØĆ ļ¦żņÜ░ ļé£ĒĢ┤ĒĢ£ ņØ╝ņØ┤ļ®░ ĒŖ╣Ē׳ ņłśņłĀ ņĀä ĒĢŁĒśłņĀäņĀ£ņØś ņżæļŗ© ļśÉļŖö ņ¦ĆņåŹņŚÉ Ļ┤ĆĒĢ┤ņä£ļŖö ņŗ¼ņןļé┤Ļ│╝ņØśņÖĆ ņÖĖĻ│╝ņØś Ļ░äņØś ņØśĻ▓¼ ļČłņØ╝ņ╣śĻ░Ć ļ░£ņāØĒĢśļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äļŗż. ĒĢŁĒśłņĀäņĀ£ļź╝ ņé¼ņÜ® ņżæņØĖ ĒÖśņ×ÉĻ░Ć ņłśņłĀņØ┤ ĒĢäņÜöĒĢ£ Ļ▓ĮņÜ░ ņĢĮņĀ£ ņżæļŗ©ņ£╝ļĪ£ ņØĖĒĢ£ ņŗ¼ĒśłĻ┤ĆĻ│ä ņ£äĒŚśļÅäņØś ņ”ØĻ░Ć, ņłśņłĀņØä ņŚ░ĻĖ░ĒĢśņśĆņØä ļĢī ļ░£ņāØĒĢĀ ņłś ņ׳ļŖö ņ£äĒŚśļÅä, ĒĢŁĒśłņĀäņĀ£ļź╝ ņ£Āņ¦ĆĒĢśņśĆņØä ļĢī ļ░£ņāØĒĢĀ ņłś ņ׳ļŖö ņČ£ĒśłņØś ņ£äĒŚśļÅäļź╝ ļŗżļ®┤ņĀüņ£╝ļĪ£ ĒīÉļŗ©ĒĢśņŚ¼ņĢ╝ ĒĢśļ»ĆļĪ£ ņŗ¼ņןļé┤Ļ│╝ņØś, ņÖĖĻ│╝ņØś ļ░Å ļ¦łņĘ©Ļ│╝ņØś Ļ░äņØś ļŗżĒĢÖ ņĀ£ņ¦äļŻīļź╝ ĒåĄĒĢ┤ ņ╣śļŻī ņĀäļץņØä ņłśļ”ĮĒĢ┤ņĢ╝ ĒĢ£ļŗż. Ēśäņ×¼ ņé¼ņÜ®ļÉśĻ│Ā ņ׳ļŖö Ēæ£ņżĆņ╣śļŻīņ¦Ćņ╣©ņØś ļīĆļץņĀüņØĖ ņøÉņ╣ÖņØĆ ļŗżņØīĻ│╝ Ļ░Öļŗż[10,13]. ņ▓½ņ¦Ė, ņØ┤ņżæĒĢŁĒśłņåīĒīÉņÜöļ▓Ģ(dual antiplatelet therapy, DAPT)ņØś ĒĢäņłś ņé¼ņÜ®ĻĖ░Ļ░ä ļÅÖņĢł ļ╣äņØæĻĖēņłśņłĀ(elective surgery)ņØĆ ņŚ░ĻĖ░ĒĢ£ļŗż. ļæśņ¦Ė, ņłśņłĀ Ēøä ņ¦ĆĒśłņØ┤ ĒלļōĀ Ļ▓ĮņÜ░ ņÖĖņŚÉļŖö ņĢäņŖżĒö╝ļ”░ņØĆ ņżæļŗ©ņŚåņØ┤ ņé¼ņÜ®ĒĢ£ļŗż. ņģŗņ¦Ė, ņłśņłĀ ņĀä ĒÖśņ×É Ļ░£Ļ░£ņØĖņØś ĒśłņĀä ļ░Å ņČ£Ēśł ņ£äĒŚśņØä ļŗżĻ░üņĀüņ£╝ļĪ£ Ļ│ĀļĀżĒĢśņŚ¼ ļ¦×ņČżĒśĢ ņ╣śļŻī ņĀäļץņØä ņĀüņÜ®ĒĢ£ļŗż. ņØ┤ļ¤¼ĒĢ£ ĒĢŁĒśłņĀäņĀ£ ņé¼ņÜ® ņøÉņ╣ÖņØĆ ļ¼┤ņ×æņ£äņŗ£ĒŚśņØä ĒåĄĒĢ┤ ņ”Øļ¬ģĒĢśĻĖ░ņŚÉļŖö ņĀ£ņĢĮņØ┤ ļ¦ÄņĢä Ļ┤Ćņ░░ ņŚ░ĻĄ¼ļéś ņĀäļ¼ĖĻ░ĆņØś ņØśĻ▓¼ņØä ĻĘ╝Ļ▒░ļĪ£ ņłśļ”ĮļÉśņŚłņ£╝ļ®░ ņĀäĻ│Ą ņśüņŚŁļ│äļĪ£ ņāüņØ┤ĒĢ£ ņ×ģņןņØä ļ│┤ņØ┤Ļ│Ā ņ׳ņ¢┤ Ēæ£ņżĆņ╣śļŻīņ¦Ćņ╣© ņłśĒ¢ēļźĀļÅä ļåÆņ¦Ć ņĢŖļŗż[9-14].
ĒĢŁĒśłņĀäņĀ£ ņé¼ņÜ®ņ×ÉņØś ņłśņłĀ ņĀäĒøä ĒśłņĀä ņ£äĒŚś ĒÅēĻ░Ć Ļ│╝ņĀĢņØĆ ļŗżņØīĻ│╝ Ļ░Öļŗż. ņ▓½ņ¦Ė, ĒÖśņ×É Ļ░£Ļ░£ņØĖņØś ņ×äņāüņĀü ĒŖ╣ņä▒ ļśÉļŖö Ļ┤ĆļÅÖļ¦źļ│æļ│ĆņØś ĒŖ╣ņä▒ņØ┤ Ļ│Āņ£äĒŚśĻĄ░ņØś ņä▒ņāüņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ļŖöņ¦Ć ĒīīņĢģĒĢ£ļŗż (Table 1) [10,13]. ļæśņ¦Ė, ņŗ£ņłĀ ļ░®ļ▓ĢĻ│╝ ņé¼ņÜ®ļÉ£ ņŖżĒģÉĒŖĖņØś ņóģļźś ļ░Å Ļ┤ĆļÅÖļ¦źņżæņ×¼ņłĀņŚÉņä£ ņłśņłĀĻ╣īņ¦ĆņØś Ļ▓ĮĻ│╝ ņŗ£Ļ░äņØä ņóģĒĢ®ĒĢśņŚ¼ ņłśņłĀ ņŗ£ ĒśłņĀäņ£äĒŚśļÅäļź╝ ĒÅēĻ░ĆĒĢ£ļŗż(Table 2) [10,13]. ņģŗņ¦Ė, ņłśņłĀ ņóģļ│äļĪ£ Ļ▓░ņĀĢļÉ£ ņČ£Ēśł ņ£äĒŚśĻ│╝ ņĢ×ņä£ ĻĖ░ņłĀĒĢ£ ĒśłņĀä ņ£äĒŚśņØä ņóģĒĢ®ĒĢśņŚ¼ ņłśņłĀ ņŗ£Ē¢ē ņŗ£ĻĖ░ņÖĆ ĒĢŁĒśłņĀäņĀ£ņØś ņżæļŗ© ļ░Å ņ×¼Ļ░£ ņŗ£ĻĖ░ļź╝ Ļ▓░ņĀĢĒĢ£ļŗż (Table 3; Supplementary Table 1) [10,13]. ņāüĻĖ░ Ļ│╝ņĀĢņØĆ ĒÖśņ×ÉņØś ņ£äĒŚśļÅäļź╝ ņóĆ ļŹö ņäĖļ░ĆĒĢśĻ▓ī ņĀ£Ļ│ĄĒĢĀ ņłś ņ׳ļŗżļŖö ņןņĀÉņØ┤ ņ׳ņ£╝ļéś ņŗżņĀ£ ņ×äņāüņŚÉņä£ ņé¼ņÜ®ĒĢśĻĖ░ņŚÉļŖö ļ▓łĻ▒░ļĪ£ņÜ┤ ņĀÉņØ┤ ļ¦ÄĻ│Ā ņĢäņŖżĒö╝ļ”░ ņé¼ņÜ®ņØä ļ¬©ļōĀ ņłśņłĀņŚÉņä£ Ļ░ĢņĀ£ĒĢśĻ│Ā ņ׳ņ¢┤ ņÖĖĻ│╝ņØśļōżņØś ņĀĆĒĢŁļÅä ņāüļŗ╣ĒĢśļŗż.
ĒśłņĀä ņ£äĒŚśņØś ņśłņĖĪ
ņłśņłĀĻ│╝ ņŚ░Ļ┤ĆļÉ£ ĒśłņĀä ņ£äĒŚśņØĆ ņłśņłĀ Ēøä 30ņØ╝ ņØ┤ļé┤ņŚÉ ļ░£ņāØĒĢśļŖö MACEņØś ļ░£ņāØļźĀņØä ĻĖ░ņżĆņ£╝ļĪ£ ņĀĆņ£äĒŚśĻĄ░(< 1%), ņżæļō▒ļÅäņ£äĒŚśĻĄ░(1-5%), ļ░Å Ļ│Āņ£äĒŚśĻĄ░(Ōēź 5%)ņ£╝ļĪ£ ļČäļźśļÉ£ļŗż[14]. ņłśņłĀ Ēøä ļ░£ņāØĒĢśļŖö MACEļŖö ĒÖśņ×ÉņØś ņ×äņāüņĀü ĒŖ╣ņä▒, Ļ┤ĆļÅÖļ¦źļ│æļ│ĆņØś ĒŖ╣ņä▒, ņŗ£ņłĀņØś ļ│Ąņ×ĪļÅä, ņØæĻ│ĀĻ│äņØś ĒÖ£ņä▒ļÅä ļ░Å ņé¼ņÜ® ņżæņØĖ ĒĢŁĒśłņĀäņĀ£ņØś ņóģļźś ļō▒ ļŗżņ¢æĒĢ£ ņøÉņØĖņØś ņśüĒ¢źņØä ļ░øĻ▓ī ļÉśļ»ĆļĪ£ Ēæ£ņżĆĒÖöļÉ£ ņ£äĒŚśļÅäļź╝ ņĀ£Ļ│ĄĒĢśĻĖ░Ļ░Ć ļ¦żņÜ░ Ēלļōżļŗż[19]. ņāüĻĖ░ ņøÉņØĖļōż ņżæ Ļ┤ĆļÅÖļ¦źņżæņ×¼ņłĀļČĆĒä░ ņłśņłĀĻ╣īņ¦Ć Ļ▓ĮĻ│╝ ņŗ£Ļ░ä ļ░Å ņłśņłĀ ņĀä DAPTņØś ņĪ░ĻĖ░ ņżæļŗ© ņŚ¼ļČĆĻ░Ć ĒśłņĀä ņé¼Ļ▒┤ ļ░£ņāØņŚÉ Ļ░Ćņן ņżæņÜöĒĢ£ ņÜöņØĖņØ┤ļŗż. ļö░ļØ╝ņä£, ņłśņłĀ ņŗ£ĻĖ░ņÖĆ ņłśņłĀ ņĀä DAPTņØś ņżæļŗ© ņŚ¼ļČĆļŖö ņŖżĒģÉĒŖĖ ņé¼ņÜ® ņŚ¼ļČĆ, ņŖżĒģÉĒŖĖņØś ņóģļźś, ņ×äņāüņĀü ļ░Å Ļ┤ĆļÅÖļ¦źļ│æļ│ĆņØś ĒŖ╣ņ¦Ģ ļō▒ņØä ņóģĒĢ®ņĀüņ£╝ļĪ£ Ļ│ĀļĀżĒĢ£ Ēøä Ļ▓░ņĀĢĒĢ┤ņĢ╝ ĒĢ£ļŗż.
ņ×äņāü ņ¢æņāü ļ░Å Ļ┤ĆļÅÖļ¦źļ│æļ│ĆņØś ĒŖ╣ņä▒
ļéśņØ┤, ļŗ╣ļć©ļ│æ, ņŗĀļČĆņĀä, ņŗ¼ļČĆņĀä ļ░Å ņóīņŗ¼ņŗżĻĄ¼ĒśłļźĀ ļō▒ ļ¦żņÜ░ ļŗżņ¢æĒĢ£ ņ£äĒŚśņØĖņ×ÉĻ░Ć ņłśņłĀ Ēøä ĒśłņĀä ņé¼Ļ▒┤ņØś ļ░£ņāØņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣śļ®░ ĻĖēņä▒Ļ┤ĆļÅÖļ¦źņ”ØĒøäĻĄ░ņØś ļ│æļĀź, ņŖżĒģÉĒŖĖĒśłņĀäņ”ØņØś ļ│æļĀź, ņŗ¼ĻĘ╝Ļ▓Įņāēņ”ØņØś ņ×¼ļ░£ ļ│æļĀź ļō▒ļÅä ņżæņÜöĒĢ£ ņ£äĒŚśņØĖņ×ÉļōżņØ┤ļŗż(Table 1) [10,13]. ņāüĻĖ░ņØś ņ×äņāü ņ¢æņāüļōżĻ│╝ ĒĢ©Ļ╗ś Ļ┤ĆļÅÖļ¦źļ│æļ│ĆņØś ĒŖ╣ņä▒Ļ│╝ ņŗ£ņłĀņØś ļ│Ąņ×ĪļÅä ļśÉĒĢ£ ņČ®ļČäĒ׳ Ļ│ĀļĀż Ēøä ĒĢŁĒśłņĀäņĀ£ņØś ņżæļŗ© ņŚ¼ļČĆļź╝ ĒīÉļŗ©ĒĢ┤ņĢ╝ ĒĢ£ļŗż(Table 1). ļ│æļ│ĆņØś ņ╣śļŻīļź╝ ņ£äĒĢ┤ 3Ļ░£ ņØ┤ņāüņØś ņŖżĒģÉĒŖĖĻ░Ć ņéĮņ×ģļÉśņŚłĻ▒░ļéś 3ĻĄ░ļŹ░ ņØ┤ņāüņØś ļ│æļ│ĆņØä ņ╣śļŻīĒĢ£ Ļ▓ĮņÜ░ ļ░Å ļČäņ¦Ćļ│æļ│ĆņŚÉ ļīĆĒĢ£ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢ£ Ļ▓ĮņÜ░ ļō▒ņØĆ ĒśłņĀä ņ£äĒŚśņØ┤ ņāüņŖ╣ĒĢśļ»ĆļĪ£ ļ╣äņŗ¼ņןņłśņłĀņØä ņŗ£Ē¢ēĒĢĀ Ļ▓ĮņÜ░ ņŻ╝ņØśļź╝ ņÜöĒĢ£ļŗż[10,13]. ļśÉĒĢ£ ĒśłņĀä ņ£äĒŚśņØ┤ ļåÆņ¦Ć ņĢŖļŹöļØ╝ļÅä ņóīņŻ╝Ļ░äļČĆ Ļ┤ĆļÅÖļ¦źĻ│╝ Ļ░ÖņØ┤ ĒśłņĀä ņé¼Ļ▒┤ņØ┤ ļ░£ņāØĒĢśļ®┤ ņ╣śļ¬ģņĀüņØĖ Ļ▓░Ļ│╝ļź╝ ņ┤łļלĒĢĀ ņłś ņ׳ļŖö ļ│æļ│ĆņŚÉ ņŗ£ņłĀņØä ĒĢ£ Ļ▓ĮņÜ░ņŚÉļŖö ĒĢŁĒśłņĀäņĀ£ņØś ņżæļŗ©ņØä Ēö╝ĒĢ┤ņĢ╝ ĒĢ£ļŗż.
ņłśņłĀ ņŗ£ĻĖ░ņŚÉ ļö░ļźĖ ņ£äĒŚśļÅäņÖĆ DAPTņØś ņĪ░ĻĖ░ņżæļŗ©
Ļ┤ĆļÅÖļ¦źņżæņ×¼ņłĀ ĒøäļČĆĒä░ ņłśņłĀĻ╣īņ¦Ć Ļ▓ĮĻ│╝ ņŗ£Ļ░äņØĆ DAPT ņżæļŗ©ņŚÉ ļö░ļźĖ ĒśłņĀä ņé¼Ļ▒┤ ļ░£ņāØņØś Ļ░Ćņן ņżæņÜöĒĢ£ ņøÉņØĖ ņżæ ĒĢśļéśņØ┤ļŗż. ņŚ¼ļ¤¼ ņŚ░ĻĄ¼ļōżņŚÉņä£ ņłśņłĀ ņĀäĒøä ĒśłņĀä ņé¼Ļ▒┤ ļ░£ņāØļźĀņØĆ Ļ┤ĆļÅÖļ¦źņżæņ×¼ņłĀ ĒøäļČĆĒä░ ņłśņłĀņØ┤ ņŗ£Ē¢ēļÉśĻĖ░Ļ╣īņ¦ĆņØś ņŗ£Ļ░äĻ│╝ ļ░ĆņĀæĒĢ£ Ļ┤ĆĻ│äĻ░Ć ņ׳ļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż. ĒĢśņ¦Ćļ¦ī, ĻĘĖ ĻĘ╝Ļ▒░Ļ░Ć ļÉśļŖö ļ¦ÄņØĆ ņŚ░ĻĄ¼ļōżņØ┤ ņłśņłĀ ņĀäĒøä ĒĢŁĒśłņåīĒīÉņĀ£ ņé¼ņÜ®ņŚÉ ļīĆĒĢ£ ĻĖ░ņłĀņØä ļ¬ģĒÖĢĒĢśĻ▓ī ĒĢśņ¦Ć ņĢŖņĢä ĒĢŁĒśłņåīĒīÉņĀ£ņØś ņ¦ĆņåŹ ļśÉļŖö ņżæļŗ©Ļ│╝ ĒśłņĀä ņé¼Ļ▒┤ ļ░£ņāØ ņé¼ņØ┤ņØś ņØĖĻ│╝Ļ┤ĆĻ│äļź╝ ĻĘ£ņĀĢĒĢśĻĖ░ ņ¢┤ļĀżņÜ┤ Ļ▓ĮņÜ░Ļ░Ć ļ¦Äļŗż[20-23].
ņłśņłĀņŚÉ ļö░ļźĖ ĒśłņĀä ņé¼Ļ▒┤ņØś ņ£äĒŚśļÅäļŖö ņ▓½ 1ļģä ļÅÖņĢł ņāüņŖ╣ĒĢśņ¦Ćļ¦ī ĻĘĖ ņØ┤ĒøäņŚÉļŖö ņŖżĒģÉĒŖĖļź╝ ņéĮņ×ģĒĢśņ¦Ć ņĢŖņØĆ ĒÖśņ×ÉņÖĆ ļÅÖņØ╝ĒĢ£ Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ņ¢┤ ĒśäĒ¢ē Ēæ£ņżĆņ╣śļŻīņ¦Ćņ╣©ņØĆ Ļ┤ĆļÅÖļ¦źņżæņ×¼ņłĀ Ēøä 1ļģä ļé┤ņŚÉ ļ╣äņŗ¼ņןņä▒ņłśņłĀņØ┤ ĒĢäņÜöĒĢ£ Ļ▓ĮņÜ░ņØś ņ£äĒŚśļÅä ņśłņĖĪņŚÉ ņŻ╝ņĢłņĀÉņØä ļæÉĻ│Ā ņ׳ļŗż[12,14]. ļŹ┤ļ¦łĒü¼ņŚÉņä£ ņŗ£Ē¢ēļÉ£ Ļ┤Ćņ░░ ņŚ░ĻĄ¼ņŚÉņä£ ņĢĮļ¼╝ ļ░®ņČ£ņŖżĒģÉĒŖĖ(drug eluting stent, DES)ļź╝ ņéĮņ×ģ Ēøä 1Ļ░£ņøöņØ┤ ņ¦Ćļéśļ®┤ Ļ┤ĆļÅÖļ¦źņ¦łĒÖśņØ┤ ņŚåļŖö ĒÖśņ×ÉņÖĆ ņ£Āņé¼ĒĢ£ ņłśņłĀ ņĀäĒøä ņŗ¼ĻĘ╝Ļ▓Įņāēņ”Ø ļ░£ņāØļźĀĻ│╝ ņé¼ļ¦ØļźĀņØä ļ│┤ņØ┤ļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļéś ņŗ£ņłĀ Ēøä 1-3Ļ░£ņøöņØ┤ ņ¦Ćļéśļ®┤ Ļ│Āņ£äĒŚśĻĄ░ņØś ņ×äņāü ņ¢æņāüņØ┤ ņŚåĻ│Ā ļ│Ąņ×ĪĒĢ£ Ļ┤ĆļÅÖļ¦źņżæņ×¼ņłĀņØä ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖņØĆ Ļ▓ĮņÜ░ ļ╣äĻĄÉņĀü ņĢłņĀäĒĢśĻ▓ī ņłśņłĀņØä ņŗ£Ē¢ēĒĢĀ ņłś ņ׳ļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż[6]. ļŗżļźĖ ļ¦ÄņØĆ Ļ┤Ćņ░░ ņŚ░ĻĄ¼ļōżņŚÉņä£ļÅä ņłśņłĀĻ│╝ ņŚ░Ļ┤ĆļÉ£ ĒśłņĀä ņé¼Ļ▒┤ņØś ņ”ØĻ░ĆļŖö 3-6Ļ░£ņøö ĒøäļČĆĒä░ ņĢłņĀĢĒÖöļÉ£ļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśĻ│Ā ņ׳ļŗż[21,24]. ļö░ļØ╝ņä£ Ļ┤ĆļÅÖļ¦źņżæņ×¼ņłĀ Ēøä ļ╣äņØæĻĖēņłśņłĀņØĆ Ļ░ĆļŖźĒĢ£ 6Ļ░£ņøö ņØ┤ĒøäļĪ£ ņŚ░ĻĖ░ĒĢśļŖö Ļ▓āņØ┤ ņóŗļŗż. ĒĢśņ¦Ćļ¦ī, ņāüĻĖ░ ņŚ░ĻĄ¼ ļōżņŚÉņä£ļŖö ĒĢŁĒśłņåīĒīÉņĀ£ ņé¼ņÜ® ņŚ¼ļČĆņŚÉ ļö░ļźĖ ĒśłņĀä ļ░Å ņČ£Ēśł ņ£äĒŚśņŚÉ ļīĆĒĢ£ ļČäņäØ Ļ▓░Ļ│╝Ļ░Ć ņĀ£ņŗ£ļÉśņ¢┤ ņ׳ņ¦Ć ņĢŖņĢä ņĀ£ĒĢ£ņĀÉņØ┤ ņ׳ļŗż. ļ╣äņØæĻĖēņłśņłĀņØä ņ¢ĖņĀ£Ļ╣īņ¦Ć ņŚ░ĻĖ░ĒĢĀ Ļ▓āņØĖĻ░ĆņŚÉ ļīĆĒĢ£ ĻĖ░ņżĆņØĆ ņ£Āļ¤ĮĻ│╝ ļ»ĖĻĄŁņØś Ēæ£ņżĆņ╣śļŻīņ¦Ćņ╣©ņŚÉļÅä ņ░©ņØ┤Ļ░Ć ņ׳ļŗż[12,14]. ņ£Āļ¤Įņŗ¼ņןĒĢÖĒÜīņØś Ēæ£ņżĆņ╣śļŻīņ¦Ćņ╣©ņØĆ ņĢäņŖżĒö╝ļ”░ņØä ņ£Āņ¦ĆĒĢĀ ņłś ņ׳ļŗżļ®┤ ņé¼ņÜ®ļÉ£ ņŖżĒģÉĒŖĖņŚÉ ņāüĻ┤ĆņŚåņØ┤ ņŗ£ņłĀ Ēøä 1Ļ░£ņøöņØ┤ ņ¦Ćļéśļ®┤ P2Y12 ņłśņÜ®ņ▓┤ ņ¢ĄņĀ£ņĀ£ļŖö ņżæļŗ©ĒĢĀ ņłś ņ׳Ļ│Ā ļ╣äņØæĻĖēņłśņłĀļÅä Ļ░ĆļŖźĒĢ£ Ļ▓āņ£╝ļĪ£ ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż[14]. ĒĢśņ¦Ćļ¦ī, ĻĖēņä▒Ļ┤ĆļÅÖļ¦źņ”ØĒøäĻĄ░ņØ┤ļéś ļ│Ąņ×ĪĒĢ£ ņŗ£ņłĀņØä ņŗ£Ē¢ēĒĢ£ Ļ▓ĮņÜ░ 6Ļ░£ņøö ļÅÖņĢł DAPTļź╝ ņ£Āņ¦ĆĒĢśĻ│Ā ņłśņłĀ ļśÉĒĢ£ ņØ┤ ĻĖ░Ļ░ä ļÅÖņĢłņØĆ ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖļÅäļĪØ ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż[14]. ļ»ĖĻĄŁņŗ¼ņןĒĢÖĒÜīņØś Ēæ£ņżĆņ╣śļŻīņ¦Ćņ╣©ņØĆ ņØ╝ļ░śĻĖłņåŹņŖżĒģÉĒŖĖ(bare metal stent, BMS)ļź╝ ņéĮņ×ģĒĢ£ Ļ▓ĮņÜ░ 30ņØ╝ņØ┤ Ļ▓ĮĻ│╝ĒĢśļ®┤ ļ╣äņØæĻĖēņłśņłĀņØä ņŗ£Ē¢ēĒĢĀ ņłś ņ׳Ļ│Ā DESļź╝ ņéĮņ×ģĒĢ£ Ļ▓ĮņÜ░ 3Ļ░£ņøöĻ░äņØĆ ņØæĻĖē ņāüĒÖ®ņØä ņĀ£ņÖĖĒĢ£ ņłśņłĀņØĆ ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖļÅäļĪØ ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż[12]. ļ¦īņĢĮ, DAPT ņżæļŗ©Ļ│╝ ņŚ░Ļ┤ĆļÉ£ ĒśłņĀä ņ£äĒŚśļ│┤ļŗż ņłśņłĀņØä ņŚ░ĻĖ░ĒĢśņśĆņØä ļĢī ņśłņāüļÉśļŖö ņ¦łĒÖśņØś ņ¦äĒ¢ē ļśÉļŖö ĒĢ®ļ│æņ”Ø ļ░£ņāØņØś ņ£äĒŚśļÅäĻ░Ć ļŹö ļåÆļŗżļ®┤ DESļź╝ ņéĮņ×ģĒĢśņśĆļŹöļØ╝ļÅä 3-6Ļ░£ņøöņŚÉ ņŗ£Ē¢ēņØä Ļ│ĀļĀżĒĢĀ ņłś ņ׳ļŗż[12].
ņŖżĒģÉĒŖĖ ņóģļźśņŚÉ ļö░ļźĖ ņ£äĒŚśļÅä
ņŖżĒģÉĒŖĖ ņĀ£ņ×æ ĻĖ░ņłĀņØś ļ░£ņĀäĻ│╝ ļŹöļČłņ¢┤ ņŖżĒģÉĒŖĖņÖĆ ņŚ░Ļ┤ĆļÉ£ ĒśłņĀä ņ£äĒŚśņØ┤ ĒÜŹĻĖ░ņĀüņ£╝ļĪ£ Ļ░ÉņåīĒĢśņśĆņ£╝ļ®░, ņØ┤ļŖö DAPT ņé¼ņÜ® ĻĖ░Ļ░ä ļŗ©ņČĢņØś ņżæņÜöĒĢ£ ĻĘ╝Ļ▒░Ļ░Ć ļÉśĻ│Ā ņ׳ļŗż[24-27]. ĒĢśņ¦Ćļ¦ī, ņŗ£ņłĀ ĒśłĻ┤ĆņØś ĻĖ░ļŖź ĒÜīļ│ĄĻ│╝ ņŖżĒģÉĒŖĖĻ░Ć ņéĮņ×ģļÉ£ ĒśłĻ┤ĆņØś ņ×¼ņāüĒö╝ĒÖöĻ░Ć ņ¦äĒ¢ēļÉśļŖö ņłśĻ░£ņøö ļÅÖņĢł ņŖżĒģÉĒŖĖņÖĆ ņŚ░Ļ┤ĆļÉ£ ĒśłņĀä ņ£äĒŚśņØä ņśłļ░®ĒĢśĻĖ░ ņ£äĒĢ┤ DAPTļź╝ ņØ╝ņĀĢ ĻĖ░Ļ░ä ļ░śļō£ņŗ£ ņé¼ņÜ®ĒĢ┤ņĢ╝ ĒĢ£ļŗż[12,14]. ĒÆŹņäĀņä▒ĒśĢņłĀļ¦īņ£╝ļĪ£ ņ╣śļŻīĒĢ£ ĒÖśņ×ÉņŚÉņä£ļŖö ĒśłņĀä ņ£äĒŚśņØä ļåÆņØ╝ ņłś ņ׳ļŖö ņ×äņāü ņ¢æņāüņØ┤ļéś Ļ┤ĆļÅÖļ¦źļ│æļ│ĆņØś ĒŖ╣ņä▒ņØ┤ ņŚåļŖö Ļ▓ĮņÜ░ ņŗ£ņłĀ Ēøä 2ņŻ╝Ļ░Ć Ļ▓ĮĻ│╝ĒĢśļ®┤ DAPTņØś ņżæļŗ©ņØä Ļ│ĀļĀżĒĢ┤ ļ│╝ ņłś ņ׳ņ¦Ćļ¦ī, ĒÆŹņäĀņä▒ĒśĢņłĀļ¦īņ£╝ļĪ£ ņ╣śļŻīĒĢśļŹöļØ╝ļÅä ņ×äņāüņĀü ņ£äĒŚśņØĖņ×ÉĻ░Ć ņ׳ļŖö Ļ▓ĮņÜ░ ņĄ£ņåī 1Ļ░£ņøö ļÅÖņĢłņØĆ DAPTļź╝ ņ£Āņ¦ĆĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż(Table 2) [12].
ņŖżĒģÉĒŖĖņØś ņóģļźśņÖĆ ļ╣äņŗ¼ņןņłśņłĀ Ēøä ĒśłņĀä ņé¼Ļ▒┤ ļ░£ņāØ ņé¼ņØ┤ņØś ņŚ░Ļ┤Ćņä▒ņØĆ ļ¬ģĒÖĢĒĢśņ¦Ć ņĢŖļŗż. 1ņäĖļīĆ DESņÖĆ BMS ņé¼ņÜ®ņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ņŗ£Ē¢ēļÉ£ Ontario stent registryņŚÉņä£ļŖö BMSļź╝ ņé¼ņÜ®ĒĢ£ Ļ▓ĮņÜ░ņŚÉļŖö 46-180ņØ╝ ņé¼ņØ┤ņŚÉ, 1ņäĖļīĆ DESļź╝ ņé¼ņÜ®ĒĢ£ Ļ▓ĮņÜ░ļŖö 180ņØ╝ ņØ┤ĒøäņŚÉ ļ╣äņØæĻĖēņłśņłĀņØä ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØ┤ ņĀüĒĢ®ĒĢśļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż[28]. ĒĢśņ¦Ćļ¦ī, ļśÉ ļŗżļźĖ Ļ┤Ćņ░░ ņŚ░ĻĄ¼ļōżņŚÉņä£ļŖö ņŗ£ņłĀ Ēøä 6Ļ░£ņøö ņØ┤ĒøäņŚÉ ņłśņłĀņØä ņŗ£Ē¢ēĒĢĀ Ļ▓ĮņÜ░ ņé¼ņÜ®ļÉ£ ņŖżĒģÉĒŖĖņØś ņóģļźśļŖö ĒśłņĀä ņé¼Ļ▒┤ņØś ļ░£ņāØĻ│╝ ļ¼┤Ļ┤ĆĒĢ£ Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀĒĢśņśĆļŗż[15,29]. Ēśäņ×¼ ņé¼ņÜ®ļÉśĻ│Ā ņ׳ļŖö DESļŖö 1ņäĖļīĆ DESļ│┤ļŗż ņÜ░ņłśĒĢ£ ņĢłņĀĢņä▒ņØä ĒÖĢļ│┤ĒĢśĻ│Ā ņ׳ņ¢┤ ņéĮņ×ģ ļÉ£ ņŖżĒģÉĒŖĖņØś ņóģļźśļ│┤ļŗżļŖö ņŗ£ņłĀņØś ļ│Ąņ×Īņä▒(ņ╣śļŻīĒĢ£ ĒśłĻ┤Ć ņłś, ņé¼ņÜ®ļÉ£ ņŖżĒģÉĒŖĖņØś ņ┤Ø ņłśņÖĆ ņ┤Ø ĻĖĖņØ┤, ļ│æļ│ĆņØś ĒŖ╣ņä▒)ņŚÉ ļö░ļØ╝ DAPT ņé¼ņÜ® ĻĖ░Ļ░ä ļ░Å ļ╣äņŗ¼ņןņłśņłĀņØś ņŗ£ĻĖ░ļź╝ Ļ▓░ņĀĢĒĢśļŖö Ļ▓āņØ┤ ļŹö ņĀüņĀłĒĢĀ Ļ▓āņ£╝ļĪ£ ĒīÉļŗ©ļÉśļéś Ē¢źĒøä ļ¼┤ņ×æņ£ä ņŚ░ĻĄ¼ļź╝ ĒåĄĒĢ£ ņ”Øļ¬ģņØ┤ ĒĢäņÜöĒĢśļŗż[30].
ņČ£Ēśł ņé¼Ļ▒┤ņØś ņśłņĖĪ
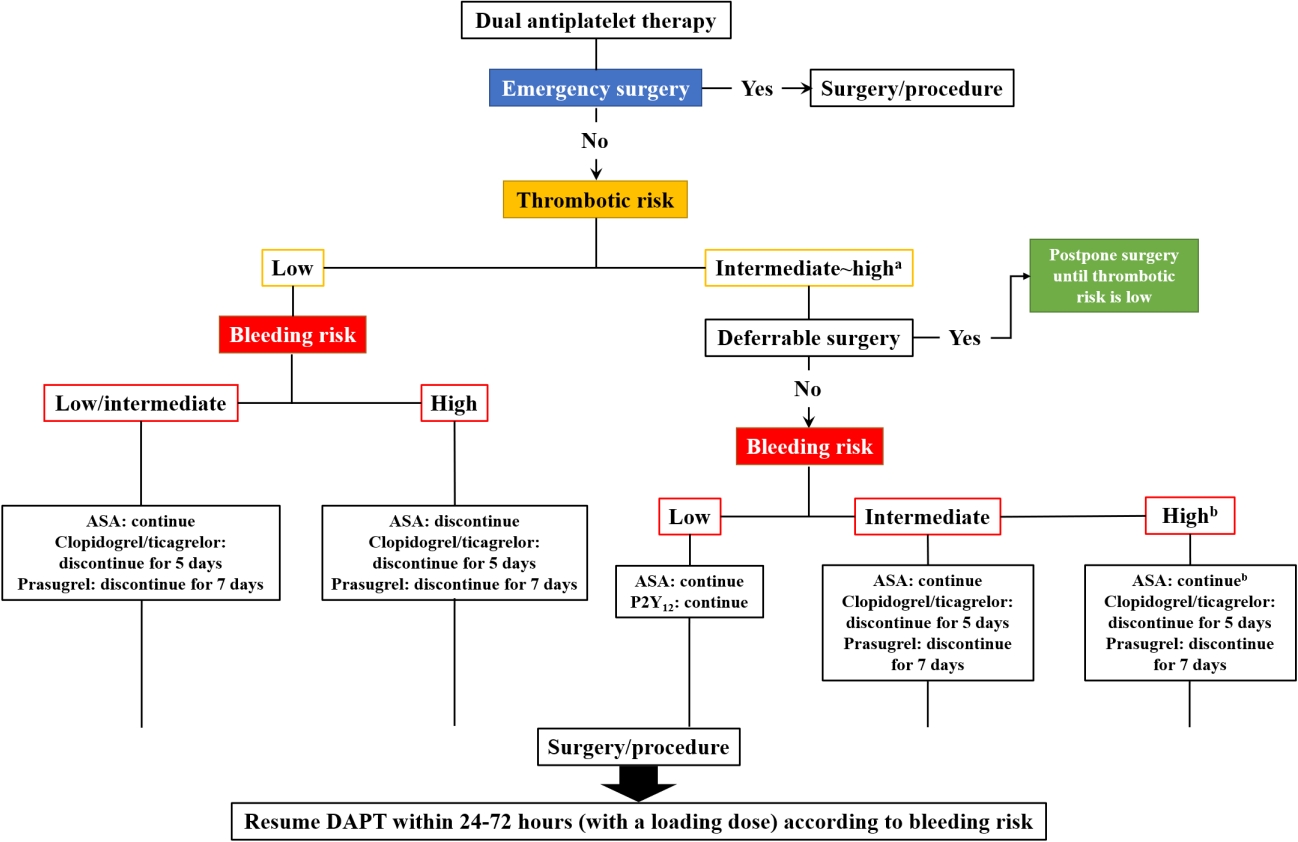
ņŗ¼ĒśłĻ┤Ćņ¦łĒÖśņ×ÉņØś ļ╣äņŗ¼ņןņłśņłĀ ņżĆļ╣ä ņżæ ĒĢŁĒśłņĀäņĀ£ņØś ņ¦ĆņåŹ ļśÉļŖö ņżæļŗ©ņØä Ļ▓░ņĀĢĒĢ┤ņĢ╝ ĒĢĀ ļĢī ĒśłņĀä ļ░Å ņČ£Ēśł ņ£äĒŚśņØä ĒĢ©Ļ╗ś Ļ│ĀļĀżĒĢśņŚ¼ ņ╣śļŻī ņĀäļץņØä ņłśļ”ĮĒĢśļŖö Ļ▓āņØ┤ ņżæņÜöĒĢśļŗż. ļ╣äņŗ¼ņןņłśņłĀņØĆ ņČ£Ēśł ņ£äĒŚśņŚÉ ļö░ļØ╝ ņĀĆņ£äĒŚśĻĄ░, ņżæļō▒ļÅäņ£äĒŚśĻĄ░ ļ░Å Ļ│Āņ£äĒŚśĻĄ░ņ£╝ļĪ£ ļČäļźśļÉśĻ│Ā ņØ┤ļ¤¼ĒĢ£ ņ£äĒŚśļÅäļŖö ņłśņłĀ Ēøä ļ░£ņāØ Ļ░ĆļŖźĒĢ£ ņČ£ĒśłņØś ņ£äĒŚśļÅäļ│┤ļŗżļŖö ņłśņłĀ Ēøä ņĀüņĀłĒĢ£ ņ¦ĆĒśłņØ┤ Ļ░ĆļŖźĒĢ£ņ¦ĆņŚÉ ļö░ļØ╝ Ļ▓░ņĀĢļÉ£ļŗż[10,12-14].
ļ»ĖĻĄŁĻ│╝ ņ£Āļ¤ĮņØś Ēæ£ņżĆņ╣śļŻīņ¦Ćņ╣©ņØĆ ņĢĮ 250Ļ░£ņØś ņłśņłĀņŚÉ ļīĆĒĢ┤ ņČ£ĒśłņØś ņ£äĒŚśļÅäļź╝ ĻĘ£ņĀĢĒĢ┤ ļåōĻ│Ā ņ׳ņ£╝ļ®░ ņØ┤ļŖö ĒÖśņ×ÉņØś ņČ£Ēśł ņä▒Ē¢źņØ┤ļéś ļé┤ņ×¼ņĀü ņ£äĒŚśļÅäļ│┤ļŗżļŖö ņłśņłĀ ņ×Éņ▓┤ņÖĆ ņŚ░Ļ┤ĆļÉ£ ņČ£Ēśł ņ£äĒŚśļÅäļź╝ ĻĖ░ļ░śņ£╝ļĪ£ ņ×æņä▒ļÉśņŚłļŗż(Supplementary Table 1) [10,12-14]. ņØ┤ļ¤¼ĒĢ£ ļČäļźśļŖö ļ¼┤ņ×æņ£ä ņŚ░ĻĄ¼Ļ░Ć ņĢäļŗī Ļ┤Ćņ░░ ņŚ░ĻĄ¼ļéś ņĀäļ¼ĖĻ░ĆņØś ņØśĻ▓¼ņØä ļ░öĒāĢņ£╝ļĪ£ ņĀ£ņĀĢļÉśņ¢┤ ņ׳ļŗżļŖö ļŗ©ņĀÉņØ┤ ņ׳Ļ│Ā ņłśņłĀ Ēøä ņä▒Ļ│ĄņĀüņØĖ ņ¦ĆĒśł ņŚ¼ļČĆļŖö ņ¦æļÅäņØśņØś ņłÖļĀ©ļÅäņÖĆ ņ¦üņĀæņĀüņØĖ ņŚ░Ļ┤Ćņä▒ņØ┤ ņ׳ņ£╝ļ»ĆļĪ£ ņ¦æļÅäņØśļéś ņØśļŻīĻĖ░Ļ┤Ć Ļ░äņØś ņ¦äļŻīņØś ĒÄĖņ░©Ļ░Ć ļ░£ņāØĒĢśļŖö ņŻ╝ņÜöĒĢ£ ņøÉņØĖņØ┤ ļÉ£ļŗż[10,12-14].
Ēśäņ×¼ ļ»ĖĻĄŁ ļ░Å ņ£Āļ¤ĮņØś Ēæ£ņżĆņ¦äļŻīņ¦Ćņ╣©ņØĆ ņøÉņ╣ÖņĀüņ£╝ļĪ£ ņČ£ĒśłņØś ņ£äĒŚśļÅäĻ░Ć ļé«ņØĆ(ņĀĆņ£äĒŚśļÅä) ņłśņłĀņØä ņŗ£Ē¢ēĒĢĀ Ļ▓ĮņÜ░ ņłśņłĀ ņĀäĒøäņŚÉ DAPTļź╝ Ļ░ĆļŖźĒĢ£ ņ£Āņ¦ĆĒĢśļÅäļĪØ ĻČīņ£ĀĒĢśĻ│Ā ņ׳ņ£╝ļ®░ ņżæļō▒ļÅä ņ£äĒŚśļÅäņØś ņłśņłĀņØä ņŗ£Ē¢ēĒĢĀ Ļ▓ĮņÜ░ņŚÉļŖö ņĢäņŖżĒö╝ļ”░ņØĆ ļ░śļō£ņŗ£ ņ£Āņ¦ĆĒĢśĻ│Ā P2Y12 ņłśņÜ®ņ▓┤ ņ¢ĄņĀ£ņĀ£ļŖö Ļ░ĆļŖźĒĢ£ ņżæļŗ©ĒĢśļÅäļĪØ ĻČīņ£ĀĒĢśĻ│Ā ņ׳ļŗż[10,12-14]. ļśÉĒĢ£, ĒśłĻ┤Ćņ×¼Ļ▒┤ņłĀ, ļ│Ąņ×ĪĒĢ£ ļé┤ņן ņłśņłĀ, ņŗĀĻ▓ĮņÖĖĻ│╝ņĀü ņłśņłĀ ļ░Å Ļ▓ĮĻĖ░Ļ┤Ćņ¦Ć ņłśņłĀĻ│╝ Ļ░ÖņØĆ Ļ│ĀņČ£Ēśł ņ£äĒŚśļÅä ņłśņłĀņØä ņŗ£Ē¢ēĒĢĀ Ļ▓ĮņÜ░ņŚÉļÅä ņĀüņĀłĒĢ£ ņŗ£ĻĖ░ņŚÉ P2Y12 ņłśņÜ®ņ▓┤ ņ¢ĄņĀ£ņĀ£ļź╝ ņżæļŗ©ĒĢśļÅäļĪØ ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż(Table 3; Supplementary Table 1) [12,14]. ĒÖśņ×É Ļ░£Ļ░£ņØĖņØś ņČ£Ēśł ņ£äĒŚśļÅäļź╝ ĒÅēĻ░ĆĒĢśĻĖ░ ņ£äĒĢ┤ ņä▒ļ│ä, ņŗĀĻĖ░ļŖź ļ░Å ļÅÖļ░ś ņ¦łĒÖśņØä ļ░öĒāĢņ£╝ļĪ£ ļ¬ć Ļ░Ćņ¦Ć ņČ£Ēśł ņ£äĒŚśļÅä ĒÅēĻ░ĆļÅäĻĄ¼ļōżņØ┤ Ļ░£ļ░£ļÉśņ¢┤ ņ׳ņ¦Ćļ¦ī ļ╣äņŗ¼ņןņłśņłĀ ĒÖśņ×ÉņŚÉ ĒŖ╣ĒÖöļÉ£ ļÅäĻĄ¼ļōżņØĆ ņĢäļŗłļŗż[31-33].
ņłśņłĀ Ēøä ņ¦ĆĒśłņØ┤ ņČ®ļČäĒ׳ ļÉśņŚłļŗżĻ│Ā ĒīÉļŗ©ļÉśļ®┤ Ļ░ĆļŖźĒĢ£ ļ╣©ļ”¼ ĒĢŁĒśłņĀäņĀ£ļź╝ ņ×¼Ļ░£ĒĢ┤ņĢ╝ ĒĢśņ¦Ćļ¦ī ņ×äņāüņĀüņ£╝ļĪ£ ņØśļ»Ė ņ׳ļŖö ņČ£Ēśł ņé¼Ļ▒┤ņØ┤ ļ░£ņāØĒĢĀ Ļ▓ĮņÜ░ ĒĢŁĒśłņĀäņĀ£ņØś ņ×¼ņé¼ņÜ®ņØĆ ņ¦ĆĒśłņØ┤ ņČ®ļČäĒ׳ ļÉĀ ļĢīĻ╣īņ¦Ć ņŚ░ĻĖ░ĒĢĀ ņłś ņ׳ļŗż. ļśÉĒĢ£, ņČ£Ēśł ņ£äĒŚśņØ┤ ļ¦żņÜ░ ļåÆņØä Ļ▓āņ£╝ļĪ£ ņśłņāüļÉĀ Ļ▓ĮņÜ░ ļ│ĄĻ░ĢĻ▓Į ņłśņłĀ, ļĪ£ļ┤ć ņłśņłĀ ļśÉļŖö ļĀłņØ┤ņĀĆ ņłśņłĀ ļō▒ņØś ņĄ£ņåī ņ╣©ņŖĄ ņłśņłĀņØä ņŗ£Ē¢ēĒĢśļŖö Ļ▓āļÅä Ļ│ĀļĀżĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż[10,13].
ņłśņłĀ ņĀä ĒĢŁĒśłņåīĒīÉņĀ£ ņĪ░ņĀł
ĒĢŁĒśłņåīĒīÉņĀ£ņØś Ļ░ĆĻĄÉņÜöļ▓Ģ(bridging therapy)
ĒĢŁĒśłņåīĒīÉņĀ£ Ļ░ĆĻĄÉņÜöļ▓ĢņØĆ ĒśłņåīĒīÉņĀ£ļź╝ ņżæļŗ©ĒĢĀ Ļ▓ĮņÜ░ ĒśłņĀä ņ£äĒŚśņØ┤ ļ¦żņÜ░ ļåÆņØĆ ĒÖśņ×ÉņŚÉņä£ ņČ£Ēśł ņ£äĒŚśņØ┤ ļåÆņØĆ ņłśņłĀņØä ļ»ĖļŻ░ ņłś ņŚåļŖö Ļ▓ĮņÜ░ņŚÉ ņØ╝ņŗ£ņĀüņ£╝ļĪ£ Ļ▓ĮĻĄ¼ĒśĢ ĒĢŁĒśłņåīĒīÉņĀ£ ļīĆņŗĀ ņ×æņÜ® ņŗ£Ļ░äņØ┤ ņ¦¦ņØĆ ņĀĢļ¦źņŻ╝ņé¼ĒśĢ ĒĢŁĒśłņåīĒīÉņĀ£ļź╝ ĻĄÉņ▓┤ Ēł¼ņŚ¼ĒĢśļŖö Ļ▓āņØä ļ¦ÉĒĢ£ļŗż[10]. ņĢäņ¦ü Ļ░ĆĻĄÉņÜöļ▓ĢņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼Ļ░Ć ļ¦Äņ¦Ć ņĢŖĻĖ░ ļĢīļ¼ĖņŚÉ ņØ┤ņŚÉ ļīĆĒĢ£ ņĀüņØæ ņ”ØņØ┤ ĒÖĢļ”ĮļÉśņ¢┤ ņ׳ņ¦Ć ņĢŖļŗż. ņ£Āļ¤Įņŗ¼ņןĒĢÖĒÜī Ēæ£ņżĆņ╣śļŻīņ¦Ćņ╣©ņŚÉņä£ļŖö ņżæņ×¼ņŗ£ņłĀ ņŗ£Ē¢ē Ēøä 1Ļ░£ņøö ņØ┤ļé┤ņŚÉ ļ¬©ļōĀ ĒĢŁĒśłņåīĒīÉņĀ£ļź╝ ņżæļŗ©ĒĢ┤ņĢ╝ ĒĢĀ Ļ▓ĮņÜ░ Ļ│ĀļĀżĒĢ┤ ļ│╝ ņłś ņ׳ļŗżĻ│Ā ĻĖ░ņłĀĒĢśĻ│Ā ņ׳ļŗż[14].
Ļ░ĆĻĄÉņÜöļ▓ĢņŚÉ ņé¼ņÜ®ĒĢĀ ņłś ņ׳ļŖö ņĀĢļ¦źņŻ╝ņé¼ĒśĢ ĒĢŁĒśłņåīĒīÉņĀ£ļĪ£ļŖö ņ╣ĖĻĘĖļĀÉļ¤¼(cangrelor), Ēŗ░ļĪ£Ēö╝ļ░ś(tirofiban), ņĢ▒Ēŗ░Ēö╝ļ░öĒāĆņØ┤ļō£(eptifibatide) ļō▒ņØ┤ ņ׳ļŗż. ĒŚżĒīīļ”░(heparin)Ļ│╝ Ļ░ÖņØĆ ĒĢŁņØæĻ│ĀņĀ£ļŖö ņśżĒ׳ļĀż ĒśłņåīĒīÉ ņØæņ¦æņØä ņĪ░ņןĒĢśĻ│Ā ĒśłņĀä ņāØņä▒Ļ│╝ ĒśłņĀä ņé¼Ļ▒┤ņØś ņ£äĒŚśņä▒ņØä ņ”ØĻ░Ćņŗ£Ēé¼ ņłś ņ׳ļŗżļŖö ļ│┤Ļ│ĀĻ░Ć ņ׳ļŗż[34]. ņĢäņ¦ü ĻĄŁļé┤ņŚÉņä£ ņé¼ņÜ®ņØ┤ ņ¢┤ļĀżņÜ░ļéś ņ╣ĖĻĘĖļĀÉļ¤¼ļŖö Ēŗ░ļĪ£Ēö╝ļ░śņØ┤ļéś ņĢ▒Ēŗ░Ēö╝ļ░öĒāĆņØ┤ļō£ņÖĆ ļ╣äĻĄÉĒĢśņŚ¼ ņŚ¼ļ¤¼ Ļ░Ćņ¦Ć ņןņĀÉņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ļŗż. ņ╣ĖĻĘĖļĀÉļ¤¼ļŖö ņäĖ ņĢĮņĀ£ ņżæ ņ£ĀņØ╝ĒĢśĻ▓ī P2Y12ļź╝ ĒŖ╣ņØ┤ņĀüņ£╝ļĪ£ ņ¢ĄņĀ£ĒĢśĻ│Ā, ņŗĀņןņ£╝ļĪ£ ļ░░ņäżļÉśņ¦Ć ņĢŖĻĖ░ ļĢīļ¼ĖņŚÉ ņŗĀĻĖ░ļŖźņŚÉ ļö░ļØ╝ Ēł¼ņŚ¼ ņÜ®ļ¤ēņØä ņĪ░ņĀłĒĢĀ ĒĢäņÜöĻ░Ć ņŚåņ£╝ļ®░, Ļ░Ćņן ļ░śĻ░ÉĻĖ░Ļ░Ć ņ¦¦Ļ│Ā(3-5ļČä) ņŻ╝ņ×ģ ņóģļŻī 1ņŗ£Ļ░ä ņØ┤ļé┤ņŚÉ ĒśłņåīĒīÉ ĻĖ░ļŖźņØ┤ ĒÜīļ│ĄļÉ£ļŗż. ļśÉĒĢ£, Ļ┤ĆļÅÖļ¦źņÜ░ĒÜīņłĀņØä ņŗ£Ē¢ēĒĢ£ ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ņŗ£Ē¢ēļÉ£ ļ¼┤ņ×æņ£ä ņŚ░ĻĄ¼(BRIDGE, bridging antiplatelet therapy with cangrelor in patients undergoing cardiac surgery)ņŚÉņä£ļÅä ņČ£Ēśł ņé¼Ļ▒┤ņØś ņ”ØĻ░ĆņŚåņØ┤ ņČ®ļČäĒĢ£ ĒśłņåīĒīÉ ņØæņ¦æ ņ¢ĄņĀ£ ĒÜ©Ļ│╝ļź╝ ļ│┤ņśĆļŗż[35]. ņ╣ĖĻĘĖļĀÉļ¤¼ņØś ļ╣äņÜ®Ļ│╝ Ļ▓ĮĻĄ¼ P2Y12 ņłśņÜ®ņ▓┤ ņ¢ĄņĀ£ņĀ£ņØś ņ¦ĆņåŹ ņŗ£Ļ░äņØä Ļ│ĀļĀżĒĢśņŚ¼ ĒöäļØ╝ņłśĻĘĖļĀÉ(prasugrel) ņżæļŗ© 3-4ņØ╝ ņØ┤Ēøä, Ēŗ░ņ╣┤ĻĘĖļĀÉļ¤¼ (ticagrelor) ļ░Å Ēü┤ļĪ£Ēö╝ļÅäĻĘĖļĀÉ(clopidogrel) ņżæļŗ© 2-3ņØ╝ ņØ┤Ēøä ņĢĮņĀ£ Ēł¼ņŚ¼ļź╝ ņŗ£ņ×æĒĢśņŚ¼ ņłśņłĀ ņŗ£ņ×æ 1-6ņŗ£Ļ░ä ņĀä ņżæļŗ©ĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż[36]. ņłśņłĀ Ēøä Ļ▓ĮĻĄ¼ ĒĢŁĒśłņåīĒīÉņĀ£ Ēł¼ņŚ¼Ļ░Ć Ļ░ĆļŖźĒĢ┤ņ¦Ćļ®┤ Ēŗ░ņ╣┤ĻĘĖļĀÉļ¤¼ļéś ĒöäļØ╝ņłśĻĘĖļĀÉļ│┤ļŗżļŖö Ēü┤ļĪ£Ēö╝ļÅäĻĘĖļĀÉņØä ņé¼ņÜ®ĒĢśļŖö Ļ▓āņØ┤ ņČ£Ēśł ņ£äĒŚś Ļ░Éņåīļź╝ ņ£äĒĢ┤ ņĀüņĀłĒĢśĻ│Ā ĒĢŁĒśłņåīĒīÉņĀ£ ņ×¼Ļ░£ ņŗ£ ļČĆĒĢś ņÜ®ļ¤ēņØä Ēł¼ņŚ¼ Ēøä ņ£Āņ¦Ć ņÜ®ļ¤ēņØä ņé¼ņÜ®ĒĢśļÅäļĪØ ĒĢ£ļŗż[36].
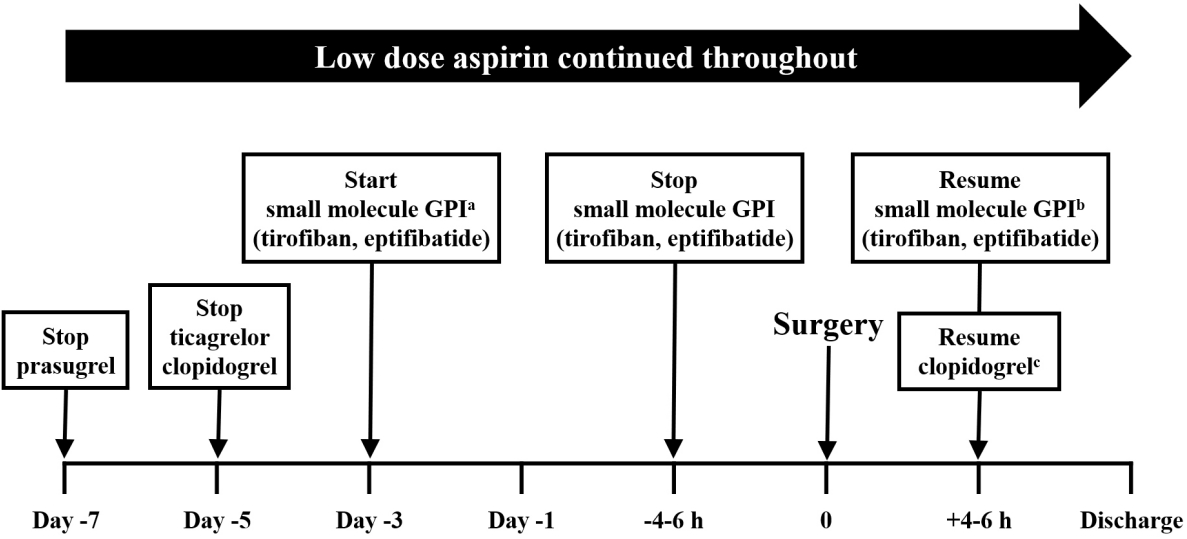
Ēŗ░ļĪ£Ēö╝ļ░śĻ│╝ ņĢ▒Ēŗ░Ēö╝ļ░öĒāĆņØ┤ļō£ļŖö glycoprotein IIb/IIIa ņłśņÜ®ņ▓┤ ņ¢ĄņĀ£ņĀ£ļĪ£ P2Y12 ņłśņÜ®ņ▓┤ļź╝ ņ¦üņĀæņĀüņ£╝ļĪ£ ņ¢ĄņĀ£ĒĢśņ¦Ć ņĢŖņ£╝ļ®░ ņ×æņÜ® ņŗ£Ļ░äņØ┤ļéś ņŗĀĻĖ░ļŖźņŚÉ ļö░ļØ╝ ņÜ®ļ¤ē ņĪ░ņĀłņØ┤ ĒĢäņÜöĒĢśļŗż. Ēŗ░ļĪ£Ēö╝ļ░śņØĆ 0.1 ╬╝g/kg/min, ņĢ▒Ēŗ░Ēö╝ļ░öĒāĆņØ┤ļō£ļŖö 2.0 ╬╝g/kg/minļź╝ Ēł¼ņŚ¼ĒĢśļ®░ Ēü¼ļĀłņĢäĒŗ░ļŗī ņ▓Łņåīņ£©(creatinine clearance)ņØ┤ 50 mL/min ņØ┤ĒĢśņØ╝ Ļ▓ĮņÜ░ ņĀłļ░śņ£╝ļĪ£ Ļ░Éļ¤ēĒĢśņŚ¼ ņé¼ņÜ®ĒĢ£ļŗż(Fig. 1). Ēł¼ņŚ¼ ņŗ£ņ×æņĀÉņØĆ ņ╣ĖĻĘĖļĀÉļ¤¼ņÖĆ ļÅÖņØ╝ĒĢśļ®░ ņłśņłĀ ņŗ£ņ×æ 4-6ņŗ£Ļ░ä ņĀä ņżæļŗ©ĒĢśĻ│Ā, ņŗĀĻĖ░ļŖź ņĀĆĒĢś ņåīĻ▓¼ņØ┤ ņ׳ļŗżļ®┤ ņĢĮņĀ£ļź╝ ļŹö ļ╣©ļ”¼ ņżæļŗ©(8-12ņŗ£Ļ░ä)ĒĢśļÅäļĪØ ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż[10]. ĒĢśņ¦Ćļ¦ī, ņØ┤ ņĢĮņĀ£ļōżņØś ĒÜ©Ļ│╝ļź╝ ņ”Øļ¬ģĒĢ£ ņŚ░ĻĄ¼ļŖö ļ╣äĻĄÉņĀü ĻĘ╝Ļ▒░ ņłśņżĆņØ┤ ņĢĮĒĢ£ ņåīĻĘ£ļ¬© ņĀäĒ¢źņĀü ņŚ░ĻĄ¼, ĒøäĒ¢źņĀü ņŚ░ĻĄ¼ ļśÉļŖö ļ®öĒāĆņŚ░ĻĄ¼ļ░¢ņŚÉļŖö ņŚåņ¢┤ Ēśäņ×¼ Ēæ£ņżĆņ╣śļŻīņ¦Ćņ╣©ņØĆ ņĀäļ¼ĖĻ░Ć ĻČīĻ│Āņé¼ĒĢŁ ņĀĢļÅäņØś ĻĘ╝Ļ▒░ ņłśņżĆļ¦ī ņĀ£ņŗ£ĒĢśĻ│Ā ņ׳ļŗż[10].
ņŖżĒģÉĒŖĖ ņéĮņ×ģ ĒÖśņ×ÉņŚÉņä£ ņłśņłĀ ņŗ£ ĒĢŁĒśłņåīĒīÉņĀ£ ņĪ░ņĀł
ļ╣äņØæĻĖēņłśņłĀ
ņłśņłĀņØś ņóģļźśļéś ņŖżĒģÉĒŖĖ ņéĮņ×ģņłĀ ļŗ╣ņŗ£ ĒÖśņ×ÉņØś ņāüĒÖ®ņŚÉ ļö░ļØ╝ ļŗżņ¢æĒĢ£ ļ│ĆņłśĻ░Ć ļ░£ņāØĒĢĀ ņłś ņ׳ņ¢┤ ņłśņłĀ ņĀäĒøä ĒĢŁĒśłņåīĒīÉņĀ£ ņé¼ņÜ® ļ░Å ņżæļŗ©ņØä Ļ░äļŗ©Ē׳ ņĀĢņØśĒĢśļŖö Ļ▓āņØĆ ļ¦żņÜ░ Ēלļōżļŗż. ļīĆĻ░£ļŖö ņłśņłĀņØä ļ»ĖļŻ░ ņłś ņ׳ļŗżļ®┤ P2Y12 ņłśņÜ®ņ▓┤ ņ¢ĄņĀ£ņĀ£ļź╝ ņżæļŗ©ĒĢĀ ņłś ņ׳ņØä ņĀĢļÅäļĪ£ ĒśłņĀä ņ£äĒŚśņØ┤ ļé«ņĢäņ¦ä Ēøä ņĢäņŖżĒö╝ļ”░ņØä ņ£Āņ¦ĆĒĢśļ®┤ņä£ ņłśņłĀĒĢśļŖö Ļ▓āņØ┤ ņóŗļŗż[14]. Ēü┤ļĪ£Ēö╝ļÅäĻĘĖļĀÉņØ┤ļéś ĒöäļØ╝ņłśĻĘĖļĀÉņØĆ P2Y12 ņłśņÜ®ņ▓┤ņŚÉ ļ╣ä Ļ░ĆņŚŁņĀüņ£╝ļĪ£ Ļ▓░ĒĢ®ĒĢśļ»ĆļĪ£ ņĢĮņĀ£Ļ░Ć Ļ▓░ĒĢ®ĒĢ£ ĒśłņåīĒīÉņØś ņłśļ¬ģņØ┤ ļŗż ĒĢĀ ļĢīĻ╣īņ¦Ć ĒśłņåīĒīÉ ĻĖ░ļŖź ņ¢ĄņĀ£Ļ░Ć ņ£Āņ¦ĆļÉ£ļŗż. Ēü┤ļĪ£Ēö╝ļÅäĻĘĖļĀÉņØĆ 5-7ņØ╝, ĒöäļØ╝ņłśĻĘĖļĀÉņØĆ 7-10ņØ╝ ņĀĢļÅäņØś ņżæļŗ© ĻĖ░Ļ░äņØ┤ ĒĢäņÜöĒĢśļŗż. Ēŗ░ņ╣┤ĻĘĖļĀÉļ¤¼ļŖö P2Y12 ņłśņÜ®ņ▓┤ņŚÉ Ļ░ĆņŚŁņĀüņ£╝ļĪ£ Ļ▓░ĒĢ®ĒĢśĻ│Ā ļ░śĻ░ÉĻĖ░Ļ░Ć ņāüļīĆņĀüņ£╝ļĪ£ ņ¦¦ņĢä(6-12ņŗ£Ļ░ä), Ēü┤ļĪ£Ēö╝ļÅäĻĘĖļĀÉņØ┤ļéś ĒöäļØ╝ņłśĻĘĖļĀÉļ│┤ļŗż ļ╣Āļź┤Ļ▓ī ĒĢŁĒśłņåīĒīÉ ĒÜ©Ļ│╝Ļ░Ć ņé¼ļØ╝ņ¦äļŗż(3-5ņØ╝) [36]. ņ£Āļ¤Įņŗ¼ņןĒĢÖĒÜī Ēæ£ņżĆņ╣śļŻīņ¦Ćņ╣©ņØĆ P2Y12 ņ¢ĄņĀ£ņĀ£ņØś ņĄ£ņåī ņżæļŗ© ĻĖ░Ļ░äņØä Ēŗ░ņ╣┤ĻĘĖļĀÉļ¤¼ļŖö 3ņØ╝, Ēü┤ļĪ£Ēö╝ļÅäĻĘĖļĀÉņØĆ 5ņØ╝, ĒöäļØ╝ņłśĻĘĖļĀÉņØĆ 7ņØ╝ļĪ£ ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż[14]. ļ░śļ®┤, ņØ┤Ēāłļ”¼ņĢäņŚÉņä£ ļ░£Ēæ£ļÉ£ ņłśņłĀ ņĀä ĒĢŁĒśłņåīĒīÉņĀ£ ĻČīĻ│ĀņĢłņŚÉņä£ļŖö Ēü┤ļĪ£Ēö╝ļÅäĻĘĖļĀÉĻ│╝ Ēŗ░ņ╣┤ĻĘĖļĀÉļ¤¼ļŖö 5ņØ╝, ĒöäļØ╝ņłśĻĘĖļĀÉņØĆ 7ņØ╝ ņĀĢļÅäņØś ņżæļŗ© ĻĖ░Ļ░äņØä ņĀ£ņŗ£ĒĢśĻ│Ā ņ׳ļŗż[10]. Ļ│╝Ļ▒░ņŚÉļŖö ļæÉĻ░£ļé┤ ļśÉļŖö ņ▓ÖņłśĻ░Ģļé┤ ņŗĀĻ▓ĮņÖĖĻ│╝ ņłśņłĀņØ┤ļéś ņÜöļÅäļź╝ ĒåĄĒĢ£ ņĀäļ”ĮņäĀņĀłņĀ£ņłĀĻ│╝ Ļ░ÖņØ┤ ņČ£Ēśł ņ£äĒŚśņØ┤ ļ¦żņÜ░ ļåÆņØĆ ņłśņłĀņŚÉņä£ļ¦ī ņśłņÖĖņĀüņ£╝ļĪ£ ņĢäņŖżĒö╝ļ”░ ņżæļŗ©ņØä ĻČīĻ│ĀĒĢśņśĆņ¦Ćļ¦ī, ņĄ£ĻĘ╝ ļ░£Ēæ£ļÉ£ ĻČīĻ│ĀņĢłņŚÉņä£ļŖö ņČ£Ēśł ņ£äĒŚśņŚÉ ļö░ļØ╝ ļ│┤ļŗż ļ¦ÄņØĆ ņłśņłĀņŚÉņä£ ņĢäņŖżĒö╝ļ”░ ņżæļŗ©ņØä Ļ│ĀļĀżĒĢĀ ņłś ņ׳ļŗżĻ│Ā ĻĖ░ņłĀĒĢśņśĆļŗż(Supplementary Table 2) [37,38]. ĻĄŁļé┤ņŚÉņä£ ņŗ£Ē¢ēļÉ£ ņŚ░ĻĄ¼ļōżņŚÉņä£ļŖö DAPTļź╝ ņżæļŗ©ĒĢśļŹöļØ╝ļÅä ņł£ņ£ĀĒĢ┤ ņ×äņāüņé¼ Ļ▒┤(net adverse clinical event)ņØä ņ”ØĻ░Ćņŗ£Ēéżņ¦Ć ņĢŖļŖöļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż. ĒĢśņ¦Ćļ¦ī, ĒĢŁĒśłņåīĒīÉņĀ£ļź╝ ņןĻĖ░Ļ░ä ņżæļŗ©ĒĢĀ Ļ▓ĮņÜ░ MACEņØś ņ£äĒŚśļÅäĻ░Ć ņ”ØĻ░ĆĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż[39,40]. ļ╣äņŗ¼ņןņłśņłĀņØ┤ ĒĢäņÜöĒĢ£ DAPT ņé¼ņÜ®ņ×ÉņØś ņłśņłĀ ņĀäĒøä ņĢĮņĀ£ ņĪ░ņĀłņŚÉ ļīĆĒĢ£ Ļ░£ņÜöļŖö ĻĘĖļ”╝ 2ņŚÉ ļéśĒāĆļé┤ņŚłļŗż.
ņØæĻĖēņłśņłĀ
ņØæĻĖēņłśņłĀ(urgent surgery)ņØĆ 48ņŗ£Ļ░ä ļé┤ņŚÉ ņłśņłĀņØ┤ ĒĢäņÜöĒĢ£ Ļ▓ĮņÜ░ļź╝ ņØśļ»ĖĒĢ£ļŗż. DAPTļź╝ ņé¼ņÜ® ņżæņØĖ ĒÖśņ×ÉņŚÉņä£ļŖö ņØ┤ ĻĖ░Ļ░ä ļÅÖņĢł ņĢĮņĀ£ļź╝ ņżæļŗ©ĒĢśļŹöļØ╝ļÅä ĒśłņåīĒīÉ ņ¢ĄņĀ£ ĒÜ©Ļ│╝Ļ░Ć ļé©ņĢäņ׳ĻĖ░ ļĢīļ¼ĖņŚÉ Ļ│╝ļÅäĒĢ£ ņČ£ĒśłņŚÉ ļīĆĒĢ£ ļīĆļ╣äĻ░Ć ĒĢäņÜöĒĢśļŗż. Ēśäņ×¼ ĒśłņåīĒīÉ ņ¢ĄņĀ£ ņ×æņÜ®ņØä ņŚŁņĀäņŗ£Ēé¼ ņłś ņ׳ļŖö ņĢĮņĀ£Ļ░Ć ņŚåĻĖ░ ļĢīļ¼ĖņŚÉ ņČ£Ēśł ņ£äĒŚśņØ┤ ļåÆņØĆ ĒÖśņ×ÉņŚÉņä£ļŖö ĒśłņåīĒīÉ ņłśĒśłņØä Ļ│ĀļĀżĒĢ┤ ļ│╝ ņłś ņ׳ļŗż. ĒĢśņ¦Ćļ¦ī, ņłśņłĀ Ēøä ņČ£Ēśł ņé¼Ļ▒┤ņØä ņśłļ░®ĒĢśĻ▒░ļéś ņČ£Ēśł ņé¼Ļ▒┤ņØ┤ ļ░£ņāØĒĢ£ ĒÖśņ×ÉņŚÉņä£ ĒśłņåīĒīÉ ĻĖ░ļŖźņØä ĒÜīļ│ĄĒĢĀ ņłś ņ׳ļŖö ņłśĒśłļ¤ēņŚÉ Ļ┤ĆĒĢ£ ņŚ░ĻĄ¼ ņ×ÉļŻīļŖö ļČĆņĪ▒ĒĢśļŗż[10]. ĒĢŁĒśłņåīĒīÉņĀ£Ļ░Ć ņłśĒśłļÉ£ ĒśłņåīĒīÉņØś ĻĖ░ļŖźļÅä ņ¢ĄņĀ£ĒĢĀ ņłś ņ׳ņ£╝ļ»ĆļĪ£ ĒśłņåīĒīÉ ņłśĒśłņØĆ ļÉśļÅäļĪØ ņĢĮņĀ£ņØś ĒÖ£ņä▒ ļīĆņé¼ ņé░ļ¼╝ (active metabolites)ņØ┤ ĒśłņżæņŚÉ ņ×öļźśĒĢśļŖö ļÅÖņĢłņØĆ ņé¼ņÜ®ĒĢśņ¦Ć ņĢŖļŖö Ļ▓āņØ┤ ņóŗļŗż. Ēü┤ļĪ£Ēö╝ļÅäĻĘĖļĀÉĻ│╝ ĒöäļØ╝ņłśĻĘĖļĀÉņØś ĒÖ£ņä▒ ļīĆņé¼ ņé░ļ¼╝ņØĆ 6ņŗ£Ļ░ä, Ēŗ░ņ╣┤ĻĘĖļĀÉļ¤¼ņŚÉņä£ļŖö 10-12ņŗ£Ļ░ä ļÅÖņĢł ĒśłņżæņŚÉ ņ×öļźśĒĢśļ»ĆļĪ£ Ēü┤ļĪ£Ēö╝ļÅäĻĘĖļĀÉņØ┤ļéś ĒöäļØ╝ņłśĻĘĖļĀÉņØ┤ ņé¼ņÜ®ļÉ£ Ļ▓ĮņÜ░ļŖö ļ¦łņ¦Ćļ¦ē ņĢĮļ¼╝ ņäŁņĘ© Ēøä 4-6ņŗ£Ļ░ä ņØ┤Ēøä, Ēŗ░ņ╣┤ĻĘĖļĀÉļ¤¼ ņé¼ņÜ®ņ×ÉņŚÉņä£ļŖö 10-12ņŗ£Ļ░ä ņØ┤ĒøäņŚÉ ĒśłņåīĒīÉ ņłśĒśłņØä ņŗ£Ē¢ēĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż[10].
ņłśņłĀ Ēøä ĒĢŁĒśłņåīĒīÉņĀ£ņØś ņ×¼Ļ░£
ņĢäņŖżĒö╝ļ”░ņØä ņżæļŗ©ĒĢ£ Ļ▓ĮņÜ░ ņłśņłĀ ņóģļŻī Ēøä ņ”ēņŗ£ ņĢĮņĀ£ļź╝ ņ×¼Ļ░£ĒĢśļÅäļĪØ ĒĢ£ļŗż. ņĄ£ĻĘ╝ ņŗ£Ē¢ēļÉ£ ĻĄŁļé┤ ņŚ░ĻĄ¼ņŚÉņä£ļŖö DESļź╝ ņéĮņ×ģ Ēøä ļ╣äņŗ¼ņןņłśņłĀņØä ņŗ£Ē¢ēĒĢ£ ĒÖśņ×ÉņŚÉņä£ 8ņØ╝ ņØ┤ņāü ņĢäņŖżĒö╝ļ”░ņØä ņżæļŗ©ĒĢĀ Ļ▓ĮņÜ░ ņ×äņāü Ļ▓ĮĻ│╝ļź╝ ņ£ĀņØśĒĢśĻ▓ī ņĢģĒÖöņŗ£ĒéżļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż[38]. ņłśņłĀ Ēøä ņĪ░ĻĖ░ņŚÉļŖö ņČ£ĒśłņØś ņ£äĒŚśņØ┤ ļåÆĻĖ░ ļĢīļ¼ĖņŚÉ ĒöäļØ╝ņłśĻĘĖļĀÉņØ┤ ļéś Ēŗ░ņ╣┤ĻĘĖļĀÉļ¤¼ļ│┤ļŗżļŖö Ēü┤ļĪ£Ēö╝ļÅäĻĘĖļĀÉņØä ņé¼ņÜ®ĒĢśņŚ¼ņĢ╝ ĒĢśļ®░, ņłśņłĀ Ēøä 24-72ņŗ£Ļ░ä ņØ┤ļé┤ņŚÉ ņŗ¼ĒĢ£ ņČ£ĒśłņØś ņ£äĒŚśņØ┤ ņŚåļŗżļ®┤ ļČĆĒĢśņÜ®ļ¤ē(600 mg)ņØä ņé¼ņÜ®ĒĢśņŚ¼ ņ×¼Ļ░£ĒĢśļÅäļĪØ ĒĢ£ļŗż[35]. ĒĢśņ¦Ćļ¦ī, ņłśņłĀ Ēøä ņ×äņāüņĀüņ£╝ļĪ£ ņŻ╝ņØśļź╝ ņÜöĒĢśļŖö ņČ£ĒśłņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ņŚÉļŖö ĒĢŁĒśłņåī ĒīÉņĀ£ņØś ņ×¼Ļ░£ļź╝ ļ»ĖļŻ©ņ¢┤ņĢ╝ ĒĢ£ļŗż[10].
ņłśņłĀ ņĀä ĒĢŁņØæĻ│ĀņĀ£ ņĪ░ņĀł
ņØ╝ļ░ś ņøÉņ╣Ö
Ļ▓ĮĻĄ¼ĒśĢ ĒĢŁņØæĻ│ĀņĀ£ļŖö ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£(vitamin K antagonist, VKA)ņÖĆ ĒŖ╣ņĀĢ ņØæĻ│ĀņØĖņ×Éļź╝ ņäĀĒāØņĀüņ£╝ļĪ£ ņ¢ĄņĀ£ĒĢśļŖö non-vitamin K antagonist oral anticoagulants (NOAC)ļĪ£ ļČäļźśļÉ£ļŗż. NOACņØĆ direct oral anticoagulant (DOAC), target-specific oral anticoagulant (TSOC) ļō▒ņ£╝ļĪ£ļÅä ļČłļ”░ļŗż. ĒŖĖļĪ¼ļ╣ł(thrombin)ņØä ņŻ╝ Ēæ£ņĀüņ£╝ļĪ£ ĒĢśļŖö ļŗżļ╣äĻ░ĆĒŖĖļ×Ć(dabigatran)Ļ│╝ 10ļ▓ł ņØæĻ│ĀņØĖņ×É(Factor Xa)ļź╝ Ēæ£ņĀüņ£╝ļĪ£ ĒĢśļŖö Xa ņ¢ĄņĀ£ņĀ£ņØĖ ļ”¼ļ░öļĪØņé¼ļ░ś(rivaroxaban), ņĢäĒöĮņé¼ļ░ś (apixaban) ļ░Å ņŚÉļÅģņé¼ļ░ś(edoxaban) ļō▒ņØ┤ Ēśäņ×¼ ņé¼ņÜ®ļÉśĻ│Ā ņ׳ļŗż. ņÖĆĒīīļ”░(warfarin)ņØĆ ļīĆĒæ£ņĀüņØĖ VKAļĪ£ ļ░śĻ░ÉĻĖ░ļŖö 36ņŗ£Ļ░äņØ┤ļ®░ ļ╣ä ņŗ¼ņןņłśņłĀņØ┤ Ļ│äĒÜŹļÉ£ Ļ▓ĮņÜ░ ņłśņłĀ 5ņØ╝ ņĀä ņżæļŗ©ĒĢ┤ņĢ╝ ĒĢ£ļŗż[41]. Vitamin K ņØśņĪ┤ĒśĢ ņ×æņÜ® ĻĖ░ņĀäņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ņ¢┤ ņĀĢļ¦źņŻ╝ņé¼ĒśĢ vitamin KĻ░Ć ņŚŁņĀäņĀ£ļĪ£ ņé¼ņÜ®ļÉ£ļŗż. NOACņØś ļ░śĻ░ÉĻĖ░ļŖö ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØ┤ 12-17ņŗ£Ļ░äņ£╝ļĪ£ Ļ░Ćņן ĻĖĖĻ│Ā ļ”¼ļ░öļĪØņé¼ļ░śņØ┤ 5-9ņŗ£Ļ░äņ£╝ļĪ£ Ļ░Ćņן ņ¦¦ļŗż[42]. NOAC ņé¼ņÜ®ņ×ÉļōżņŚÉņä£ ņłśņłĀņØ┤ ĒĢäņÜöĒĢ£ Ļ▓ĮņÜ░ ņČ£ĒśłņØś ņ£äĒŚśļÅäņÖĆ ņŗĀĻĖ░ļŖźņŚÉ ļö░ļØ╝ ņĢĮļ¼╝ ņżæļŗ© ĻĖ░Ļ░äņØä Ļ▓░ņĀĢĒĢ£ļŗż(Fig. 3). ņŗĀņןņ£╝ļĪ£ 80% ņØ┤ņāü ļ░░ņČ£ļÉśļŖö ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØĆ Ēü¼ļĀłņĢäĒŗ░ļŗī ņ▓Łņåīņ£© 50 mL/minļź╝ ĻĖ░ņżĆņ£╝ļĪ£ ļŗżļźĖ NOACņØĆ 30 mL/minļź╝ ĻĖ░ņżĆņ£╝ ļĪ£ ņżæļŗ© ĻĖ░Ļ░äņØä Ļ▓░ņĀĢĒĢ£ļŗż(Fig. 3) [41].
ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£
VKAļź╝ ņØ┤ņÜ®ĒĢ£ Ļ▓ĮĻĄ¼ ĒĢŁņØæĻ│ĀņĀ£ļź╝ ņé¼ņÜ® ņżæņØĖ ĒÖśņ×ÉļŖö ņłśņłĀ ņĀäĒøä ņČ£Ēśł ņ£äĒŚśņØ┤ ņ”ØĻ░ĆĒĢ£ļŗż. ņłśņłĀ ņĀä ņŗ£Ē¢ēĒĢ£ international normalized ratio (INR) Ōēż 1.5ņØ┤ļ®┤ ņłśņłĀņØä ņĢłņĀäĒĢśĻ▓ī ņłśĒ¢ēĒĢĀ ņłś ņ׳ļŗż[41,42]. ĒĢśņ¦Ćļ¦ī, ĒśłņĀäņāēņĀäņ”ØņØś ņ£äĒŚśņØ┤ ļåÆņØĆ ņĢäļלņÖĆ Ļ░ÖņØĆ ĒÖśņ×ÉļōżņŚÉņä£ VKAņØś ņżæļŗ©ņØĆ ņ£äĒŚśĒĢśļ®░ ļ╣äļČäĒÜŹ ĒŚżĒīīļ”░ (unfractionated heparin, UFH) ļśÉļŖö ņ╣śļŻī ņÜ®ļ¤ēņØś ņĀĆļČäņ×Éļ¤ē ĒŚżĒīīļ”░(low molecular weight heparin, LMWH)ņØä ņé¼ņÜ®ĒĢ£ Ļ░ĆĻĄÉņÜöļ▓ĢņØ┤ ĒĢäņÜöĒĢśļŗż[43].
1. CHA2DS2-VASc ņĀÉņłśĻ░Ć 4ņĀÉ ņØ┤ņāüņØĖ ņŗ¼ļ░®ņäĖļÅÖ
2. ĻĖ░Ļ│ä ņŗ¼ņןĒīÉļ¦ē, ņāłļĪ£ ņéĮņ×ģļÉ£ ņāØņ▓┤ ņŗ¼ņןĒīÉļ¦ē ņ¦łĒÖś ĒÖśņ×É
3. ņĄ£ĻĘ╝ 3Ļ░£ņøö ņØ┤ļé┤ ņŖ╣ļ¬©ĒīÉņ×¼Ļ▒┤ņłĀņØä ļ░øņØĆ ĒÖśņ×É
4. ņĄ£ĻĘ╝ 3Ļ░£ņøö ņØ┤ļé┤ ņĀĢļ¦źĒśłņĀäņāēņĀäņ”ØņØ┤ ļ░£ņāØĒĢ£ ĒÖśņ×É
5. ĒśłņĀäņä▒Ē¢źņ”Ø(thrombophilia) ĒÖśņ×É
Ļ░ĆĻĄÉņÜöļ▓ĢņØä ņŗ£Ē¢ēĒĢĀ Ļ▓ĮņÜ░, ĒśłņĀäņāēņĀäņ”Ø ņ£äĒŚśņØ┤ ļåÆņØĆ ĒÖśņ×ÉļŖö ĒĢśļŻ© 2ĒÜī ņ╣śļŻī ņÜ®ļ¤ēņØś LMWH ņé¼ņÜ®ņØ┤ ĻČīņןļÉśĻ│Ā ņ£äĒŚśņØ┤ ļé«ņØĆ ĒÖśņ×ÉņØś Ļ▓ĮņÜ░ ļ¦żņØ╝ 1ĒÜī ņśłļ░® ņÜ®ļ¤ē ņé¼ņÜ®ņØ┤ ĒĢäņÜöĒĢśļŗż[10,13]. LMWHņØś ļ¦łņ¦Ćļ¦ē ņÜ®ļ¤ēņØĆ ņłśņłĀ 12ņŗ£Ļ░ä ņØ┤ņĀäņŚÉ Ēł¼ņŚ¼ļÉśņ¢┤ņĢ╝ ĒĢśļ®░ ņżæļō▒ļÅä ņØ┤ņāüņØś ņŗĀņן ĻĖ░ļŖź ņןņĢĀĻ░Ć ņ׳ļŖö ĒÖśņ×ÉņŚÉņä£ļŖö Ēł¼ņŚ¼ ņÜ®ļ¤ēņØś ņĪ░ņĀĢņØ┤ ĒĢäņÜöĒĢśļŗż[44]. VKA ņé¼ņÜ®ņØĆ ņłśņłĀ ņĀä 3-5ņØ╝Ļ░ä ņżæļŗ©ĒĢśļ®░ INR Ōēż 1.5ņŚÉ ļÅäļŗ¼ĒĢĀ ļĢīĻ╣īņ¦Ć ļ¦żņØ╝ INRņØä ņĖĪņĀĢĒĢśĻ│Ā, VKA ņżæļŗ© Ēøä 24ņŗ£Ļ░ä Ēøä ļśÉļŖö INR < 2.0ņØ┤ ļÉśļŖö ņ”ēņŗ£ LMWH ļśÉļŖö UFH ņÜöļ▓ĢņØä ņŗ£ņ×æĒĢśļŖö Ļ▓āņØä ĻČīĻ│ĀĒĢ£ļŗż[10,13].
VKAļź╝ ņé¼ņÜ® ņżæņØĖ ĒÖśņ×ÉņŚÉĻ▓ī ņłśņłĀņØä ņŗ£Ē¢ēĒĢĀ Ļ▓ĮņÜ░ ņČ£Ēśł ņ£äĒŚśņØ┤ ņāüļŗ╣Ē׳ ļåÆņ£╝ļ®░ ņ¦ĆĒśł Ļ│╝ņĀĢņŚÉļÅä ņśüĒ¢źņØä ļ»Ėņ╣śĻĖ░ ļĢīļ¼ĖņŚÉ ņŗ£Ē¢ēļÉśļŖö ņłśņłĀņØ┤ļéś ņŗ£ņłĀņØś ņ£ĀĒśĢņŚÉ ļö░ļØ╝ Ļ░ĆĻĄÉņÜöļ▓Ģ ņĀüņÜ® ņŚ¼ļČĆļź╝ ĒīÉļŗ©ĒĢ┤ņĢ╝ ĒĢ£ļŗż. ņČ£Ēśł ņ£äĒŚśņØ┤ ļåÆņØĆ ņłśņłĀņØ╝ Ļ▓ĮņÜ░ Ļ▓ĮĻĄ¼ ĒĢŁņØæĻ│ĀņĀ£ņØś ņżæļŗ© ļ░Å LMWHļź╝ ņØ┤ņÜ®ĒĢ£ Ļ░ĆĻĄÉņÜöļ▓ĢņØä ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØ┤ ĻČīĻ│ĀļÉśļéś ļ░▒ļé┤ņן ļśÉļŖö Ļ▓Įļ»ĖĒĢ£ Ēö╝ļČĆ ņłśņłĀĻ│╝ Ļ░ÖņØ┤ ņČ£Ēśł ņ£äĒŚśņØ┤ ļé«ņØĆ ņłśņłĀņŚÉņä£ļŖö Ļ▓ĮĻĄ¼ ĒĢŁņØæĻ│ĀņĀ£ļź╝ ņ£Āņ¦ĆĒĢśļ®┤ņä£ ņ¦äĒ¢ēĒĢśļŖö Ļ▓āņØä ĻČīĻ│ĀĒĢ£ļŗż[44]. ĻĘĖļ¤¼ļéś ņØ┤ļ¤¼ĒĢ£ Ļ▓ĮņÜ░ņŚÉļÅä INRņØĆ ļé«ņØĆ ņ╣śļŻī ļ▓öņ£äļź╝ ņ£Āņ¦ĆĒĢśļŖö Ļ▓āņØ┤ ļ░öļ×īņ¦üĒĢśļŗż[44].
NOAC
ĒĢŁņØæĻ│ĀņĀ£ļź╝ ņé¼ņÜ® ņżæņØĖ ĒÖśņ×Éļōż ņżæ ļ¦ÄņØĆ ņłśĻ░Ć ņżæņ×¼ņŗ£ņłĀ ļśÉļŖö ņłśņłĀļĪ£ ņØĖĒĢ┤ ĒĢ┤ļŗ╣ ņĢĮņĀ£ļź╝ ņØ╝ņŗ£ņĀüņ£╝ļĪ£ ņżæļŗ©ĒĢ┤ņĢ╝ ĒĢ£ļŗż. ņŚ¼ļ¤¼ ņ£ĀĻ┤Ć ĒĢÖĒÜīļōżņØ┤ NOACņØś ņé¼ņÜ®Ļ│╝ ņżæļŗ©ņŚÉ Ļ┤ĆĒĢ£ ļ│äļÅäņØś Ēæ£ņżĆņ╣śļŻī ņ¦Ćņ╣©ņØä ņĀ£ņŗ£ĒĢśĻ│Ā ņ׳ļŗż[10,13,45]. ņłśņłĀ ņóģļźśņŚÉ ļö░ļØ╝ ņČ£Ēśł ņ£äĒŚśņØ┤ ļŗżļź┤ļ»ĆļĪ£ ņłśņłĀņØś ņóģļźś ļ░Å ĒÖśņ×ÉļōżņØś ĒŖ╣ņä▒(ĒÖśņ×ÉņØś ņŗĀĻĖ░ļŖź ļō▒)ņØä ņóģĒĢ®ĒĢśņŚ¼ ĒĢŁņØæĻ│ĀņĀ£ņØś ņżæļŗ© ņŗ£ņĀÉņØä Ļ▓░ņĀĢĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż[45]. NOAC ņé¼ņÜ®ņ×ÉņØś ņłśņłĀ ņĀäĒøä ņĢĮņĀ£ ņĪ░ņĀĢņŚÉ ļīĆĒĢ£ Ļ░£ņÜöļŖö ĻĘĖļ”╝ 3ņŚÉ ļéśĒāĆļé┤ņŚłļŗż.
ņČ£ĒśłņØś ņ£äĒŚśņØ┤ Ļ▓Įļ»ĖĒĢ£(minor bleeding risk) ņłśņłĀņØ┤ļéś ņŗ£ņłĀņØ┤ ĒĢäņÜöĒĢ£ Ļ▓ĮņÜ░ ĒĢŁņØæĻ│ĀņĀ£ļź╝ ņ£Āņ¦ĆĒĢśļ®┤ņä£ ņłśņłĀ ļśÉļŖö ņŗ£ņłĀņØä ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØä ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż[45]. ļ░£ņ╣ś, ņ╣śņŻ╝ņłśņłĀ, ļ░▒ļé┤ņןņØ┤ļéś ļģ╣ļé┤ņןņłśņłĀ, ņĪ░ņ¦üĻ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖļŖö ļé┤ņŗ£Ļ▓ĮĻ▓Ćņé¼ ļō▒ņØ┤ ņČ£ĒśłņØś ņ£äĒŚśņØ┤ Ļ▓Įļ»ĖĒĢ£ ņłśņłĀņŚÉ ĒżĒĢ©ļÉ£ļŗż(Supplementary Table 3). ņØ┤ļ¤¼ĒĢ£ ņłśņłĀ ļ░Å ņŗ£ņłĀņØĆ ļ¦łņ¦Ćļ¦ē NOACņØä ļ│ĄņÜ® Ēøä 12-24 ņŗ£Ļ░ä ĒøäņŚÉ ņŗ£Ē¢ēĒĢĀ ņłś ņ׳ņ£╝ļ®░ ĒĢ┤ļŗ╣ ņ╣śļŻī Ēøä 6ņŗ£Ļ░äņØ┤ Ļ▓ĮĻ│╝ĒĢśļ®┤ ĒĢŁņØæĻ│ĀņĀ£ļź╝ ņ×¼Ļ░£ĒĢĀ ņłś ņ׳ļŗż[45].
ņČ£ĒśłņØś ņ£äĒŚśņØ┤ ļé«ņØĆ(low bleeding risk) ņłśņłĀņØ┤ļéś ņŗ£ņłĀņØ┤ ĒĢäņÜöĒĢ£ Ļ▓ĮņÜ░ ņŗĀĻĖ░ļŖźņØ┤ ņĀĢņāüņØĖ ĒÖśņ×ÉņŚÉņä£ļŖö 24ņŗ£Ļ░ä ņĀäņŚÉ NOACņØä ņżæļŗ©ĒĢśĻ│Ā, ņŗĀņןĻĖ░ļŖźņŚÉ ņØ┤ņāüņØ┤ ņ׳ļŖö ĒÖśņ×ÉļŖö ņØ┤ļ│┤ļŗż ļŹö ņØ┤ļźĖ ņŗ£Ļ░ä(48ņŗ£Ļ░ä ņĀä)ņŚÉ ņżæļŗ©ĒĢśļŖö Ļ▓āņØ┤ ņóŗļŗż[45]. ņĪ░ņ¦üĻ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśļŖö ļé┤ņŗ£Ļ▓Į ņŗ£ņłĀ, ņĀäļ”ĮņäĀņØ┤ļéś ļ░®Ļ┤æ ņĪ░ņ¦üĻ▓Ćņé¼, ļ░ĢļÅÖĻĖ░ Ēś╣ņØĆ ICD ņéĮņ×ģņłĀ ļō▒ņØ┤ ņØ┤ņŚÉ ņåŹĒĢ£ļŗż(Supplementary Table 3; Fig. 3) [45].
ļ¦łņ¦Ćļ¦ēņ£╝ļĪ£, ņČ£ĒśłņØś ņ£äĒŚśņØ┤ ļåÆņØĆ(high bleeding risk) ņŗ£ņłĀņØ┤ļéś ņłśņłĀņØä ņ¦äĒ¢ēĒĢĀ Ļ▓ĮņÜ░ ņłśņłĀ 48ņŗ£Ļ░ä ņĀäņŚÉ NOAC ņżæļŗ©ņØä ņČöņ▓£ĒĢśļ®░ ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØä ņé¼ņÜ® ņżæņØĖ ņŗĀĻĖ░ļŖź ņןņĢĀ ĒÖśņ×ÉļŖö 48ņŗ£Ļ░ä ņØ┤ņāü NOACņØä ņżæļŗ©ĒĢ┤ņĢ╝ ĒĢ£ļŗż. ļīĆļČĆļČäņØś ļ│ĄĻ░Ģ ļé┤ ņłśņłĀ, ĒØēĻ░Ģ ļé┤ ņłśņłĀ, ņ▓ÖņČö ļ¦łņĘ© ĒĢś ņŗ£ņłĀ ļō▒ņØ┤ ņØ┤ņŚÉ ĒżĒĢ©ļÉ£ļŗż(Supplementary Table 3) [45]. NOACņØä ņé¼ņÜ®ĒĢśļŖö ĒÖśņ×ÉļōżņŚÉĻ▓īļŖö ĒŚżĒīīļ”░ņØä ņØ┤ņÜ®ĒĢ£ Ļ░ĆĻĄÉņÜöļ▓ĢņØĆ ņČöņ▓£ļÉśņ¦Ć ņĢŖļŖöļŗż. ņØ┤ļŖö NOACņØś ņśłņĖĪ Ļ░ĆļŖźĒĢ£ ņĢĮļĀźĒĢÖņĀü ĒŖ╣ņä▒, ņ¦¦ņØĆ ļ░śĻ░ÉĻĖ░ ļ░Å ļ╣ĀļźĖ ĒĢŁņØæĻ│ĀĒÜ©Ļ│╝ ņŚŁņĀä ņŗ£Ļ░ä ļō▒ņØś ĒŖ╣ņä▒ ļĢīļ¼ĖņØ┤ļŗż. NOAC ņé¼ņÜ®ņ×ÉļōżņØä ļīĆņāüņ£╝ļĪ£ ņŗ£Ē¢ēļÉ£ ņ×äņāü ņŚ░ĻĄ¼ņŚÉņä£ļÅä Ļ░ĆĻĄÉņÜöļ▓ĢņØĆ ņČ£ĒśłņØś ņ£äĒŚśļÅäļ¦ī ņ”ØĻ░Ćņŗ£Ēé¼ ļ┐É ĒśłņĀä ņé¼Ļ▒┤ņØĆ ņżäņØ┤ņ¦Ć ļ¬╗ĒĢśņśĆļŗż[46].
ņłśņłĀ Ēøä Ļ▓ĮĻĄ¼ ĒĢŁņØæĻ│ĀņĀ£ņØś ņ×¼Ļ░£
ņłśņłĀ Ēøä VKAļź╝ ņØ┤ņÜ®ĒĢ£ ĒĢŁņØæĻ│ĀņÜöļ▓ĢņØś ņ×¼Ļ░£ Ļ│╝ņĀĢņØĆ ļŗżņØīĻ│╝ Ļ░Öļŗż. LMWH ļśÉļŖö UFHļŖö ĒÖśņ×ÉņØś ņ¦ĆĒśł ņāüĒā£ņŚÉ ļö░ļØ╝ ņłśņłĀ Ēøä 1-2ņØ╝ ĒøäņŚÉ ņłśņłĀ ņĀä ņé¼ņÜ®ĒĢśļŹś ņÜ®ļ¤ēņ£╝ļĪ£ ļŗżņŗ£ ņŗ£ņ×æĒĢ£ļŗż. VKA ļŖö ņ▓śņØī 2ņØ╝ ļÅÖņĢłņØĆ ņłśņłĀ ņĀä ņ£Āņ¦Ć ņÜ®ļ¤ēņØś 1.5ļ░░ ņÜ®ļ¤ēņØä ņé¼ņÜ®ĒĢśĻ│Ā, ņØ┤ Ēøä ņłśņłĀ ņĀä ņ£Āņ¦Ć ņÜ®ļ¤ēņØä Ēł¼ņŚ¼ĒĢ┤ņĢ╝ ĒĢ£ļŗż. INRņØ┤ ņ╣śļŻī ņłśņżĆņ£╝ļĪ£ ĒÜīļ│ĄļÉĀ ļĢīĻ╣īņ¦Ć LMWH ļśÉļŖö UFHļź╝ Ļ│äņåŹ ļ│æņÜ® Ēł¼ņŚ¼ĒĢ┤ņĢ╝ ĒĢ£ļŗż.
ņłśņłĀ Ēøä ņÖäņĀäĒĢ£ ņ¦ĆĒśłņØ┤ ņØ┤ļŻ©ņ¢┤ņĪīļŗżļ®┤ NOACņØĆ ņŗ£ņłĀ Ēøä 6-8ņŗ£Ļ░ä ņØ┤Ēøä ņé¼ņÜ® Ļ░ĆļŖźĒĢśļŗż. ĒĢśņ¦Ćļ¦ī, ņØ╝ļČĆ ņłśņłĀņŚÉņä£ļŖö ņłśņłĀ ņØ┤Ēøä 48-72ņŗ£Ļ░ä ņØ┤ļé┤ņŚÉ NOACņØä ņ×¼Ļ░£ĒĢĀ Ļ▓ĮņÜ░ ņČ£Ēśł ņ£äĒŚśņØ┤ ņāüņŖ╣ĒĢĀ ņłś ņ׳ņ£╝ļ®░ ļ¦łļ╣äņä▒ ņןĒÅÉņćä ļō▒ņØś ĒĢ®ļ│æņ”Øņ£╝ļĪ£ Ļ▓ĮĻĄ¼ ņĢĮņĀ£ Ēł¼ņŚ¼Ļ░Ć ļČłĻ░ĆļŖźĒĢ£ Ļ▓ĮņÜ░ļÅä ļ░£ņāØĒĢĀ ņłś ņ׳ļŗż. ņØ┤ļ¤¼ĒĢ£ ņāüĒÖ®ņŚÉņä£ļŖö ĒŚżĒīīļ”░ ļō▒ņØś ļ╣äĻ▓ĮĻĄ¼ņĢĮļ¼╝ņØä ņØ┤ņÜ®ĒĢ£ ĒĢŁĒśłņĀäņĀ£ ņśłļ░®ņÜöļ▓ĢņØä ņŗ£Ē¢ēĒĢ£ ĒøäņŚÉ NOACņØä ļŗżņŗ£ ņŗ£ņ×æĒĢśļŖö Ļ▓āņØä ĻČīĻ│ĀĒĢ£ļŗż. Ļ░ü ņĢĮņĀ£ ļ│äļĪ£ ņłśņłĀ ņĀä ņĢĮņĀ£ ņżæļŗ© ņŗ£ņĀÉĻ│╝ ņ×¼Ļ░£ ņŗ£Ļ░äņØĆ Fig. 4ņŚÉ ļéśĒāĆļé┤ ņŚłļŗż[45].
NOACņØä ļ│ĄņÜ® ņżæņØĖ ĒÖśņ×ÉņŚÉņä£ ņØæĻĖēņłśņłĀņØ┤ ĒĢäņÜöĒĢ£ Ļ▓ĮņÜ░
ņ”ēĻ░üņłśņłĀ(immediate procedures)
ņłś ļČäļé┤ņŚÉ ņłśņłĀņØś Ļ▓░ņĀĢņØ┤ ņØ┤ļŻ©ņ¢┤ņĀĖņĢ╝ ĒĢśļŖö ņ”ēĻ░üņłśņłĀ(ņśł, ņ”ēĻ░üņĀüņØĖ ņāØļ¬ģ/ņé¼ņ¦Ć/ņןĻĖ░ļź╝ ĻĄ¼ĒĢśļŖö ņłśņłĀ, ĒŖ╣Ē׳ ņŗ¼ņן/ĒśłĻ┤Ć/ņŗĀĻ▓Į ņÖĖĻ│╝ņĀü ņØæĻĖēņłśņłĀ)ņØ┤ ĒĢäņÜöĒĢĀ Ļ▓ĮņÜ░ ĒĢŁņØæĻ│ĀņĀ£ ĒÜ©Ļ│╝Ļ░Ć ņåīņŗżļÉĀ ļĢīĻ╣īņ¦Ć ņłśņłĀņØä ņŚ░ĻĖ░ĒĢĀ ņłś ņŚåļŗż. ņżæļō▒ļÅä-ņżæņ”ØņØś ņČ£Ēśł ņ£äĒŚśņØ┤ ņ׳ļŖö ņłśņłĀņŚÉņä£ļŖö ņłśņłĀ ņĀä ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØś ņŚŁņĀäņĀ£ņØĖ ņØ┤ļŗżļŻ©ņŗ£ņŻ╝ļ¦Ö (idarucizumab)ņØä Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢ£ļŗż[47]. ĒĢśņ¦Ćļ¦ī, Xa ņ¢ĄņĀ£ņĀ£ņØś ņŚŁņĀäņĀ£ņØĖ ņĢłļŹ▒ņé¼ļäżņØ┤ĒŖĖ-ņĢīĒīī(andexanate-╬▒)ļŖö ņØæĻĖēņłśņłĀ ĒÖśņ×ÉņŚÉņä£ ņĢĮļ¼╝ ĒÜ©ņÜ®ņä▒ņØ┤ ĒÖĢļ”ĮļÉśņ¢┤ ņ׳ņ¦Ć ņĢŖņ£╝ļ®░, ĻĄŁļé┤ņŚÉņä£ļŖö ņØ┤ ņĢĮņĀ£ļź╝ ņĢäņ¦ü ņ×äņāüņŚÉņä£ ņé¼ņÜ®ĒĢĀ ņłś ņŚåļŗż. ļśÉĒĢ£, ĒÜ©Ļ│╝ņÖĆ ņĢłņĀäņä▒ ļŹ░ņØ┤Ēä░ļŖö ļČĆņĪ▒ĒĢśņ¦Ćļ¦ī ļ╣äĒŖ╣ņØ┤ņĀü ņØæĻ│ĀņØĖņ×É ļåŹņČĢļ¼╝(prothrombin complex concentrate, PCC) Ēł¼ņŚ¼ļź╝ Ļ│ĀļĀżĒĢ┤ļ│╝ ņłś ņ׳ņ£╝ļéś ĻĄŁļé┤ņŚÉļŖö Ēśäņ×¼ PCCĻ░Ć ĒŚłĻ░ĆļÉśņ¦Ć ņĢŖņĢä ņé¼ņÜ®ĒĢĀ ņłś ņŚåļŗż[45].
ĻĖ┤ĻĖēņłśņłĀ(urgent procedures)
ņłśņłĀņØ┤ Ļ▓░ņĀĢļÉ£ Ēøä ņłś ņŗ£Ļ░ä ņØ┤ļé┤ņŚÉ ņŗżĒ¢ēņØ┤ ņÜöĻĄ¼ļÉśļŖö ĻĖ┤ĻĖē ņłśņłĀ(ņśł, ņ×Āņ×¼ņĀüņ£╝ļĪ£ ņāØļ¬ģņØä ņ£äĒśæĒĢśļŖö ņāüĒā£ņØś ĻĖēņä▒ ļ░£ļ│æ ļśÉļŖö ņ×äņāüņĀü ņĢģĒÖöņŚÉ ņØśĒĢ£ ņżæņ×¼ņĀü ņłśņłĀ, ņé¼ņ¦Ć/ņןĻĖ░ņØś ņāØņĪ┤ ļ░Å Ļ│©ņĀłņØś ĻĄÉņĀĢ, ĒåĄņ”Ø ņÖäĒÖö ļśÉļŖö ĻĖ░ĒāĆ ņ”ØņāüņØä ņ£äĒśæĒĢĀ ņłś ņ׳ļŖö ņāüĒā£)ņØĆ ņłśņłĀ ļśÉļŖö ņŗ£ņłĀņØä ņĀüņ¢┤ļÅä 12ņŗ£Ļ░ä(Ļ░ĆļŖźĒĢśļŗżļ®┤ ļ¦łņ¦Ćļ¦ē NOAC Ēł¼ņŚ¼ Ēøä 24ņŗ£Ļ░ä) ņĀĢļÅä ņŚ░ĻĖ░ĒĢśļŖö Ļ▓āņØ┤ ĻČīņןļÉ£ļŗż. ļśÉĒĢ£, ņŚŁņĀäņĀ£ ļśÉļŖö PCCņØś ņé¼ņÜ® ņŚ¼ļČĆļź╝ Ļ▓░ņĀĢĒĢśĻĖ░ ņ£äĒĢśņŚ¼ ĒśłņĢĪņØæĻ│Ā Ļ▓Ćņé¼ Ļ▓░Ļ│╝(prothrombin time [PT], activated partial thromboplastin time [aPTT], anti-FXa assay, diluted thrombin time [dTT] ļō▒)ļź╝ ĒÖĢņØĖĒĢ┤ ļæÉļŖö Ļ▓āņØ┤ ņóŗļŗż[45].
ņŗĀņåŹņłśņłĀ(expedite procedures)
ņłśņłĀ Ļ▓░ņĀĢ Ēøä ņłśņØ╝ ļé┤ņŚÉ ņŗżĒ¢ēņØ┤ ņÜöĻĄ¼ļÉśļŖö ņŗĀņåŹņłśņłĀ(ņāØļ¬ģ/ņé¼ņ¦Ć/ņןĻĖ░ ņāØņĪ┤ņŚÉ ņ£äĒśæņØ┤ ļÉśņ¦Ć ņĢŖļŖö ņĪ░ĻĖ░ ņ╣śļŻīĻ░Ć ĒĢäņÜöĒĢ£ Ļ▓ĮņÜ░)ņØ┤ ĒĢäņÜöĒĢ£ Ļ▓ĮņÜ░ NOACņØś ņżæļŗ© ņŚ¼ļČĆļŖö ļ╣äņØæĻĖēņłśņłĀņØś ĻĖ░ņżĆņØä ļö░ļźĖļŗż[45].
Ļ▓░ ļĪĀ
ņłśņłĀ ļ░Å ņŗ£ņłĀ ņŗ£ ĒĢŁĒśłņĀäņĀ£ņØś ņĪ░ņĀłņØĆ ņłśņłĀņŚÉ ļö░ļźĖ ņČ£Ēśł ņ£äĒŚśļÅäņÖĆ ņłśņłĀ ņĀäĒøä ĒśłņĀä ņ£äĒŚśļÅäļź╝ ņóģĒĢ®ņĀüņ£╝ļĪ£ ĒÅēĻ░ĆĒĢśņŚ¼ Ļ▓░ņĀĢĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż. ļīĆļČĆļČäņØś ņłśņłĀ ļ░Å ņŗ£ņłĀ ņŗ£Ē¢ē ņŗ£ ņĢäņŖżĒö╝ļ”░ņØĆ ņ£Āņ¦ĆĒĢśļŖö Ļ▓āņØ┤ ņøÉņ╣ÖņØ┤ļŗż. DAPTļź╝ ņżæļŗ©ĒĢĀ Ļ▓ĮņÜ░ ĒśłņĀä ņ£äĒŚśņØ┤ ļ¦żņÜ░ ļåÆņØĆ ĒÖśņ×ÉņŚÉņä£ ņČ£Ēśł ņ£äĒŚśņØ┤ ļåÆņØĆ ņłśņłĀņØä ņŗ£Ē¢ēĒĢ┤ņĢ╝ ĒĢĀ Ļ▓ĮņÜ░ ņĀĢļ¦źņŻ╝ņé¼ĒśĢ ĒĢŁĒśłņåīĒīÉņĀ£ļź╝ ņØ┤ņÜ®ĒĢ£ Ļ░ĆĻĄÉņÜöļ▓ĢņØä ņĀüņÜ®ĒĢĀ ņłś ņ׳ļŗż. VKAļŖö ņłśņłĀ 5ņØ╝ ņĀä ņżæļŗ©ĒĢ┤ņĢ╝ ĒĢśļ®░ NOACņØĆ ņČ£Ēśł ņ£äĒŚśļÅäņŚÉ ļö░ļØ╝ ņłśņłĀ 24-48ņŗ£Ļ░ä ņĀä ņżæļŗ©ĒĢśļŖö Ļ▓āņØ┤ ņøÉņ╣ÖņØ┤ļŗż. ĒĢśņ¦Ćļ¦ī, ņāüĻĖ░ ņ¦Ćņ╣©ņØĆ ņČ®ļČäĒĢ£ Ļ┤ĆļĀ© ņŚ░ĻĄ¼ļź╝ ĒåĄĒĢ┤ ĒÖĢļ”ĮļÉ£ Ļ▓āņØ┤ ņĢäļŗłļ»ĆļĪ£ Ē¢źĒøä ļ¼┤ņ×æņ£ä ņŚ░ĻĄ¼ļź╝ ĒåĄĒĢ┤ ĒåĄņØ╝ļÉ£ ņ╣śļŻīņ¦Ćņ╣©ņØä ļ¦łļĀ©ĒĢśĻĖ░ ņ£äĒĢ£ ļģĖļĀźņØ┤ ĒĢäņÜöĒĢśļŗż.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






