


ņä£ ļĪĀ
ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø(functional dyspepsia)ņØĆ ņåīĒÖöņä▒ ĻČżņ¢æ, ņ£äņןĻ┤Ć ņĢģņä▒ņóģņ¢æ, ņ£äņŗØļÅäņŚŁļźś ņ¦łĒÖś ļśÉļŖö ņĘīļŗ┤ļÅä ņ¦łĒÖśĻ│╝ Ļ░ÖņØĆ ĻĖ░ņ¦łņĀüņØĖ ņ¦łĒÖśņØ┤ ņŚåņ£╝ļ®┤ņä£ ņ£äņןĻ┤Ć ņ”ØņāüņØ┤ ļ¦īņä▒ņĀü, ļ░śļ│ĄņĀüņ£╝ļĪ£ ļéśĒāĆļéśļŖö ņ”Øņāüņ”ØĒøäĻĄ░ņØ┤ļŗż. ņĀäĒśĢņĀüņØĖ ņ”Øņāüņ£╝ļĪ£ļŖö ļČłņŠīĒĢ£ ņŗØĒøä Ēżļ¦īĻ░É(bothersome postprandial fullness, ņ£ä ļé┤ņŚÉ ņØīņŗØņØ┤ Ļ│äņåŹ ļé©ņĢäņ׳ļŖö Ļ▓ā Ļ░ÖņØĆ ļČłĒÄĖĒĢ£ ņ”Øņāü), ļČłņŠīĒĢ£ ņĪ░ĻĖ░ ļ¦īļ│ĄĻ░É(bothersome early satiation, ņŗØņé¼ļź╝ ņŗ£ņ×æĒĢśņ×É Ļ│¦ ļ░░Ļ░Ć ļČĆļź┤Ļ│Ā ļŹö ņØ┤ņāü ņŗØņé¼ļź╝ ĒĢĀ ņłś ņŚåļŖö ļŖÉļéī), ļČłņŠīĒĢ£ ņāüļ│ĄļČĆ ĒåĄņ”Ø(bothersome epigastric pain)Ļ│╝ ļČłņŠīĒĢ£ ņāüļ│ĄļČĆ ņō░ļ”╝(bothersome epigastric burning)ņØ┤ ņ׳ļŗż. 2006ļģä Ļ░£ņĀĢļÉ£ ļĪ£ļ¦łĻĖ░ņżĆ IIIņŚÉ ļö░ļź┤ļ®┤ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØĆ ļæÉ Ļ░Ćņ¦Ć ņĢäĒśĢ, ņ”ē ņŗØĒøäĻ│ĀĒåĄņ”ØĒøäĻĄ░(postprandial distress syndrome, PDS)Ļ│╝ ļ¬ģņ╣śĒåĄņ”Øņ”ØĒøäĻĄ░(epigastric pain syndrome, EPS)ņ£╝ļĪ£ ļéśļēśĻ│Ā[1], ņØ┤ļŖö ļĪ£ļ¦łĻĖ░ņżĆ IVņŚÉņä£ļÅä ņ▒äĒāØļÉśņŚłļŗż[2]. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ļæÉ ņĢäĒśĢņØĆ ļ│æĒā£ņāØļ”¼ĻĖ░ņĀäņØ┤ ļŗżļź┤ļŗżĻ│Ā ņČöņĀĢļÉśļ®░ ņØ┤ņŚÉ ļö░ļØ╝ ņ╣śļŻī ņĀæĻĘ╝ļÅä ņ░©ņØ┤Ļ░Ć ņ׳ļŗż. ņŗØņé¼ Ēøä ņ£äņØś ņĀüņØæņןņĢĀ(dysaccommodation), ņ¦ĆņŚ░ļÉ£ ņ£ä ļ░░ņČ£(delayed gastric emptying)Ļ│╝ ļé┤ņן Ļ│╝ļ»╝ņä▒(visceral hypersensitivity)ņØ┤ EPSņÖĆ PDS ļ¬©ļæÉņŚÉ Ļ┤ĆņŚ¼ĒĢśļ®░, EPSņÖĆ PDSĻ░Ć ļÅÖņŗ£ņŚÉ ņ׳ļŖö ņżæļ│Ąņ”ØĒøäĻĄ░ņØś ĒśĢĒā£ļĪ£ ļéśĒāĆļéśĻĖ░ļÅä ĒĢ£ļŗż[2].
ņåīĒÖöļČłļ¤ē ņ”ØņāüņØ┤ ņ׳ļŖö ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ┤ļĪ£ļ”¼(Helicobacter pylori, H. pylori) ņ£äņŚ╝ ĒÖśņ×ÉņŚÉņä£ ņÜ░ņäĀņĀüņ£╝ļĪ£ ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ĒĢśĻ│Ā 6Ļ░£ņøö Ēøä ņ”Øņāü ĒśĖņĀäņØ┤ ņŚåļŖö Ļ▓ĮņÜ░ļź╝ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Øņ£╝ļĪ£ ņĀĢņØśĒĢśļŖö ĻĄÉĒåĀ ĒĢ®ņØśļŖö ĻĄŁļé┤ ņä▒ņØĖņØś ļåÆņØĆ H. pylori ņ£Āļ│æļźĀ(~50%)Ļ│╝ ĒĢŁņāØņĀ£, ĒŖ╣Ē׳ clarithromycinņØś ļåÆņØĆ ļé┤ņä▒ņ£©ņØä Ļ░ÉņĢłĒĢĀ ļĢī, ĻĄŁļé┤ņŚÉņä£ ņłśņÜ®ĒĢśĻĖ░ņŚÉļŖö ĻĘĖ ĻĘ╝Ļ▒░Ļ░Ć ļČĆņĪ▒ĒĢśļŗż[3-5].
2005ļģäņŚÉ ļīĆĒĢ£ņåīĒÖöĻĖ░ĻĖ░ļŖźņä▒ņ¦łĒÖś┬ĘņÜ┤ļÅÖĒĢÖĒÜīļŖö ņĀäļ¼ĖĻ░Ć ņØśĻ▓¼ņØä ļ░öĒāĢņ£╝ļĪ£ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ņ¦äļŗ©Ļ│╝ ņ╣śļŻīņŚÉ ļīĆĒĢ£ ņ¦äļŻī ņ¦Ćņ╣©ņØä ļ░£Ēæ£ĒĢśņśĆĻ│Ā[6], 2011ļģäņŚÉ ņŗżņĀ£ ņ×äņāüņŚÉņä£ ņé¼ņÜ®ļÉĀ ņłś ņ׳ļÅäļĪØ ņ▓┤Ļ│äņĀü ļ¼ĖĒŚīĻ│Āņ░░ņØä ĒåĄĒĢśņŚ¼ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ņ╣śļŻīņŚÉ ļīĆĒĢ£ ņ¦äļŻī ņ¦Ćņ╣©ņØä Ļ░£ņĀĢĒĢśņśĆļŗż[7]. ņØ┤Ēøä ņČĢņĀüļÉ£ ĻĘ╝Ļ▒░ļź╝ ļ░öĒāĢņ£╝ļĪ£ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ņ¦äļŗ©Ļ│╝ ņ╣śļŻīņŚÉ ļīĆĒĢśņŚ¼ ņ¦äļŻī ņ¦Ćņ╣©ņØä Ļ░£ņĀĢĒĢśņŚ¼ 2019ļģä ņśüļ¼ĖĒīÉņ£╝ļĪ£ ņČ£Ļ░äĒĢśĻ▓ī ļÉśņŚłļŗż[8]. Ļ░£ņĀĢņĢłņØś ĒŖ╣ņ¦ĢņØĆ ņ▓½ņ¦Ė, ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ņ╣śļŻīņŚÉ ļīĆĒĢ£ ņ▓┤Ļ│äņĀüņØĖ ļ¼ĖĒŚī Ļ▓ĆņāēĻ│╝ ĻĘ╝Ļ▒░ ĒÅēĻ░Ćļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż. ņ¢æņä▒ņ×ÉĒÄīĒöäņ¢ĄņĀ£ņĀ£(proton pump inhibitor, PPI)ņØś ĒÜ©Ļ│╝, H. pylori ņĀ£ĻĘĀ ņ╣śļŻīņØś ņ£ĀņÜ®ņä▒, ņé╝ĒÖśĻ│ä ĒĢŁņÜ░ņÜĖņĀ£(tricyclic antidepressant, TCA)ņØś ĒÜ©Ļ│╝ņŚÉ ļīĆĒĢśņŚ¼ ļ®öĒāĆļČäņäØņØä ņŗżņŗ£ĒĢśņŚ¼ ĻĘ╝Ļ▒░ļź╝ ņĀ£ņŗ£ĒĢśņśĆļŗż. ļæśņ¦Ė, ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ņĢäĒśĢ(EPS, PDS)ņŚÉ ļö░ļźĖ ĻČīĻ│Āļ¼ĖņØä ņĀ£ņŗ£ĒĢśņśĆļŗż. ņģŗņ¦Ė, H. pyloriĻ░Ć ņåīĒÖöļČłļ¤ē ĒśĖņĀäņŚÉ ļ»Ėņ╣śļŖö ĒÜ©Ļ│╝ļź╝ ņä£ņ¢æĻ│╝ ļÅÖņ¢æņŚÉņä£ ņŗ£Ē¢ēļÉ£ ņŚ░ĻĄ¼ļź╝ ĻĄ¼ļČäĒĢśņŚ¼ ļ®öĒāĆļČäņäØņØä ņŗżņŗ£ĒĢśņśĆļŗż. ļäĘņ¦Ė, ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£ņØś ĒÜ©Ļ│╝ļ┐É ņĢäļŗłļØ╝ ļČĆņ×æņÜ®ņŚÉ ļīĆĒĢ£ ĻČīĻ│ĀņĢłņØä ĒåĄĒĢśņŚ¼ ņŗżņĀ£ ņ×äņāüņŚÉņä£ ņŻ╝ņØśĒĢĀ ņé¼ĒĢŁņØä ņĀ£ņŗ£ĒĢśņśĆļŗż.
Ļ░£ņĀĢ Ļ│╝ņĀĢņØĆ JNMņŚÉ ņČ£Ļ░äļÉ£ ņśüļ¼ĖĒīÉņŚÉ ņ×ÉņäĖĒ׳ ĻĖ░ņłĀĒĢśņśĆļŗż[8]. ņäĀņĀĢļÉ£ ļ¼ĖĒŚī ņżæ ļ¼┤ņ×æņ£ä ļīĆņĪ░ņŗ£ĒŚś(randomized controlled trials, RCT)ņØś ĒÄĖĒ¢ź ņ£äĒŚś(risk of bias)ņŚÉ ļīĆĒĢśņŚ¼ ņ¦łĒÅēĻ░Ćļź╝ ņŗżņŗ£ĒĢśņśĆļŗż[9]. ĻČīĻ│ĀņĢłņØś ĻČīĻ│Ā ļō▒ĻĖēĻ│╝ ņ”ØĻ▒░ ņłśņżĆņØĆ ņłśņĀĢļÉ£ Grading of Recommendations Assessment, Development, and EvaluationņØä ņØ┤ņÜ®ĒĢśņŚ¼ Ļ▓░ņĀĢĒĢśņśĆļŗż(Table 1) [10]. ĻČīĻ│ĀņĢł ņ┤łņĢłņŚÉ ļīĆĒĢśņŚ¼ ņłśņĀĢ ļŹĖĒīīņØ┤ ļ░®ļ▓Ģņ£╝ļĪ£ ņĀäļ¼ĖĻ░Ć ĒĢ®ņØś ļÅäņČ£ņØä ņŗżņŗ£ĒĢśņśĆļŗż[11]. Ļ░£ņĀĢņĢłņØĆ ņ┤Ø 14Ļ░£ņØś ĻČīĻ│ĀņĢłņ£╝ļĪ£ ņØ┤ļŻ©ņ¢┤ņĪīņ£╝ļ®░, ņ╣śļŻīņŚÉ Ļ┤ĆļĀ©ļÉ£ 9Ļ░£ ĻČīĻ│ĀņĢłņŚÉ ļīĆĒĢśņŚ¼ 27ļ¬ģņØś ņåīĒÖöĻĖ░ļé┤Ļ│╝ ņĀäļ¼ĖņØśĻ░Ć Ēł¼Ēæ£ĒĢśņŚ¼ 7Ļ░£ņØś ĻČīĻ│ĀņĢł ļīĆĒĢ┤ņä£ ĒĢ®ņØśļź╝ ļÅäņČ£ĒĢśņśĆļŗż. ļ│ĖĻ│ĀņŚÉņä£ļŖö ņØ┤ļ▓ł Ļ░£ņĀĢļÉ£ ņśüļ¼ĖĒīÉ ņ¦äļŻī ņ¦Ćņ╣©ņØä ņÜöņĢĮ ņĀĢļ”¼ĒĢśņŚ¼ ņåīĻ░£ĒĢśĻ│Āņ×É ĒĢ£ļŗż. Ļ░ü ĻČīĻ│ĀņĢłņØś ņÜöņĢĮņØä Ēæ£ 2ņŚÉ ņĀĢļ”¼ĒĢśņśĆļŗż.
ņåīĒÖöļČłļ¤ēņØś ņĀĢņØś
ņåīĒÖöļČłļ¤ēņØĆ ņāüļČĆņ£äņןĻ┤ĆņŚÉ ļéśĒāĆļéśļŖö ņ”Øņāüņ£╝ļĪ£, ļĪ£ļ¦łĻĖ░ņżĆ IVļŖö ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØä ļČłņŠīĒĢ£ ņŗØĒøä Ēżļ¦īĻ░É, ļČłņŠīĒĢ£ ņĪ░ĻĖ░ ļ¦īļ│ĄĻ░É, ļČłņŠīĒĢ£ ņāüļ│ĄļČĆ ĒåĄņ”Ø, ļČłņŠīĒĢ£ ņāüļ│ĄļČĆ ņō░ļ”╝ ņżæ ĒĢ£ Ļ░Ćņ¦Ć ņØ┤ņāüņØś ņ”ØņāüņØ┤ ņĄ£ņåī 6Ļ░£ņøö ņĀäļČĆĒä░ ņŗ£ņ×æļÉśĻ│Ā, ņĄ£ĻĘ╝ 3Ļ░£ņøö ņØ┤ļé┤ņŚÉ ņ׳ņØä ļĢīļĪ£ ņĀĢņØśĒĢśņśĆļŗż[2]. ņåīĒÖöļČłļ¤ē ĒÖśņ×É ņ╣śļŻīņŚÉ Ļ┤ĆĒĢ£ ļ»ĖĻĄŁĻ│╝ ņ║Éļéśļŗż ņåīĒÖöĻĖ░ ņĀäļ¼ĖņØś ĒśæĒÜī ņ×äņāüņ¦Ćņ╣©ņØĆ ņåīĒÖöļČłļ¤ēņØä ņĀüņ¢┤ļÅä 1Ļ░£ņøö ņØ┤ņāü ņ¦ĆņåŹļÉśļŖö ņāüļ│ĄļČĆ ļČłĒÄĖĻ░É, ĻĄ¼ņŚŁ, ĻĄ¼ĒåĀ, Ļ░ĆņŖ┤ņō░ļ”╝Ļ│╝ Ļ░ÖņØĆ ņ”ØņāüĻ│╝ Ļ┤ĆļĀ©ņØ┤ ņ׳ļŖö ņāüļ│ĄļČĆ ĒåĄņ”Øņ£╝ļĪ£ ņĀĢņØśĒĢśņśĆļŗż[12,13]. Ēśäņ×¼ ņŚ¼ļ¤¼ ņ¦Ćņ╣©ņŚÉņä£ ņåīĒÖöļČłļ¤ēņØś ņĀĢņØśļŖö ņāüļ│ĄļČĆņØś ĒåĄņ”ØĻ│╝ ļČłĒÄĖĻ░ÉņØ┤ 1Ļ░£ņøö ņØ┤ņāüņØ┤ ņ׳ņØä ļĢīļĪ£ ņĀĢņØśĒĢśļ®░ ĻĄ¼ņ▓┤ņĀü ņ”ØņāüņØĆ ņŗØĒøä Ēżļ¦īĻ░É, ņĪ░ĻĖ░ ļ¦īļ│ĄĻ░É, ļ│ĄļČĆĒīĮļ¦ī, ĻĄ¼ņŚŁ ļśÉļŖö ĻĄ¼ĒåĀņØ┤ļŗż.
ļČłņØæņä▒ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØĆ ņĄ£ņåī 8 ņŻ╝ ņØ┤ņāü ņ”ØņāüņØ┤ ņ¦ĆņåŹļÉśĻ│Ā 2 Ļ░Ćņ¦Ć ņØ┤ņāüņØś ņ╣śļŻīņŚÉ ļ░śņØæĒĢśņ¦Ć ņĢŖņØä ļĢīļĪ£ ņĀĢņØśĒĢ£ļŗż[14]. ņĢäņŗ£ņĢä Ēā£ĒÅēņ¢æ ņ¦ĆņŚŁĻ│╝ ļ»ĖĻĄŁ ņ¦äļŻī ņ¦Ćņ╣©ņØĆ 4 ņŻ╝ ļÅÖņĢł ņ╣śļŻī ĒøäņŚÉ ņĀüņĀłĒĢ£ ņ╣śļŻī ĒÜ©Ļ│╝Ļ░Ć ļŗ¼ņä▒ļÉśņ¦Ć ņĢŖņ£╝ļ®┤ ļŗżļźĖ ņĢĮļ¼╝ļĪ£ ļ│ĆĻ▓ĮņØä ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż[15,16]. ņØ╝ļ│Ė ņ╣śļŻī ņ¦Ćņ╣©ņØĆ 1ņ░©ņĀüņ£╝ļĪ£ ņ£äņé░ ļČäļ╣äņ¢ĄņĀ£ņĀ£ņÖĆ ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£ļĪ£ ņ╣śļŻīĒĢśņŚ¼ ļ░śņØæĒĢśņ¦Ć ņĢŖļŖö Ļ▓ĮņÜ░ 2ņ░© ņ╣śļŻīļĪ£ ņĀäĒåĄņØśĒĢÖ, ĒĢŁņÜ░ņÜĖņĀ£, H. pylori ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśĻ│Ā 2ņ░© ņ╣śļŻīņŚÉļÅä ļ░śņØæĒĢśņ¦Ć ņĢŖļŖö Ļ▓ĮņÜ░ļź╝ ļČłņØæņä▒ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØ┤ļØ╝Ļ│Ā ņĀ£ņĢłĒĢśņśĆļŗż[14]. ļČłņØæņä▒ņØ┤ļØ╝Ļ│Ā ņ¦äļŗ© ļé┤ļ”¼ĻĖ░ ņ£äĒĢ┤ņä£ļŖö ņĘīļŗ┤ļÅä ņ¦łĒÖś ļ░Å ĻĖ░ĒāĆ ņāüļ│ĄļČĆ ņ”ØņāüņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ļŖö ļŗżļźĖ ĻĖ░ņ¦łņĀüņØĖ ņ¦łĒÖśņØä ļ░śļō£ņŗ£ ļ░░ņĀ£ĒĢ┤ņĢ╝ ĒĢ£ļŗż.
ņ¦äļŗ©
ņāüļČĆņ£äņןĻ┤Ć ļé┤ņŗ£Ļ▓Į
1. 40ņäĖ ņØ┤ņāüņØś ļ¦īņä▒ ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉņŚÉņä£ļŖö ĻĖ░ņ¦łņĀü ņøÉņØĖņØä ļ░░ņĀ£ĒĢśĻĖ░ ņ£äĒĢśņŚ¼ ņāüļČĆņ£äņןĻ┤Ć ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ļź╝ ņĪ░ĻĖ░ņŚÉ ņŗ£Ē¢ēĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢ£ļŗż.
ŌĆó ĻČīĻ│Ā ļō▒ĻĖē: Ļ░ĢĒĢ©
ŌĆó ņ”ØĻ▒░ ņłśņżĆ: ļé«ņØī
ŌĆó ņĀäļ¼ĖĻ░Ć ņØśĻ▓¼: ņĀäņĀüņ£╝ļĪ£ ļÅÖņØśĒĢ©(70.4%), ļīĆņ▓┤ļĪ£ ļÅÖņØśĒĢ©(29.6%), ņØ╝ļČĆ ļÅÖņØśĒĢ©(0%), ļīĆņ▓┤ļĪ£ ļÅÖņØśĒĢśņ¦Ć ņĢŖņØī(0%), ņĀäņĀüņ£╝ļĪ£ ļÅÖņØśĒĢśņ¦Ć ņĢŖņØī(0%), ļ¬©ļź┤Ļ▓ĀņØī(0%)
ļ»ĖĻĄŁĻ│╝ ņ║Éļéśļŗż ņ¦äļŻī ņ¦Ćņ╣©ņŚÉņä£ļŖö ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉņŚÉņä£ ļé┤ņŗ£Ļ▓Įļ│┤ļŗżļŖö H. pylori Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśņŚ¼ ņ¢æņä▒ņØĖ Ļ▓ĮņÜ░ ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśĻ│Ā, ņØ┤ĒøäņŚÉļÅä ņ”ØņāüņØ┤ ņ¦ĆņåŹļÉśļ®┤ ņ£äļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢ£ļŗż[17]. ņØ┤ļŖö ņĪ░ĻĖ░ņŚÉ ņāüļČĆņ£äņןĻ┤Ć ļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ēĒĢ£ Ļ▓ĮņÜ░ņÖĆ ŌĆ£H. pylori Ļ▓Ćņé¼ Ēøä ņĀ£ĻĘĀ ņ╣śļŻīŌĆØļź╝ ļ╣äĻĄÉĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ ņ”Øņāü ĒśĖņĀäņŚÉ ļ»Ėņ╣śļŖö ņśüĒ¢źņØĆ ļ╣äņŖĘĒĢśņśĆņ£╝ļéś ŌĆ£H. pylori Ļ▓Ćņé¼ Ēøä ņĀ£ĻĘĀ ņ╣śļŻīŌĆØļź╝ ņŗ£Ē¢ēĒĢ£ Ļ▓ĮņÜ░Ļ░Ć ļ╣äņÜ®-ĒÜ©Ļ│╝ņŚÉņä£ ņØ┤ļōØņØ┤ ņ׳ņŚłļŗżļŖö ņŚ░ĻĄ¼ļź╝ ĻĘ╝Ļ░äņ£╝ļĪ£ ĒĢśĻ│Ā ņ׳ļŗż[18-20]. ļśÉĒĢ£ ņĪ░ĻĖ░ņŚÉ ņ£äļé┤ņŗ£Ļ▓ĮņØä ņŗżņŗ£ĒĢ£ ĻĄ░Ļ│╝ Ļ▓ĮĒŚśņĀüņ£╝ļĪ£ ņ£äņé░ļČäļ╣äņ¢ĄņĀ£ņĀ£ļź╝ ņÜ░ņäĀņĀüņ£╝ļĪ£ ņé¼ņÜ®ĒĢ£ Ēøä ņ”Øņāü ĒśĖņĀäņŚÉ ļ»Ėņ╣śļŖö ĒÜ©Ļ│╝ļź╝ ļ╣äĻĄÉĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļÅä ņ¢æĻĄ░Ļ░ä ļ╣äņŖĘĒĢ£ ņ”Øņāü ĒśĖņĀä ņĀĢļÅäļź╝ Ļ░ĆņĀĖņÖöņ£╝ļéś ņÜ░ņäĀņĀüņ£╝ļĪ£ ņ£äņé░ļČäļ╣äņ¢ĄņĀ£ņĀ£ļź╝ ņé¼ņÜ®ĒĢśļŖö Ļ▓ĮņÜ░ ļ╣äņÜ®-ĒÜ©Ļ│╝ņŚÉņä£ ņØ┤ļōØņØ┤ ņ׳ņŚłļŗż[21,22]. ņØ┤ļŖö ļ»ĖĻĄŁņØ┤ļéś ņ║Éļéśļŗż ļō▒ ņä£ĻĄ¼ĻČīņŚÉņä£ļŖö ņĢĮņĀ£ ņé¼ņÜ®ļ╣äļ│┤ļŗż ļé┤ņŗ£Ļ▓Į ļ╣äņÜ®ņØ┤ Ēø©ņö¼ ļåÆĻĖ░ ļĢīļ¼ĖņŚÉ ļé┤ņŗ£Ļ▓ĮņØä ņÜ░ņäĀņĀüņ£╝ļĪ£ ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØ┤ ļ╣äņÜ®-ĒÜ©Ļ│╝ļ®┤ņŚÉņä£ ļČłļ”¼ĒĢśĻĖ░ ļĢīļ¼ĖņØ╝ Ļ▓āņØ┤ļŗż. ĻĘĖļ¤¼ļéś ņä£ĻĄ¼ņÖĆ ļŗ¼ļ”¼ ņĢäņŗ£ņĢäļŖö ļé┤ņŗ£Ļ▓Į ļ╣äņÜ®ņØ┤ ņĀĆļĀ┤ĒĢśĻ│Ā ļ¼┤ņŚćļ│┤ļŗżļÅä ņ£äņĢö ņ£Āļ│æļźĀņØ┤ ļåÆņ£╝ļ®░ ļ░£ļ│æ ņŚ░ļĀ╣ļÅä ļé«ĻĖ░ ļĢīļ¼ĖņŚÉ ļŗżļźĖ ņĀæĻĘ╝ņØ┤ ĒĢäņÜöĒĢśļŗż. ņżæĻĄŁņŚÉņä£ ņåīĒÖöļČłļ¤ēņ£╝ļĪ£ ļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ē ļ░øņØĆ 14,101ļ¬ģņØä ĒøäĒ¢źņĀüņ£╝ļĪ£ ļČäņäØĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ 45ņäĖ ņØ┤ĒĢśņØś Ļ▓ĮĻ│Ā ņ”Øņāü(ņ▓┤ņżæĻ░Éņåī, ņŚ░ĒĢśĻ│żļ×Ć, ņ£äņןĻ┤Ć ņČ£Ēśł, ņ▓ĀĻ▓░ĒĢŹņä▒ ļ╣łĒśł, ļ│ĄļČĆ ņóģĻ┤┤, ņ¦ĆņåŹņĀüņØĖ ĻĄ¼ĒåĀ ļō▒)ņØ┤ ņŚåļŖö ņĮöĒśĖĒŖĖņŚÉņä£ ļé┤ņŗ£Ļ▓Į ļīĆņŗĀ ŌĆ£H. pylori Ļ▓Ćņé¼ Ēøä ņĀ£ĻĘĀ ņ╣śļŻīŌĆØļź╝ ņŗ£Ē¢ēĒĢśņśĆņØä ļĢī 18ļ¬ģņØś ņ£äņĢö ĒÖśņ×É ņżæ 13ļ¬ģ(72.2%)ņØä ņ¦äļŗ©ĒĢśņ¦Ć ļ¬╗ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņČöņĀĢļÉ£ļŗż[23]. ņåīĒÖöļČłļ¤ēņ£╝ļĪ£ ļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ē ļ░øņØĆ 17,894ļ¬ģņŚÉ ļīĆĒĢ£ ļīĆļ¦īņØś ņŚ░ĻĄ¼ņŚÉņä£ļÅä ņ£äņĢö ĒÖśņ×ÉņØś 5.3% (12/225)Ļ░Ć 45ņäĖ ļ»Ėļ¦īņØ┤ņŚłĻ│Ā Ļ▓ĮĻ│Ā ņ”ØņāüņØ┤ ņŚåļŖö Ļ▓āņ£╝ļĪ£ ĒÖĢņØĖļÉśņ¢┤, Ļ▓Ćņé¼ļź╝ ļ░øņ¦Ć ņĢŖņØĆ ņåīĒÖöļČłļ¤ē(uninvestigated dyspepsia) ĒÖśņ×ÉņŚÉņä£ 40ņäĖ ņØ┤ņāüņØĖ Ļ▓ĮņÜ░ ņāüļČĆņ£äņןĻ┤Ć ļé┤ņŗ£Ļ▓ĮņØä ņÜ░ņäĀņĀüņ£╝ļĪ£ ņŗ£Ē¢ēĒĢĀ Ļ▓āņØä ņĀ£ņŗ£ĒĢśņśĆļŗż[24].
ņÜ░ļ”¼ļéśļØ╝ļŖö ņ£äņĢö ļ░£ņāØļźĀņØ┤ ļåÆļŗż[25]. 1999-2010ļģäņØś ņ×ÉļŻīņŚÉņä£ļÅä ņ£äņĢö ļ░£ņāØļźĀņØĆ 20-39ņäĖņŚÉņä£ 10ļ¦ī ņØĖļģä(person-years) ļŗ╣ ļé©ņ×É 7.40ļ¬ģ, ņŚ¼ņ×É 8.33ļ¬ģņØ┤ ļ░£ņāØĒĢśņśĆņ£╝ļ®░, 40-54ņäĖņŚÉļŖö Ļ░üĻ░ü 73.11ļ¬ģ, 35.13ļ¬ģņ£╝ļĪ£ ņ”ØĻ░ĆĒĢśņśĆļŗż[26]. International Agency for Research on CancerņØś GLOBOCAN 2012 ņ×ÉļŻīņŚÉņä£ļÅä ļéśņØ┤ņŚÉ ļö░ļźĖ ņ£äņĢöņØś Ēæ£ņżĆ ļ░£ņāØļźĀņØĆ ņØĖĻĄ¼ 10ļ¦ī ļ¬ģļŗ╣ 15-39ņäĖņŚÉ 5.7ļ¬ģņØ┤ņŚłĻ│Ā, 40-44ņäĖņŚÉļŖö 30ļ¬ģņ£╝ļĪ£ ĻĖēĻ▓®ĒĢśĻ▓ī ņ”ØĻ░ĆĒĢśņśĆļŗż. ņÜ░ļ”¼ļéśļØ╝ ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉņŚÉņä£ ļéśņØ┤ņŚÉ ļö░ļźĖ ņ£äņĢö ļ░£ņāØļźĀņØä ņĪ░ņé¼ĒĢ£ ņŚ░ĻĄ¼ļŖö ņĢäņ¦ü ņŚåļŗż. Ļ▓ĮĻ│Ā ņ”ØņāüņØ┤ ņŚåļŖö 615ļ¬ģņØś ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉņŚÉņä£ H. pylori Ļ▓Ćņé¼ņØś ņ£ĀņÜ®ņä▒ņØä ņĢīņĢäļ│Ė ĻĄŁļé┤ ņŚ░ĻĄ¼ņŚÉņä£ 40ņäĖ ņØ┤ĒĢśņŚÉņä£ļŖö H.pylori Ļ░ÉņŚ╝ ņ£Āļ¼┤ņÖĆ ļ¼┤Ļ┤ĆĒĢśĻ▓ī ņ£äņĢöņØ┤ ļ░£Ļ▓¼ļÉśņ¦Ć ņĢŖņĢśļŗż[27].
ņĄ£ĻĘ╝ H. pylori ņÖĆ ņ£äņĢö ļ░£ņāØļźĀņØ┤ ļåÆņØĆ ņĢäņŗ£ņĢäņŚÉņä£ ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉņŚÉ ļīĆĒĢ£ ņ┤łĻĖ░ ņĀæĻĘ╝ ļ░®ļ▓Ģņ£╝ļĪ£ ņĪ░ĻĖ░ņŚÉ ņāüļČĆņ£äņןĻ┤Ć ļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņŚÉ ļīĆĒĢ£ ņĀüņĀłņä▒ņØä ņé┤ĒÄ┤ļ│┤ĻĖ░ ņ£äĒĢ£ ļ®öĒāĆļČäņäØ Ļ▓░Ļ│╝, ņ£äņĢö ĒÖśņ×É ņżæ 45ņäĖ ņØ┤ĒĢśĻ░Ć 17.8%, 35ņäĖ ļ»Ėļ¦īņŚÉņä£ 3.0%Ļ░Ć ļ░£ļ│æĒĢśņŚ¼ ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢ┤ņĢ╝ ĒĢśļŖö ņĀüņĀłĒĢ£ ļéśņØ┤ļź╝ 35ņäĖļĪ£ ņĀ£ņĢłĒĢśĻĖ░ļÅä ĒĢśņśĆļŗż[24]. 2014ļģä ņÜ░ļ”¼ļéśļØ╝ ĻĄŁĻ░ĆņĢöļō▒ļĪØņé¼ņŚģ ņŚ░ļĪĆ ļ│┤Ļ│Āņä£ņŚÉņä£ ļö░ļź┤ļ®┤ ņĀäņ▓┤ ņ£äņĢö ĒÖśņ×É 29,854ļ¬ģ ņżæ 35ņäĖ ļ»Ėļ¦īņØ┤ 1.2% (353ļ¬ģ), 40ņäĖ ļ»Ėļ¦īņØ┤ 3.1% (932ļ¬ģ), 45ņäĖ ļ»Ėļ¦īņØ┤ 7.5% (2,230ļ¬ģ)ļĪ£, ņÜ░ļ”¼ļéśļØ╝ 40ņäĖ ņØ┤ņāüņØś ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉļŖö ņ£äņĢöņØ┤ ļé┤ņĀ£ļÉśņ¢┤ ņ׳ņØä Ļ░ĆļŖźņä▒ņØ┤ ļåÆļŗż. ļö░ļØ╝ņä£ 40ņäĖ ņØ┤ņāüņØś ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉņŚÉņä£ ņ£äņĢöņØä ĒżĒĢ©ĒĢ£ ĻĖ░ņ¦łņĀü ņøÉņØĖņØä ļ░░ņĀ£ĒĢśĻĖ░ ņ£äĒĢ┤ ņĪ░ĻĖ░ņŚÉ ņāüļČĆņ£äņןĻ┤Ć ļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ēĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢ£ļŗż.
ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ Ļ░ÉņŚ╝(Helicobacter pylori) ņ¦äļŗ©
2. ņé░ļČäļ╣äņ¢ĄņĀ£ņĀ£ļéś ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£ņŚÉ ļ░śņØæĒĢśņ¦Ć ņĢŖļŖö ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉĻ▓īņä£ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ┤ļĪ£ļ”¼ Ļ░ÉņŚ╝ Ļ▓Ćņé¼ļź╝ ĻČīĻ│ĀĒĢ£ļŗż.
ŌĆó ĻČīĻ│Ā ļō▒ĻĖē: ņĢĮĒĢ©
ŌĆó ņ”ØĻ▒░ ņłśņżĆ: ļ¦żņÜ░ ļé«ņØī
ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØĆ ļ│æĒā£ņāØļ”¼ĒĢÖņĀüņ£╝ļĪ£ ļŗżņ¢æĒĢ£ ņÜöņØĖļōżņØ┤ ļ│ĄĒĢ®ņĀüņ£╝ļĪ£ ņ×æņÜ®ĒĢśņŚ¼ ļ░£ĒśäļÉ£ļŗż. ņĢīļĀżņ¦ä ņÜöņØĖņ£╝ļĪ£ļŖö ņ£äņĀĆļČĆņØś ņł£ņØæļÅä Ļ░Éņåī, ņ£äļ░░ņČ£ļŖźņØś ņĀĆĒĢś, ņ£äņØś ļé┤ņן Ļ│╝ļ»╝ņä▒, ņ£äņé░ ļČäļ╣ä ņןņĢĀ, ņ£ĀņĀäņĀü ┬Ę ĒÖśĻ▓ĮņĀü ņÜöņØĖ, ņĀĢņŗĀņé¼ĒÜīņĀü ņÜöņØĖ, ņāØĒÖ£ ņŖĄĻ┤Ć ĻĘĖļ”¼Ļ│Ā H.pylori Ļ░ÉņŚ╝ ļō▒ņØ┤ ņ׳ļŗż[28]. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņŚÉņä£ H. pylori Ļ░ÉņŚ╝ņØ┤ ļ»Ėņ╣śļŖö ņśüĒ¢źņŚÉ ļīĆĒĢśņŚ¼ ļ¦ÄņØĆ ņŚ░ĻĄ¼ļōżņØ┤ ņ¦äĒ¢ēļÉśņ¢┤ ņÖöņ¦Ćļ¦ī ņĢäņ¦üĻ╣īņ¦Ć ļ¬ģĒÖĢĒĢ£ Ļ┤ĆĻ│äļŖö ļ░ØĒśĆņĀĖ ņ׳ņ¦Ć ņĢŖļŗż. H. pylori Ļ░ÉņŚ╝ņØ┤ ņ£ä ņĀÉļ¦ēņŚÉ ņŚ╝ņ”ØņØä ņ£Āļ░£ĒĢśĻ│Ā, ņØ┤ļĪ£ ņØĖĒĢ┤ ņ£äņĢĪņØś ļČäļ╣ä ļ░Å ņ£äņןņÜ┤ļÅÖĻĖ░ļŖźņŚÉ ņןņĢĀļź╝ ņ£Āļ░£ĒĢśņŚ¼ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØä ņ£Āļ░£ĒĢ£ļŗżĻ│Ā ĒĢ£ļŗż[29].
17Ļ░£ RCT (n=3,500) ļ®öĒāĆļČäņäØ Ļ▓░Ļ│╝, ļīĆņĪ░ĻĄ░ņŚÉ ļ╣äĒĢśņŚ¼ H. pylori ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢ£ Ļ▓ĮņÜ░ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ņ”ØņāüņØ┤ ņ¦ĆņåŹļÉĀ ņāüļīĆņ£äĒŚśļÅä(relative risk, RR)Ļ░Ć 10% (95% ņŗĀļó░ĻĄ¼Ļ░ä [confidence interval, CI] 6.0-14.0%) Ļ░ÉņåīĒĢśņśĆņ£╝ļéś ĒÜ©Ļ│╝ ļ░£Ēśä ĒĢäņÜö ņ”ØļĪĆ ņłś(number needed to treat, NNT)ļŖö 14ļ¬ģ(95% CI = 10-25)ņ£╝ļĪ£ ĻĘĖ ĒÜ©Ļ│╝ņØś ņ░©ņØ┤Ļ░Ć Ēü¼ņ¦Ć ņĢŖņĢśļŗż[30]. ņśüĻĄŁņŚÉņä£ ņ¦äĒ¢ēĒĢ£ the Bristol Helicobacter ProjectņŚÉņä£ļŖö 60ņäĖ ņØ┤ĒĢśņØś ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×É 1,517ļ¬ģņØä H. pylori ņĀ£ĻĘĀ ņ╣śļŻīļ░øņØĆ ĻĄ░Ļ│╝ ņ£äņĢĮĻĄ░ņ£╝ļĪ£ ļéśļłäņ¢┤ ņČöņĀü Ļ┤Ćņ░░ĒĢśņśĆļŖöļŹ░, ņĀ£ĻĘĀ ņ╣śļŻī ņä▒Ļ│ĄĻĄ░ņØś 90%ņŚÉņä£ ņ”Øņāü Ļ░£ņäĀņŚÉ ĒÜ©Ļ│╝ļź╝ ļ│┤ņśĆļŗż(p< 0.05) [31].
ņä£ĻĄ¼ņŚÉ ļ╣äĒĢśņŚ¼ ĒĢ£ĻĄŁņØĆ H. pylori ņ£Āļ│æļźĀņØ┤ ļåÆņ£╝ļéś 2005ļģä 59.6%ņŚÉņä£ 2015ļģä 51.0%ļĪ£ Ļ░Éņåī ņČöņäĖļĪ£ ņØ┤ļ¤¼ĒĢ£ ļ│ĆĒÖöļŖö 40ļīĆ ņØ┤ĒĢś ņĀŖņØĆ ņŚ░ļĀ╣ņĖĄņŚÉņä£ ļŹöņÜ▒ ļÜ£ļĀĘĒĢśļŗż[32,33]. ĒĢ£ĻĄŁņØä ĒżĒĢ©ĒĢ£ ņĢäņŗ£ņĢä ĻĄŁĻ░ĆņŚÉņä£ļŖö ņä£ņ¢æņŚÉ ļ╣äĒĢ┤ ņ£äņĢöņØ┤ ĒØöĒĢśĻ│Ā ļ░£ļ│æ ņŚ░ļĀ╣ņØ┤ ļé«ņĢä ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ ņןĻĖ░Ļ░ä ņé░ļČäļ╣äņ¢ĄņĀ£ņĀ£ļéś H. pylori ņĀ£ĻĘĀ ņ╣śļŻī ļō▒ Ļ▓ĮĒŚśņĀü ņĢĮļ¼╝ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØĆ ĻĖ░ņ¦łņĀü ņ¦łĒÖśņØś ņ¦äļŗ©ņØä ņ¦ĆņŚ░ņŗ£Ēé¼ Ļ░ĆļŖźņä▒ņØ┤ ņ׳ļŗż. ļö░ļØ╝ņä£ ĻĄŁļé┤ņŚÉņä£ļŖö Ļ▓ĮĻ│Ā ņ”ØņāüņØ┤ ņŚåļŖö 40ņäĖ ļ»Ėļ¦īņØś ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉļōżņŚÉĻ▓ī ļ╣äņ╣©ņŖĄņĀüņØĖ ļ░®ļ▓ĢņØä ĒåĄĒĢ£ "H.pylori Ļ▓Ćņé¼ Ēøä ņ╣śļŻīŌĆØ ņŗ£Ē¢ēņØĆ Ļ│ĀļĀżĒĢĀ ņłś ņ׳ņ£╝ļéś 40ņäĖ ņØ┤ņāüņØ┤Ļ▒░ļéś Ļ▓ĮĻ│Ā ņ”ØņāüņØ┤ ņ׳ļŖö ĒÖśņ×ÉņŚÉĻ▓īļŖö ņÜ░ņäĀņĀüņ£╝ļĪ£ ņ£äļé┤ņŗ£Ļ▓ĮņØä ņŗżņŗ£ĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢśņśĆļŗż.
H. pylori Ļ░ÉņŚ╝ ņ¦äļŗ©ņŚÉ ņé¼ņÜ®ļÉśļŖö ļ╣äņ╣©ņŖĄņä▒ Ļ▓Ćņé¼ļŖö ņÜöņåīĒśĖĻĖ░ Ļ▓Ćņé¼, ļīĆļ│ĆĒĢŁņøÉ Ļ▓Ćņé¼, Ēśłņ▓Ł Ļ▓Ćņé¼Ļ░Ć ņ׳ļŗż. ņÜöņåīĒśĖĻĖ░ Ļ▓Ćņé¼ņÖĆ ļīĆļ│ĆĒĢŁņøÉ Ļ▓Ćņé¼ļŖö 90% ņØ┤ņāüņØś ļåÆņØĆ ļ»╝Ļ░ÉļÅäņÖĆ ĒŖ╣ņØ┤ļÅäļź╝ ļ│┤ņØ┤Ļ│Ā, ĒŖ╣Ē׳ ņÜöņåīĒśĖĻĖ░ Ļ▓Ćņé¼ļŖö ņŗ£Ē¢ēņØ┤ ņÜ®ņØ┤ĒĢśņŚ¼ H. pylori ņĀ£ĻĘĀ ņ╣śļŻī ņä▒Ļ│ĄņØä ĒÖĢņØĖĒĢśļŖö ļŹ░ ņ×äņāüņĀüņ£╝ļĪ£ Ļ░Ćņן ĒØöĒĢśĻ▓ī ņé¼ņÜ®ļÉ£ļŗż. Ēśłņ▓Ł Ļ▓Ćņé¼ļŖö H. pyloriņŚÉ ļīĆĒĢ£ ĒĢŁņ▓┤ļź╝ ņĖĪņĀĢĒĢśļŖö ļ░®ļ▓Ģņ£╝ļĪ£ ņĀĆļĀ┤ĒĢśĻ│Ā ņē¼ņÜ┤ ļ░®ļ▓ĢņØ┤ņ¦Ćļ¦ī, ĒĢŁņ▓┤ ņŚŁĻ░ĆĻ░Ć ļĢīļĪ£ļŖö ļ¬ć ļģä ļÅÖņĢł ņ¦ĆņåŹļÉśļŖö Ļ▓ĮņÜ░Ļ░Ć ņ׳ĻĖ░ ļĢīļ¼ĖņŚÉ ņĀ£ĻĘĀ ņ╣śļŻīņØś ņä▒Ļ│Ą ņŚ¼ļČĆļź╝ ļ░öļĪ£ ĒīÉņĀĢĒĢśĻĖ░ņŚÉļŖö ļČĆņĀüņĀłĒĢśņŚ¼ ņŻ╝ļĪ£ ņäĀļ│ä Ļ▓Ćņé¼ņÖĆ ņŚŁĒĢÖ ņŚ░ĻĄ¼ņŚÉ ņØ┤ņÜ®ļÉ£ļŗż. ņ╣©ņŖĄņĀü Ļ▓Ćņé¼ļĪ£ļŖö ņ£äļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ēĒĢĀ ļĢī, ņ£äņĀÉļ¦ē ņĪ░ņ¦üņāØĻ▓ĆņØä ņ¦äĒ¢ēĒĢśņŚ¼ ņŗĀņåŹņÜöņåīļČäĒĢ┤ĒÜ©ņåī Ļ▓Ćņé¼(rapid urease test)ņÖĆ ņĪ░ņ¦ü Ļ▓Ćņé¼ļź╝ ņ¦äĒ¢ēĒĢĀ ņłś ņ׳ļŗż. ņŗĀņåŹņÜöņåīļČäĒĢ┤ĒÜ©ņåī Ļ▓Ćņé¼ļŖö H. pyloriĻ░Ć ļČäļ╣äĒĢśļŖö ņÜöņåīļČäĒĢ┤ĒÜ©ņåīņŚÉ ņØśĒĢśņŚ¼ ņāØņä▒ļÉ£ ņĢöļ¬©ļŗłņĢäĻ░Ć ņÜöņåīļ░░ņ¦ĆņØś pHļź╝ ņāüņŖ╣ņŗ£ĒéżļŖö Ļ▓āņØä ņāē ļ│ĆĒÖöļĪ£ ĒÖĢņØĖĒĢśļŖö Ļ▓Ćņé¼ņØ┤ļŗż. ņĪ░ņ¦ü Ļ▓Ćņé¼ļŖö H. pylori ņ¦äļŗ© ņÖĖņŚÉļÅä ņĀÉļ¦ēņØś ņŚ╝ņ”Ø, ņ£äņČĢ ĻĘĖļ”¼Ļ│Ā ņןņāüĒö╝ĒÖöņāØ ļō▒ņØś ņČöĻ░Ć ņĀĢļ│┤ļź╝ ņ¢╗ņØä ņłś ņ׳ļŖö ņןņĀÉņØ┤ ņ׳ļŗż.
Ļ▓ĮĻ│Ā ņ”Øņāü
3. ļ¦īņä▒ ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉĻ░Ć 40ņäĖ ņØ┤ņāüņØ┤Ļ▒░ļéś ņé╝Ēé┤Ļ│żļ×Ć, ņ¦ĆņåŹņĀü ĻĄ¼ĒåĀ, ļ╣äņĀĢņāüņĀü ņ▓┤ņżæĻ░Éņåī, ņČ£Ēśł ņ¦ĢĒøä, ņ£äņĢö Ļ░ĆņĪ▒ļĀźņØ┤ ņ׳Ļ▒░ļéś ņĄ£ĻĘ╝ ņ¦äĒåĄņåīņŚ╝ņĀ£ /ĒĢŁĒśłņĀäņĀ£ļź╝ ļ│ĄņÜ®ĒĢ£ Ļ▓ĮņÜ░ ĻĖ░ņ¦łņĀü ņ¦łĒÖśņØä Ļ░Éļ│äĒĢśĻĖ░ ņ£äĒĢśņŚ¼ ņČöĻ░Ć Ļ▓Ćņé¼ļź╝ ĻČīĻ│ĀĒĢ£ļŗż.
ŌĆó ĻČīĻ│Ā ļō▒ĻĖē: Ļ░ĢĒĢ©
ŌĆó ņ”ØĻ▒░ ņłśņżĆ: ļé«ņØī
ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØĆ ņĀäĒśĢņĀü ņ”ØņāüĻ│╝ ĒĢ©Ļ╗ś ņ£äņĢö, ņ£äĻČżņ¢æ ļō▒ ĻĖ░ņ¦łņĀü ņ¦łĒÖśņØä ļ░░ņĀ£ĒĢ£ Ēøä ņ¦äļŗ©ĒĢ£ļŗż. ņŚ¼ļ¤¼ ĻČīĻ│ĀņĢłņŚÉņä£ ņ£äĒŚś ņ¦ĢĒøäĻ░Ć ņ׳ļŖö Ļ▓ĮņÜ░(ņé╝Ēé┤Ļ│żļ×Ć, ņ¦ĆņåŹņĀü ĻĄ¼ĒåĀ, ļ╣äņĀĢņāüņĀü ņ▓┤ņżæĻ░Éņåī, ņČ£Ēśł ņ¦ĢĒøä ļ░Å ņ£äņĢö Ļ░ĆņĪ▒ļĀźņØ┤ ņ׳Ļ▒░ļéś ņĄ£ĻĘ╝ ņ¦äĒåĄņåīņŚ╝ņĀ£ ļśÉļŖö ĒĢŁĒśłņĀäņĀ£ļź╝ ļ│ĄņÜ®ĒĢ£ Ļ▓ĮņÜ░, ĻĖ░ņ¦łņĀü ņ¦łĒÖśņØä Ļ░Éļ│äĒĢśĻĖ░ ņ£äĒĢśņŚ¼ Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢ£ļŗż[14,16,34,35]. ĻĘĖļ¤¼ļéś ņ▓┤Ļ│äņĀü ļ¼ĖĒŚīĻ│Āņ░░ņŚÉ ļö░ļź┤ļ®┤ ņ£äĒŚś ņ”ØņāüņØ┤ļéś ņ¦ĢĒøäĻ░Ć ĻĖ░ņ¦łņĀü ņøÉņØĖņØä Ļ░Éļ│äĒĢśļŖö ļŹ░ ņĀ£ĒĢ£ņĀüņØ┤ņŚłļŗż[36]. 2017ļģä ļ░£Ēæ£ĒĢ£ ļ»ĖĻĄŁĻ│╝ ņ║Éļéśļŗż ņ¦äļŻī ņ¦Ćņ╣©ņŚÉņä£ļŖö 60ņäĖ ņØ┤ĒĢśņØś ĒÖśņ×ÉļōżņŚÉĻ▓ī ņ£äĒŚś ņ¦ĢĒøäĻ░Ć ņ׳ņ¢┤ļÅä ņāüļČĆņ£äņןĻ┤Ć ņŗĀņāØļ¼╝ņØä Ļ░Éļ│äĒĢśĻĖ░ ņ£äĒĢ£ ļé┤ņŗ£Ļ▓ĮņØä ĻČīĻ│ĀĒĢśņ¦Ć ņĢŖņĢśĻ│Ā, ņĘīņןļŗ┤ļÅä ņ¦łĒÖśņØ┤ ņØśņŗ¼ļÉśļŖö Ļ▓ĮņÜ░ņŚÉ ņśüņāüĒĢÖņĀü Ļ▓Ćņé¼ļź╝ ĻČīĻ│ĀĒĢśņśĆļŗż[17]. ĻĘĖļ¤¼ļéś ĒĢ£ĻĄŁņØĆ ņ£äņĢö ņ£Āļ│æļźĀņØ┤ ļåÆĻ│Ā[37], ņĢäņŗ£ņĢäņØĖņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ ņ▓┤Ļ│äņĀü ļ¼ĖĒŚīĻ│Āņ░░ņŚÉņä£ ņ£äĒŚś ņ¦ĢĒøäĻ░Ć ņĀŖņØĆ ņĢäņŗ£ņĢäņØĖņŚÉņä£ ĻĖ░ņ¦łņĀü ņ¦łĒÖśņØä Ļ░Éļ│äĒĢśļŖö ļŹ░ ņ£ĀņÜ®ĒĢśļŗżļŖö Ļ▓░Ļ│╝ļź╝ ņĀ£ņŗ£ĒĢśņŚ¼[38], ņØ┤ļ▓ł ņ¦Ćņ╣©ņŚÉņä£ļŖö ņ£äĒŚś ņ¦ĢĒøäĻ░Ć ņ׳ļŖö ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉņŚÉņä£ļŖö ļéśņØ┤ņÖĆ ļ¼┤Ļ┤ĆĒĢśĻ▓ī ņāüļČĆņ£äņןĻ┤Ć ļé┤ņŗ£Ļ▓Į ļō▒ņØä ņŗ£Ē¢ēĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢśņśĆļŗż.
ņåīĒÖöļČłļ¤ēņØś Ļ▓ĮĒŚśņĀü ņ╣śļŻīņŚÉ ļ░śņØæņØ┤ ņŚåļŖö ĒÖśņ×ÉļŖö ņ▓½ ņ¦äļŗ© ļŗ╣ņŗ£ ĒśłņĢĪ Ļ▓Ćņé¼ļź╝ ņŗżņŗ£ĒĢśņ¦Ć ņĢŖņĢśļŗżļ®┤ ņØ╝ļ░śĒśłņĢĪ Ļ▓Ćņé¼, ĒśłņĢĪĒÖöĒĢÖ Ļ▓Ćņé¼ņÖĆ Ļ░ÖņØĆ ĒśłņĢĪ Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØä ĻČīĻ│ĀĒĢ£ļŗż. ĒŖ╣Ē׳ Ļ░äņĢö ļśÉļŖö ņĘīņןņĢöņØś ņ£Āļ│æļźĀņØ┤ ļåÆņØĆ ņ¦ĆņŚŁņŚÉņä£ļŖö ņØ┤ļōż ņ¦łĒÖśņØ┤ ņåīĒÖöļČłļ¤ē ņ”ØņāüņØä ļÅÖļ░śĒĢĀ ņłś ņ׳ņ£╝ļ»ĆļĪ£, ņāüļ│ĄļČĆ ņ┤łņØīĒīī ļśÉļŖö ļ│ĄļČĆ CTļź╝ Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢ£ļŗż[14,17,39,40].
ņ╣śļŻī
ņ£äņé░ļČäļ╣äņ¢ĄņĀ£ņĀ£
ĒöäļĪ£ĒåżĒÄīĒöäņ¢ĄņĀ£ņĀ£(proton pump inhibitor, PPI)
4. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ ĒöäļĪ£ĒåżĒÄīĒöäņ¢ĄņĀ£ņĀ£ļŖö ņ”Øņāü ĒśĖņĀäņŚÉ ĒÜ©Ļ│╝ņĀüņØ┤ņ¢┤ņä£ 1ņ░© ņ╣śļŻīļĪ£ ĻČīĻ│ĀĒĢ£ļŗż.
ŌĆó ĻČīĻ│Ā ļō▒ĻĖē: Ļ░ĢĒĢ©
ŌĆó ņ”ØĻ▒░ ņłśņżĆ: ļåÆņØī
ŌĆó ņĀäļ¼ĖĻ░Ć ņØśĻ▓¼: ņĀäņĀüņ£╝ļĪ£ ļÅÖņØśĒĢ©(44.5%), ļīĆņ▓┤ļĪ£ ļÅÖņØśĒĢ©(37.0%), ņØ╝ļČĆ ļÅÖņØśĒĢ©(14.8%), ļīĆņ▓┤ļĪ£ ļÅÖņØśĒĢśņ¦Ć ņĢŖņØī(3.7%), ņĀäņĀüņ£╝ļĪ£ ļÅÖņØśĒĢśņ¦Ć ņĢŖņØī(0%), ļ¬©ļź┤Ļ▓ĀņØī(0%)
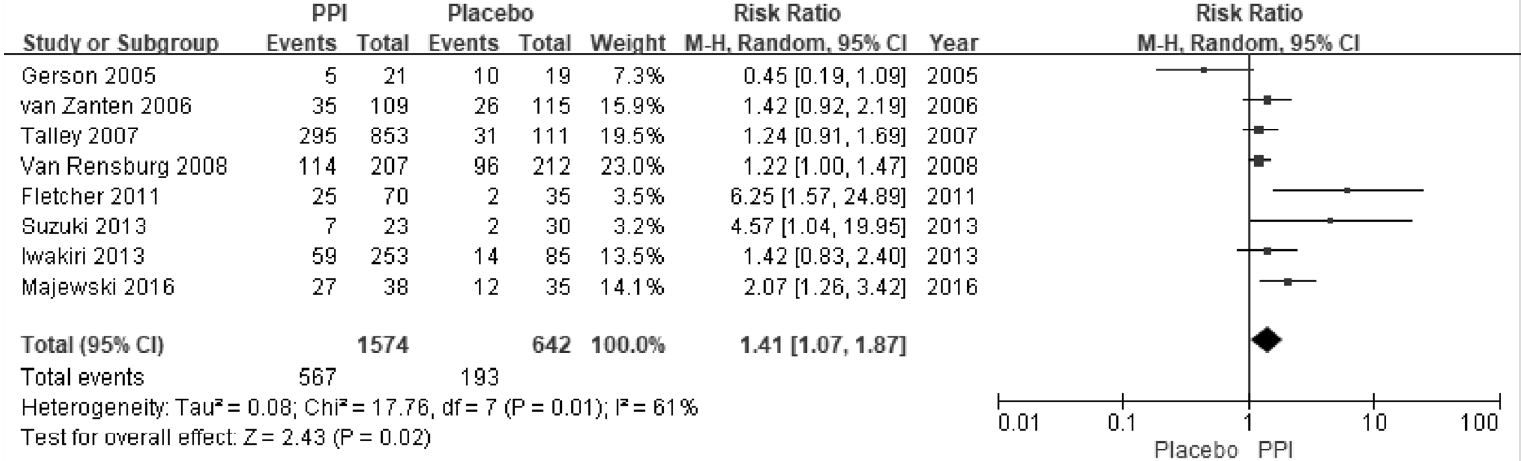
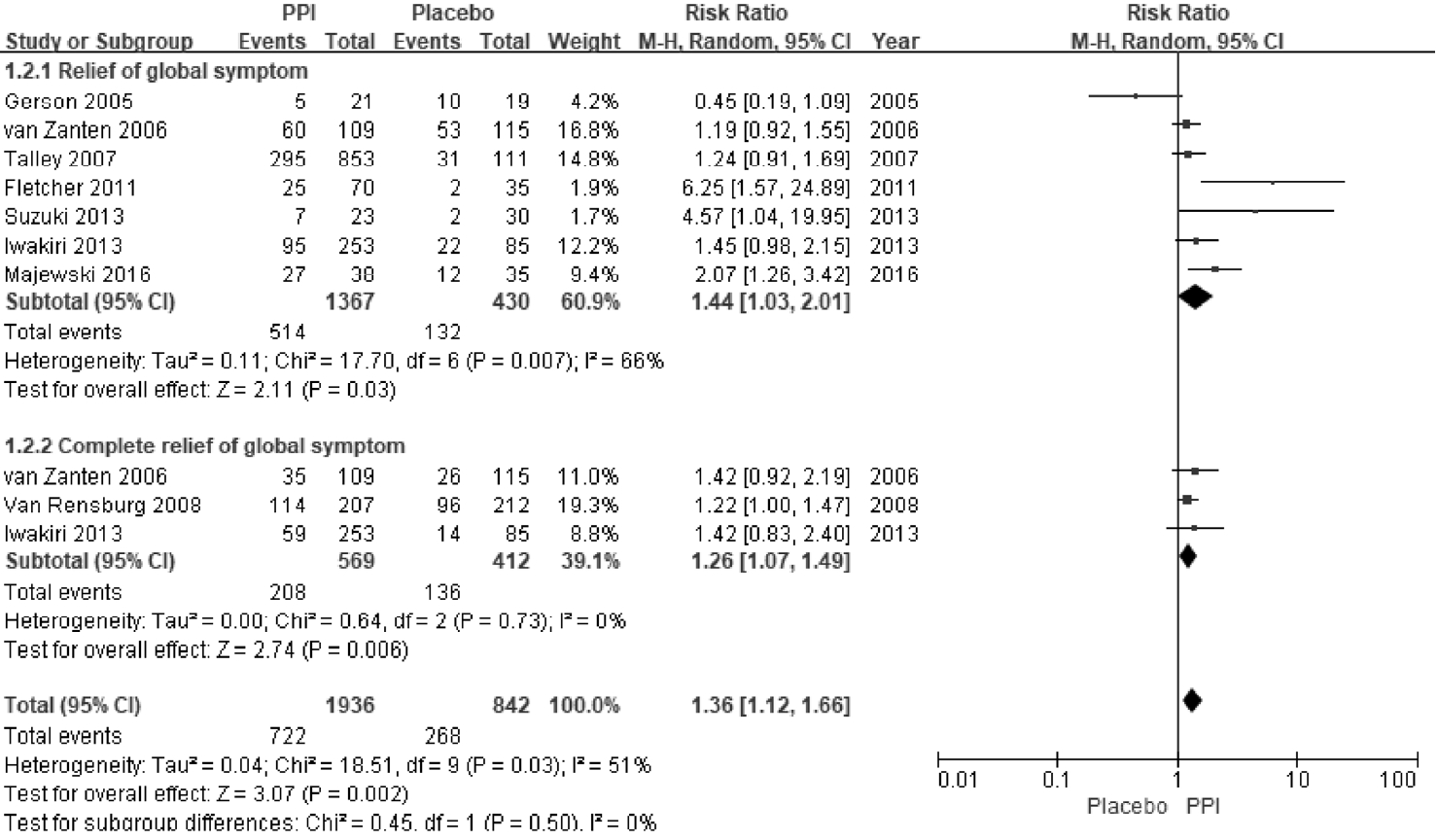
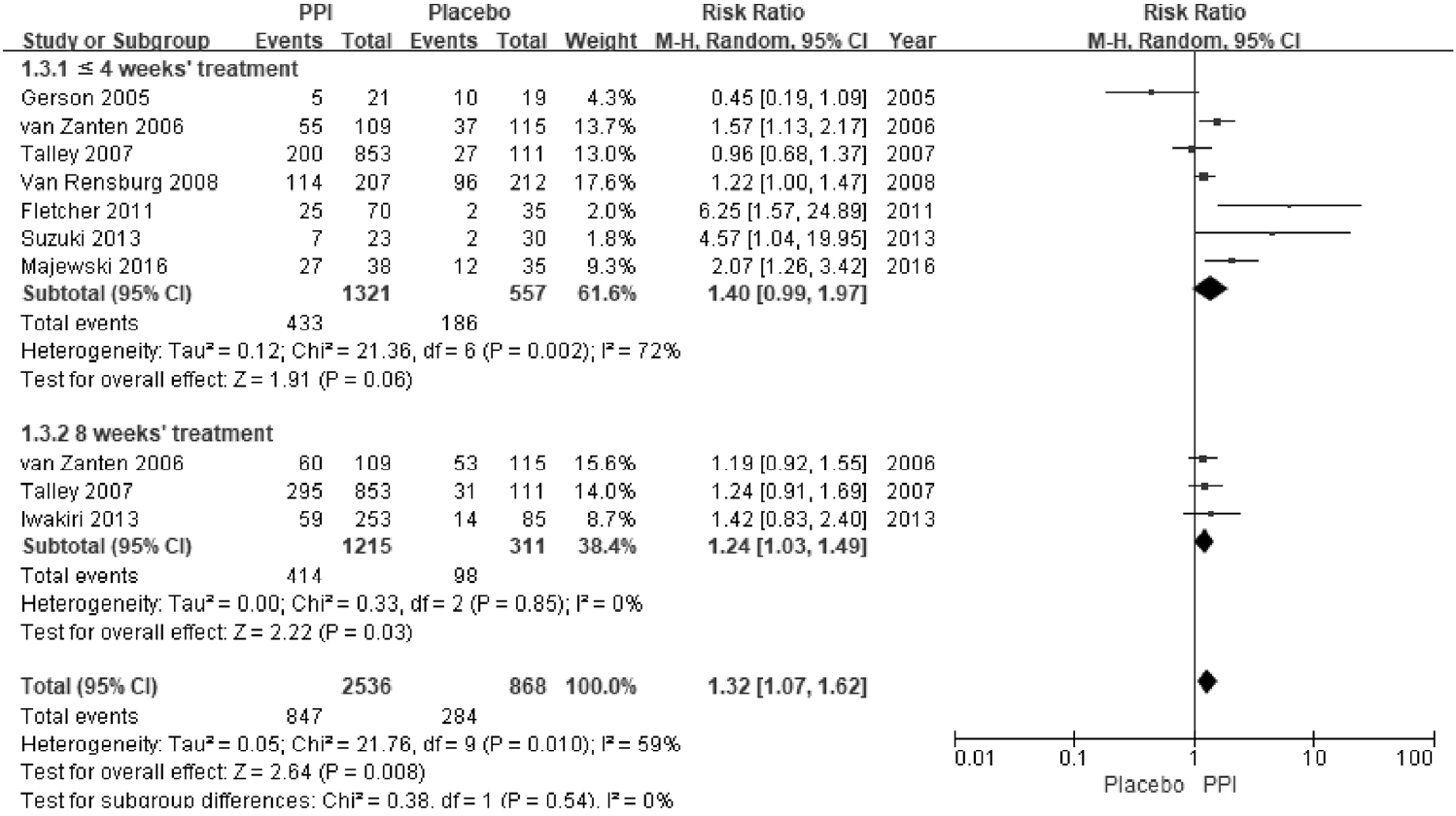
ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØĆ ņŗŁņØ┤ņ¦Ćņןļé┤ ņé░ ņ▓ŁņåīļŖź Ļ░ÉņåīļĪ£ ņØĖĒĢśņŚ¼ ņé░ļģĖņČ£ņØ┤ ņ”ØĻ░ĆĒĢśĻ│Ā ļé┤ņןĻ│╝ļ»╝ņä▒ņØ┤ ņ”ØĻ░ĆĒĢśļ®░ ņ£ä ņÜ┤ļÅÖņןņĢĀĻ░Ć ņ┤łļלļÉĀ ņłś ņ׳ļŗż. ļö░ļØ╝ņä£ ņ£äņé░ļČäļ╣äņ¢ĄņĀ£ņĀ£ļŖö ņŗŁņØ┤ņ¦Ćņןļé┤ņØś ņé░ļÅäļź╝ ņĀĢņāüĒÖöņŗ£ņ╝£ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ņ╣śļŻīņŚÉ ļÅäņøĆņØä ņŻ╝ļŖö Ļ▓āņ£╝ļĪ£ ņāØĻ░üĒĢ£ļŗż[41-43]. ņØ┤ļ¤¼ĒĢ£ ņĀÉņŚÉņä£ PPIļŖö ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ņżæņÜöĒĢ£ ņ╣śļŻīņĀ£ļĪ£ ņé¼ņÜ®ļÉśņ¢┤ ņÖöļŗż[44]. ņØ┤ļ▓ł ņ¦Ćņ╣©ņŚÉņä£ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ PPIņØś ņĀäļ░śņĀüņØĖ ņ”Øņāü ĒśĖņĀäņ£©ņØä ļ╣äĻĄÉĒĢ£ 8Ļ░£ RCT (n=2,216)ļź╝ ļīĆņāüņ£╝ļĪ£ ļ®öĒāĆļČäņäØņØä ņŗ£Ē¢ēĒĢśņśĆļŗż[45-52]. PPIļź╝ 2-8ņŻ╝Ļ░ä Ēł¼ņŚ¼ļ░øņØĆ ņ╣śļŻīĻĄ░ņŚÉņä£ ņ£äņĢĮĻĄ░ņŚÉ ļ╣äĒĢśņŚ¼ ņ£ĀņØśĒĢśĻ▓ī ņ”Øņāü ĒśĖņĀäņ£©ņØ┤ ļåÆņĢśļŗż(36% vs. 30%, RR = 1.41, 95% CI = 1.07-1.87). ĻĘĖļ¤¼ļéś ņŚ░ĻĄ¼ņØś ņØ┤ņ¦łņä▒ņØ┤ ļåÆņĢśĻ│Ā(Žć2 = 17.76, p= 0.01, I2 = 61%) (Fig. 1), NNTļŖö 9 ļ¬ģņØ┤ņŚłļŗż(95% CI = 6-24). ĒĢśņ£ä ļČäņäØņŚÉņä£ PPIņØś ņ”Øņāü ņÖäĒÖöņŚÉ ļīĆĒĢ£ RRņØĆ 1.44ņśĆĻ│Ā, ņÖäņĀäĒĢ£ ņ”Øņāü ĒśĖņĀäņŚÉ ļīĆĒĢ£ RRņØĆ 1.26ņØ┤ņŚłļŗż(Fig. 2). ņ╣śļŻī ĻĖ░Ļ░äņŚÉ ļö░ļźĖ ļČäņäØņŚÉņä£ 8ņŻ╝ ļÅÖņĢł PPIļź╝ Ēł¼ņŚ¼ĒĢśņśĆņØä ļĢī ņ”Øņāü ĒśĖņĀäņØ┤ ļÜ£ļĀĘĒĢ£ ļ░śļ®┤(RR = 1.24, 95% CI = 1.03-1.49), (Žć2 = 0.33, p= 0.85, I2 = 0%) 4ņŻ╝ ļ»Ėļ¦īņ£╝ļĪ£ Ēł¼ņŚ¼ĒĢśņśĆņØä ļĢīļŖö ņ£äņĢĮĻĄ░Ļ│╝ ņ”Øņāü ĒśĖņĀäņŚÉ ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż(RR = 1.40, 95% CI = 0.99-1.97) (Fig. 3). ļö░ļØ╝ņä£ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ ņןĻĖ░ņĀüņØĖ ņ”ØņāüņØś ĒśĖņĀäņØä ņ£äĒĢ┤ņä£ 8ņŻ╝ ņØ┤ņāü PPI ņ╣śļŻīļź╝ ĻČīĻ│ĀĒĢ£ļŗż.
5. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ņĢäĒśĢ ņżæ ļ¬ģņ╣śĒåĄņ”Øņ”ØĒøäĻĄ░ ĒÖśņ×ÉņŚÉņä£ ĒöäļĪ£ĒåżĒÄīĒöäņ¢ĄņĀ£ņĀ£ļź╝ 1ņ░© ņ╣śļŻī ņĢĮņĀ£ļĪ£ ņÜ░ņäĀņĀüņ£╝ļĪ£ ĻČīĻ│ĀĒĢ£ļŗż.
ŌĆó ĻČīĻ│Ā ļō▒ĻĖē: Ļ░ĢĒĢ©
ŌĆó ņ”ØĻ▒░ ņłśņżĆ: ņżæļō▒ļÅä
ŌĆó ņĀäļ¼ĖĻ░Ć ņØśĻ▓¼: ņĀäņĀüņ£╝ļĪ£ ļÅÖņØśĒĢ©(25.9%), ļīĆņ▓┤ļĪ£ ļÅÖņØśĒĢ©(55.6%), ņØ╝ļČĆ ļÅÖņØśĒĢ©(18.5%), ļīĆņ▓┤ļĪ£ ļÅÖņØśĒĢśņ¦Ć ņĢŖņØī(0%), ņĀäņĀüņ£╝ļĪ£ ļÅÖņØśĒĢśņ¦Ć ņĢŖņØī(0%), ļ¬©ļź┤Ļ▓ĀņØī(0%)
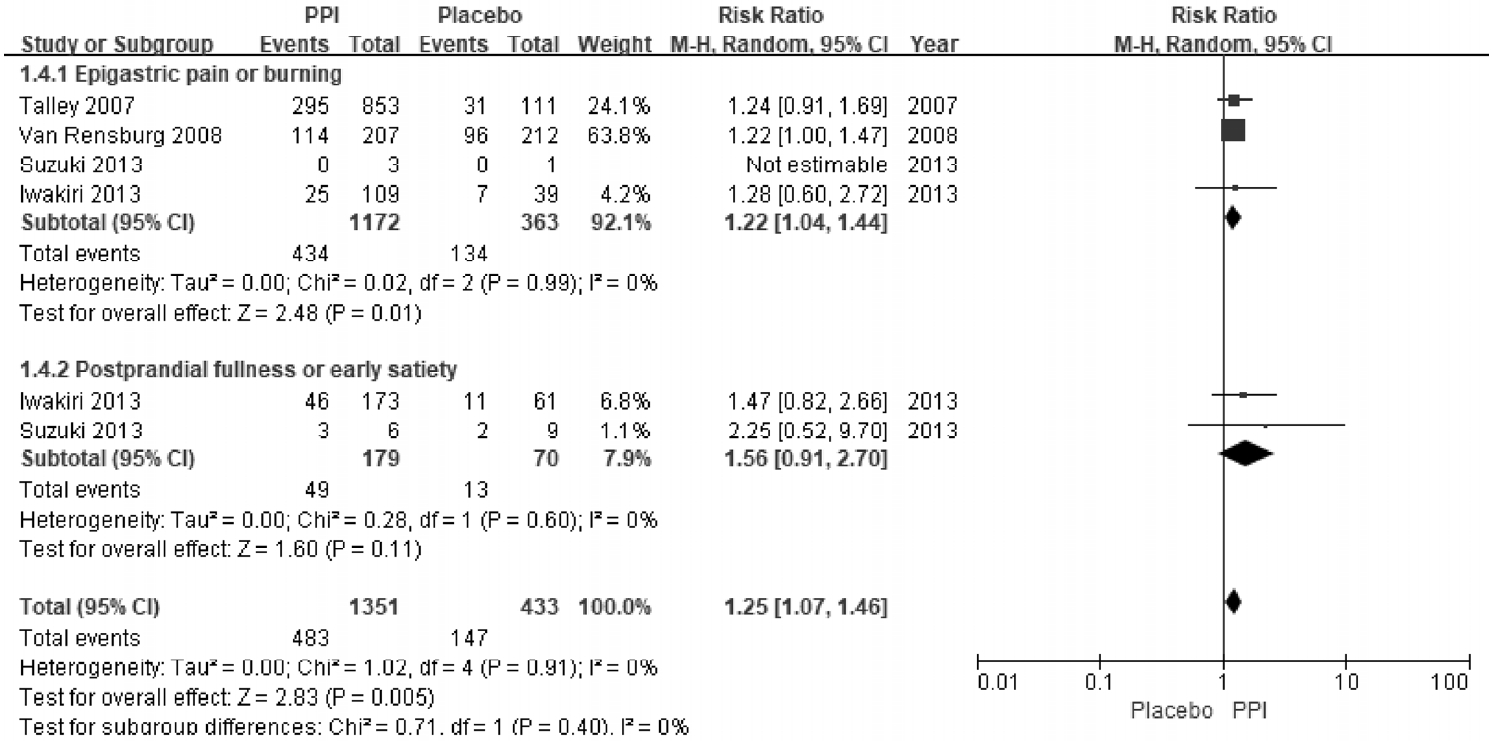
PPIļŖö ļĪ£ļ¦łĻĖ░ņżĆ IIņŚÉ ļö░ļØ╝ ņāüļ│ĄļČĆ ĒåĄņ”ØņØä ņŻ╝ļĪ£ ĒśĖņåīĒĢśļŖö ĻČżņ¢æĒśĢĻ│╝ ņŚŁļźś ņ”ØņāüņØ┤ ņŻ╝ļĪ£ ļéśĒāĆļéśļŖö ņŚŁļźśĒśĢņØś ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņŚÉņä£ ĒÜ©Ļ│╝Ļ░Ć ņ׳ļŗżĻ│Ā ņĢīļĀżņĀĖ ņÖöĻ│Ā[53], ņØ┤ņĀä ņ¦äļŻī ņ¦Ćņ╣©ņŚÉņä£ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ņĢäĒśĢņŚÉ ļö░ļØ╝ PPI ņé¼ņÜ®ņØä ĻČīĻ│ĀĒĢśņśĆņ£╝ļéś[14,54,55], ĒÜ©Ļ│╝ņÖĆ Ļ┤ĆļĀ©ĒĢ┤ņä£ ļģ╝ņ¤üņØś ņŚ¼ņ¦ĆĻ░Ć ņ׳ļŗż[56-58]. ļĪ£ļ¦łĻĖ░ņżĆ III ņŚÉņä£ļŖö ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØä EPSņÖĆ PDSļĪ£ ļéśļłäĻ│Ā ņ׳ņ¦Ćļ¦ī, Ļ░ÖņØĆ ĒÖśņ×ÉņŚÉņä£ EPSņÖĆ PDSĻ░Ć ļÅÖņŗ£ņŚÉ ņżæļ│ĄĒĢ┤ņä£ ļéśĒāĆļéśļŖö Ļ▓ĮņÜ░Ļ░Ć ĒØöĒĢśļŗż[28,59]. ņØ┤ļ▓ł ņ¦Ćņ╣©ņŚÉņä£ ņŻ╝ņ”Øņāüņ£╝ļĪ£ ņāüļ│ĄļČĆ ĒåĄņ”ØĻ│╝ ņāüļ│ĄļČĆ ņō░ļ”╝ņØä ĒśĖņåīĒĢśļŖö EPSņĢäĒśĢ ĒÖśņ×ÉļōżņŚÉ ļīĆĒĢśņŚ¼ PPIņØś ĒÜ©Ļ│╝ļź╝ ļČäņäØĒĢ£ 4Ļ░£ RCTļź╝ ļīĆņāüņ£╝ļĪ£ ļ®öĒāĆļČäņäØņØä ņŗ£Ē¢ēĒĢśņśĆļŗż[47,48,50,51]. ĻĘĖ Ļ▓░Ļ│╝, PPIļŖö ņāüļ│ĄļČĆ ĒåĄņ”ØĻ│╝ ņāüļ│ĄļČĆ ņō░ļ”╝ ņ╣śļŻīņŚÉ ņ£äņĢĮĻĄ░ļ│┤ļŗż ĒÜ©Ļ│╝ņĀüņØ┤ļéś(RR = 1.22, 95% CI = 1.04-1.44, Žć2 = 0.02, p= 0.99, I2 =0%) ņŗØĒøä Ēżļ¦īĻ░ÉņØ┤ļéś ņĪ░ĻĖ░ ļ¦īļ│ĄĻ░ÉņØä ĒśĖņåīĒĢśļŖö PDSļź╝ ļīĆņāüņ£╝ļĪ£ ĒĢśļŖö 2Ļ░£ņØś RCTņŚÉ ļīĆĒĢ£ ļ®öĒāĆļČäņäØņŚÉņä£ PPI ņ╣śļŻīĻ░Ć ņ£äņĢĮĻĄ░ņŚÉ ļ╣äĒĢśņŚ¼ ĒÜ©Ļ│╝ņĀüņØ┤ņ¦Ć ņĢŖņĢśļŗż(RR = 1.56, 95% CI = 0.91-2.70) (Fig. 4) [50,51]. ĻĘĖļ¤¼ļéś ņØ┤ ļ®öĒāĆļČäņäØņŚÉ ĒżĒĢ©ļÉ£ RCT ņŚ░ĻĄ¼ļ¦łļŗż ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ņĀĢņØśĻ░Ć ļŗ¼ļØ╝ ĻČīĻ│ĀņĢłņØś ĻĘ╝Ļ▒░ ņłśņżĆņØä ņżæļō▒ļÅäļĪ£ ļé«ņČöņŚłļŗż.
Ē׳ņŖżĒāĆļ»╝ ņłśņÜ®ņ▓┤ ĻĖĖĒĢŁņĀ£(histamine-2 receptor antagonists, H2RA)
6. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ Ē׳ņŖżĒāĆļ»╝ ņłśņÜ®ņ▓┤ ĻĖĖĒĢŁņĀ£ļŖö ņ”Øņāü ĒśĖņĀäņŚÉ ĒÜ©Ļ│╝ņĀüņØ┤ļ»ĆļĪ£ ĻČīĻ│ĀĒĢ£ļŗż. ļŗ©, Ē׳ņŖżĒāĆļ»╝ ņłśņÜ®ņ▓┤ ĻĖĖĒĢŁņĀ£ļŖö ņןĻĖ░ ņé¼ņÜ®ņ£╝ļĪ£ ņĢĮĒÜ©Ļ░Ć Ļ░ÉņåīļÉĀ ņłś ņ׳ņ¢┤ ļŗ©ĻĖ░Ļ░ä ņé¼ņÜ®ņØä Ļ│ĀļĀżĒĢ£ļŗż.
ŌĆó ĻČīĻ│Ā ļō▒ĻĖē: ņĢĮĒĢ©
ŌĆó ņ”ØĻ▒░ ņłśņżĆ: ņżæļō▒ļÅä
ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ņ╣śļŻīņŚÉ ņ£äņé░ļČäļ╣äņ¢ĄņĀ£ņĀ£ļĪ£ H2RAĻ░Ć ņé¼ņÜ®ļÉĀ ņłś ņ׳ļŗż. 2,456ļ¬ģņØś ļ╣äĻČżņ¢æņä▒ ņåīĒÖöļČłļ¤ē ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ĒĢ£ 12ĒÄĖņØś ņĮöĒü¼ļ×Ć ļ®öĒāĆļČäņäØņŚÉ ļö░ļź┤ļ®┤, H2RAļź╝ ņé¼ņÜ®ĒĢśņśĆņØä ļĢī ņ”ØņāüņØ┤ ļé©ņĢä ņ׳ņØä RRņØĆ 0.77 (95% CI=0.65-0.92)ņØ┤ņŚłņ£╝ļ®░, NNTļŖö 7ļ¬ģņØ┤ņŚłļŗż. ĻĘĖļ¤¼ļéś ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ņ╣śļŻīņŚÉ H2RAņØś ĻĘ╝Ļ▒░ļŖö ņČ®ļČäĒĢśņ¦Ć ņĢŖļŗż. ņØ┤ ļČäņäØņŚÉ ĒżĒĢ©ļÉ£ ņ×äņāüņŗ£ĒŚśņØś ņĀäļ░śņĀü ņ¦łņØĆ ļīĆņ▓┤ļĪ£ ļé«ņĢśņ£╝ļ®░, ļĪ£ļ¦łĻĖ░ņżĆIIIņØ┤ ļ¦łļĀ©ļÉśĻĖ░ ņĀäņŚÉ ņŗ£Ē¢ēļÉ£ ņŚ░ĻĄ¼ļōżļĪ£ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ĻĖ░ņżĆņĪ░ņ░© ļČäļ¬ģĒĢśņ¦Ć ņĢŖņĢśļŗż[60]. 2,456ļ¬ģņØś ņåīĒÖöļČłļ¤ē ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ 7Ļ░£ RCTļź╝ ļČäņäØĒĢ£ ņĄ£ĻĘ╝ņØś ļ®öĒāĆļČäņäØ ņŚ░ĻĄ¼ņŚÉņä£ PPIĒł¼ņŚ¼ĻĄ░Ļ│╝ H2RA Ēł¼ņŚ¼ĻĄ░ ņé¼ņØ┤ņŚÉ ņ”Øņāü ĒśĖņĀäņØś ņ£ĀņØśĒĢ£ ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśņ£╝ļéś(RR = 0.93, 95% CI = 0.76-1.16), PPIĻĄ░ņŚÉņä£ ļŹö ļåÆņØĆ ņ”Øņāü ĒśĖņĀäņØś Ļ▓ĮĒ¢źņØä ļ│┤ņśĆļŗż[17]. ļśÉĒĢ£ H2RAļŖö ņé¼ņÜ®ĒĢĀņłśļĪØ ņ▓śņØīļ│┤ļŗż ĒÜ©Ļ│╝Ļ░Ć Ļ░ÉņåīĒĢśļŖö ņåŹņä▒ļé┤ņä▒(tachyphylaxis)ņØ┤ ļ░£ņāØĒĢĀ Ļ░ĆļŖźņä▒ņØ┤ ņ׳ņ¢┤[61,62], ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ņ£Āņ¦Ćņ╣śļŻīņĀ£ļĪ£ H2RAņØś ņé¼ņÜ®ņØĆ ņĀ£ĒĢ£ņĀüņØ┤ļŗż[63]. ļ┐Éļ¦ī ņĢäļŗłļØ╝ H2RAļŖö ļ╣äĻĄÉņĀü ņĢłņĀäĒĢ£ ņĢĮņĀ£ļĪ£ ņĢīļĀżņĀĖ ņ׳ņ£╝ļéś ņĢäļéÖĒĢäļØĮņŗ£ņŖżļź╝ ĒżĒĢ©ĒĢ£ ļČĆņ×æņÜ®ņØ┤ ļ░£ņāØĒĢĀ ņłś ņ׳ļŗż. ĻĄŁļé┤ ņŚ░ĻĄ¼ņŚÉņä£ ranitidineļĪ£ ņØĖĒĢ£ ņĢäļéÖĒĢäļØĮņŗ£ņŖżĻ░Ć ļ░£ņāØĒĢśņśĆļŗżļŖö ļ│┤Ļ│ĀĻ░Ć ņ׳ļŗż[64]. ļśÉĒĢ£ 2019ļģä 9ņøö ranitidineņŚÉņä£ ņåīļ¤ēņØś N-ļŗłĒŖĖļĪ£ņåīļ®öĒŗĖņĢäļ»╝ņØ┤ Ļ▓ĆņČ£ļÉśņ¢┤ ņŗ£ņןņŚÉņä£ Ēć┤ņČ£ļÉśņŚłļŗż.
ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£
7. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£ļŖö ņ”Øņāü ĒśĖņĀäņŚÉ ĒÜ©Ļ│╝ņĀüņØ┤ļ»ĆļĪ£ ĻČīĻ│ĀĒĢ£ļŗż.
ŌĆó ĻČīĻ│Ā ļō▒ĻĖē: Ļ░ĢĒĢ©
ŌĆó ņ”ØĻ▒░ ņłśņżĆ: ņżæļō▒ļÅä
ŌĆó ņĀäļ¼ĖĻ░Ć ņØśĻ▓¼: ņĀäņĀüņ£╝ļĪ£ ļÅÖņØśĒĢ©(35.7%), ļīĆņ▓┤ļĪ£ ļÅÖņØśĒĢ©(53.6%), ņØ╝ļČĆ ļÅÖņØśĒĢ©(10.7%), ļīĆņ▓┤ļĪ£ ļÅÖņØśĒĢśņ¦Ć ņĢŖņØī(0%), ņĀäņĀüņ£╝ļĪ£ ļÅÖņØśĒĢśņ¦Ć ņĢŖņØī(0%), ļ¬©ļź┤Ļ▓ĀņØī(0%)
ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£ļŖö ņ×æņÜ® ĻĖ░ņĀäņŚÉ ĻĖ░ņ┤łĒĢśņŚ¼ ļÅäĒīīļ»╝ D2 ņłśņÜ®ņ▓┤ ĻĖĖĒĢŁņĀ£, ņäĖļĪ£ĒåĀļŗī 4ĒśĢ(5-HT4) ņłśņÜ®ņ▓┤ ņ×æņÜ®ņĀ£, ļ¬©ĒŗĖļ”░ ņ×æņÜ®ņĀ£ļĪ£ ļČäļźśļÉ£ļŗż. ļÅäĒīīļ»╝ D2 ņłśņÜ®ņ▓┤ ĻĖĖĒĢŁņĀ£ņØĖ domperidoneņØĆ ļ®öĒāĆļČäņäØņŚÉņä£ 2-4ņŻ╝ ļÅÖņĢł ņé¼ņÜ®ĒĢ£ Ļ▓ĮņÜ░ ņ£äņĢĮĻ│╝ ļ╣äĻĄÉĒĢśņśĆņØä ļĢī ĒīĮļ¦īĻ░ÉĻ│╝ ņĪ░ĻĖ░ ļ¦īļ│ĄĻ░É ņ”ØņāüņØś Ļ░£ņäĀņŚÉ ĒÜ©Ļ│╝ņĀüņØĖ Ļ▓āņ£╝ļĪ£ ļ░ØĒśĆņĪīļŗż[65]. MetoclopramideņÖĆ levosulpirideļŖö ņåīĒÖöļČłļ¤ē ņ”ØņāüņØä Ļ░£ņäĀņŗ£ĒéżļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż[66]. ĻĘĖļ¤¼ļéś ĒÜ©Ļ│╝ņĀüņØĖ D2 ĻĖĖĒĢŁņĀ£ņØĖ metoclopramide, levosulpirideņÖĆ domperidoneņØĆ ņČöņ▓┤ņÖĖļĪ£(extrapyramidal) ņ”ØņāüņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ņ¢┤ ĒĢ£ĻĄŁņŚÉņä£ļŖö Ēł¼ņĢĮ ĻĖ░Ļ░äņØś ņĀ£ĒĢ£ņØ┤ ņ׳ļŗż.
ļ¦Éņ┤łņĀüņ£╝ļĪ£ ņ×æņÜ®ĒĢśļŖö D2 ņłśņÜ®ņ▓┤ ĻĖĖĒĢŁņĀ£ņØĖ itoprideļŖö ņżæņŗ¼ ņłśņÜ®ņ▓┤ņÖĆ ņŚ░Ļ┤ĆļÉ£ ņČöņ▓┤ņÖĖļĪ£ ļČĆņ×æņÜ®ņØä Ēö╝ĒĢĀ ņłś ņ׳Ļ│Ā, ĒöäļĪ£ļØĮĒŗ┤ ĒśĖļź┤ļ¬¼ ņāüņŖ╣ļÅä ņĢäņŻ╝ ņĀüĻ▓ī ļéśĒāĆļé£ļŗż. ņØ┤ļ¤¼ĒĢ£ itoprideļŖö 9Ļ░£ ņŚ░ĻĄ¼, 2,620ļ¬ģņØä ļČäņäØĒĢ£ ļ®öĒāĆļČäņäØņŚÉ ņØśĒĢśļ®┤, ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ņĀäļ░śņĀüņØĖ ņ”Øņāü, ņŗØĒøä Ēżļ¦īĻ░É, ņĪ░ĻĖ░ ļ¦īļ│ĄĻ░ÉņŚÉ ļīĆĒĢ┤ ĒÜ©Ļ│╝ņĀüņØ┤ņŚłļŗż[67]. ņØ┤ ņĢĮņĀ£ļŖö 3ņāü ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ņŚÉņä£ ņśżņŗ¼ ņ”ØņāüņØĆ ņ£ĀņØśĒĢ£ ĒśĖņĀäņØä ļ│┤ņśĆņ£╝ļéś ņĀäļ░śņĀü ņåīĒÖöļČłļ¤ē ņ”Øņāü ĒśĖņĀäņØ┤ ņ£äņĢĮĻĄ░Ļ│╝ ņ░©ņØ┤Ļ░Ć ņŚåņ¢┤ ņśüĻĄŁĻ│╝ ļ»ĖĻĄŁņŚÉņä£ļŖö ņé¼ņÜ®ĒĢĀ ņłś ņŚåņ¦Ćļ¦ī ĒĢ£ĻĄŁņŚÉņä£ļŖö ņé¼ņÜ®ņØ┤ Ļ░ĆļŖźĒĢśļŗż[68].
5-HT4 ņłśņÜ®ņ▓┤ ņ×æņÜ®ņĀ£ ņżæ ļīĆĒæ£ņĀüņØĖ ņĢĮņĀ£ļŖö cisaprideņÖĆ tegaserodņØ┤ņ¦Ćļ¦ī ļČĆņĀĢļ¦źĻ│╝ ņŗ¼ĒśłĻ┤Ć ņ¦łĒÖś ņ£Āļ░£ Ļ░ĆļŖźņä▒ņØ┤ ļ│┤Ļ│ĀļÉśņ¢┤ ļæÉ ņĢĮļ¼╝ ļ¬©ļæÉ Ēśäņ×¼ļŖö ņŗ£ņןņŚÉņä£ Ēć┤ņČ£ļÉ£ ņāüĒā£ņØ┤ļŗż. Ēśäņ×¼ ņé¼ņÜ®Ļ░ĆļŖźĒĢ£ 5-HT4 ņłśņÜ®ņ▓┤ ņ×æņÜ®ņĀ£ņØĖ mosaprideļŖö ļČĆņĀĢļ¦ź ņ£Āļ░£Ļ│╝ Ļ░ÖņØĆ ļČĆņ×æņÜ®ņØĆ ļ│┤Ļ│ĀļÉ£ ļ░ö ņŚåņ£╝ļ®░, ņ£äņןĻ┤Ć ņÜ┤ļÅÖĻ│╝ ņ£äļ░░ņČ£ņØä ņ┤ēņ¦äĒĢ£ļŗż[69]. MosaprideļŖö RCT ņŚ░ĻĄ¼ņŚÉņä£ ņĀäļ░śņĀüņØĖ ņéČņØś ņ¦łņØä Ļ░£ņäĀņŗ£ņ╝░ņ£╝ļéś ņĀäļ░śņĀü ņåīĒÖöļČłļ¤ē ņ”Øņāü Ļ░£ņäĀņØĆ ņ£äņĢĮņŚÉ ļ╣äĒĢśņŚ¼ ņÜ░ņøöĒĢ£ ĒÜ©Ļ│╝ļź╝ ļ│┤ņŚ¼ņŻ╝ņ¦Ć ļ¬╗ĒĢśņśĆļŗż[70,71]. ņĄ£ĻĘ╝ 13Ļ░£ņØś RCTņŚÉ ļīĆĒĢ£ mosapride ļ®öĒāĆļČäņäØņŚÉņä£ ņåīĒÖöļČłļ¤ē ņ”Øņāü Ļ░£ņäĀņŚÉ ņ£ĀņØśĒĢ£ ĒÜ©Ļ│╝ ņ░©ņØ┤Ļ░Ć ņŚåņŚłņ£╝ļéś ņŚ░ĻĄ¼ļ¦łļŗż ņ¦äļŗ©ĻĖ░ņżĆņØ┤ ļŗżļźĖ ņĀ£ĒĢ£ņĀÉņØ┤ ņ׳ņ¢┤ņä£ ņÜ░ņłśĒĢśĻ▓ī ĒåĄņĀ£ļÉ£ 4Ļ░£ņØś ņŚ░ĻĄ¼ņŚÉ ļīĆĒĢ£ ĒĢśņ£ä ļČäņäØ Ļ▓░Ļ│╝, mosaprideĻ░Ć ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņŚÉ ĒÜ©Ļ│╝ņĀüņØ┤ņŚłļŗż(RR = 1.11, 95% CI = 1.01-1.23, p=0.029) [72]. ĻĘĖļ¤¼ļ»ĆļĪ£ 5-HT4 ņłśņÜ®ņ▓┤ ņ×æņÜ®ņĀ£Ļ░Ć ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ņ╣śļŻīņŚÉ ĒÜ©Ļ│╝ņĀüņØ┤ļØ╝ļŖö ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ņÖĆ ņŗżņĀ£ ņ×äņāüņŚÉņä£ ļČĆņ×æņÜ®ņØ┤ ņĀüļŗżļŖö ņĀÉņØä ņóģĒĢ®ņĀüņ£╝ļĪ£ Ļ│ĀļĀżĒĢĀ ļĢī, ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņŚÉ ņ׳ņ¢┤ mosaprideĻ░Ć ĻČīĻ│ĀļÉ£ļŗż[73-75].
ņĄ£ĻĘ╝ņŚÉļŖö ņä£ļ░®ĒśĢ 1ņØ╝ 1ĒÜī ņÜöļ▓Ģ(ĻĖ░ņĪ┤ņØś ĒĢśļŻ© 3ļ▓ł ņÜ®ļ▓ĢņŚÉņä£ Ļ░ÉņåīļÉ£)ņØś mosapride ņĀ£ĒśĢņØ┤ Ļ░£ļ░£ļÉśņŚłļŗż. ņĄ£ĻĘ╝ ņŚ░ĻĄ¼ņŚÉņä£ 138ļ¬ģņØś ĒÖśņ×Éļź╝ ļæÉ ĻĄ░ņ£╝ļĪ£ ļéśļłäņ¢┤ ņä£ļ░®ĒśĢ ņĀ£ņĀ£ņÖĆ ĻĖ░ņĪ┤ ņÜ®ļ▓Ģ ņĀ£ņĀ£ļź╝ Ēł¼ņŚ¼ĒĢ£ Ēøä, ņåīĒÖöļČłļ¤ē ņ”ØņāüņØś ĒśĖņĀäĻ│╝ ļČĆņ×æņÜ®ņØä ļ╣äĻĄÉĒĢśņśĆņØä ļĢī, 1ĒÜī ļ│ĄņÜ® ņä£ļ░®ņĀĢ Ēł¼ņŚ¼ļ▓ĢņØ┤ ĻĖ░ņĪ┤ ņÜ®ļ▓ĢņŚÉ ļ╣äĒĢ┤ņä£ ņŚ┤ļō▒ĒĢśņ¦Ć ņĢŖļŖö Ļ▓āņ£╝ļĪ£ ĒÖĢņØĖļÉśņŚłļŗż. ņĢĮņĀ£ ņł£ņØæļÅä ņĖĪļ®┤ņØä Ļ│ĀļĀżĒĢśļ®┤ 1ĒÜī Ēł¼ņĢĮ ņÜ®ļ▓ĢņØĆ Ē¢źĒøä ņ×äņāüņŚÉņä£ ņóŗņØĆ ņäĀĒāØņØ┤ ļÉĀ Ļ▓āņØ┤ļŗż[76].
2007ļģä ļ░£Ēæ£ļÉ£ ļŗżņ¢æĒĢ£ ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£ļōżņØś ĒÜ©Ļ│╝ļź╝ ņŚ░ĻĄ¼ĒĢ£ ļ®öĒāĆļČäņäØ Ļ▓░Ļ│╝ļź╝ ļ│┤ļ®┤, ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£Ļ░Ć ņ£äņĢĮĻĄ░ņŚÉ ļ╣äĒĢ┤ņä£ ņ╣śļŻī ĒÜ©Ļ│╝ļź╝ ņ¢╗ņØä ĒÖĢļźĀņØ┤ 30%Ļ░Ć ļŹö ļåÆņĢśļŗż(95% CI = 0.21-0.38, p< 0.001). ĒĢśņ¦Ćļ¦ī ļČĆņ×æņÜ®ņ£╝ļĪ£ ņØĖĒĢ┤ ļŹö ņØ┤ņāü ņé¼ņÜ®ļÉśņ¦Ć ņĢŖļŖö cisaprideĻ░Ć Ļ░Ćņן ļ¦ÄņØ┤ ĒżĒĢ©ļÉ£ ņŚ░ĻĄ¼ļĪ£ Ļ▓░Ļ│╝ ĒĢ┤ņäØņŚÉ ņŻ╝ņØśĻ░Ć ĒĢäņÜöĒĢśļŗż[77]. 38Ļ░£ ņŚ░ĻĄ¼ņŚÉ ļīĆĒĢ£ ļ®öĒāĆļČäņäØņŚÉņä£, ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£ļŖö ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ņä£ ņĀäļ░śņĀüņØĖ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ņ”ØņāüņØä ņØśļ»Ė ņ׳Ļ▓ī Ļ░Éņåīņŗ£ņ╝░Ļ│Ā(NNT = 7), ņéČņØś ņ¦łņØ┤ļéś ņĢĮņĀ£ ļČĆņ×æņÜ®ņŚÉļŖö ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż[78]. ļśÉĒĢ£ ņĄ£ĻĘ╝ 25Ļ░£ņØś ņŚ░ĻĄ¼(4,473ļ¬ģ)ņŚÉ ļīĆĒĢ£ ļ▓ĀņØ┤ņ¦ĆņĢł ļäżĒŖĖņøīĒü¼ ļČäņäØņØä ņØ┤ņÜ®ĒĢ£ ļ®öĒāĆļČäņäØ Ļ▓░Ļ│╝, ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£Ļ░Ć ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ĒÜ©Ļ│╝ņĀüņØĖ ņ╣śļŻīņĀ£ņ×äņØä ĒÖĢņØĖĒĢśņśĆļŗż. ĒŖ╣Ē׳, league-to-league ļČäņäØļ▓ĢņØä ņØ┤ņÜ®ĒĢśņŚ¼ ļ╣äĻĄÉĒĢśņśĆņØä ļĢī itoprideļéś acotiamideļ│┤ļŗż metoclopramide, trimebutine, mosapride, domperidone ņĢĮņĀ£ļōżņØ┤ ļŹö ņóŗņØĆ ĒÜ©Ļ│╝ļź╝ ļ│┤ņśĆļŗż[79].
DA-9701 (motilitone┬«)ņØĆ Pharbitidis semenĻ│╝ Corydalis tuberņŚÉņä£ ņČöņČ£ĒĢ£ ņĢĮņĀ£ļĪ£ ņ£äļ░░ņČ£ļŖź ļ░Å ņ£äņĀĆļČĆ ņĀüņØæļŖźļĀźņØä Ē¢źņāüņŗ£ĒéżĻ│Ā, ļé┤ņןĻ│╝ļ»╝ņä▒ņŚÉļÅä ĒÜ©Ļ│╝Ļ░Ć ņ׳ņŚłļŗż. 389ļ¬ģņØś ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×Éļź╝ ņäĖ ĻĘĖļŻ╣(motilitoneņ╣śļŻīĻĄ░, PPI ņ╣śļŻīĻĄ░, motilitone + PPI ņ╣śļŻīĻĄ░)ņ£╝ļĪ£ ļéśļłäņ¢┤ ļ╣äĻĄÉĒĢśņśĆņØä ļĢī ļ¬©ļōĀ ĻĘĖļŻ╣ņŚÉņä£ ņåīĒÖöļČłļ¤ē ņ”ØņāüĻ│╝ ņéČņØś ņ¦łņØ┤ ņØśļ»Ė ņ׳Ļ▓ī ĒśĖņĀäļÉśņŚłļŗż[80].
ņ”Øņāü ņĪ░ņĀłņØ┤ ņל ļÉśņ¦Ć ņĢŖļŖö ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņØś Ļ▓ĮņÜ░, metoclopramideņÖĆ domperidoneĻ│╝ Ļ░ÖņØĆ ļæÉ ņóģļźśņØś ņ£äņןĻ┤Ć ņÜ┤ļÅÖ ņ┤ēņ¦äņĀ£ļź╝ ļ│æĒĢ®ĒĢśņŚ¼ ņé¼ņÜ®ĒĢśļŖö Ļ▓āļÅä ĒÜ©Ļ│╝Ļ░Ć ņ׳ņŚłļŗż[81,82]. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņŚÉ ļīĆĒĢ£ ņ£äņןĻ┤Ć ņÜ┤ļÅÖ ņ┤ēņ¦äņĀ£ņØś ĻĖ░ņĀä, ļ│ĄņÜ® ņÜ®ļ¤ē, ļČĆņ×æņÜ® ļō▒ņØĆ Ēæ£ 3ņŚÉ ņÜöņĢĮĒĢśņśĆļŗż.
8. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ņĢäĒśĢ ņżæ ņŗØĒøäĻ│ĀĒåĄņ”ØĒøäĻĄ░ ĒÖśņ×ÉņŚÉņä£ ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£ļź╝ 1ņ░© ņ╣śļŻī ņĢĮņĀ£ļĪ£ ņÜ░ņäĀņĀüņ£╝ļĪ£ ĻČīĻ│ĀĒĢ£ļŗż.
ŌĆó ĻČīĻ│Ā ļō▒ĻĖē: Ļ░ĢĒĢ©
ŌĆó ņ”ØĻ▒░ ņłśņżĆ: ļé«ņØī
ŌĆó ņĀäļ¼ĖĻ░Ć ņØśĻ▓¼: ņĀäņĀüņ£╝ļĪ£ ļÅÖņØśĒĢ©(32.2%), ļīĆņ▓┤ļĪ£ ļÅÖņØśĒĢ©(60.7%), ņØ╝ļČĆ ļÅÖņØśĒĢ©(7.1%), ļīĆņ▓┤ļĪ£ ļÅÖņØśĒĢśņ¦Ć ņĢŖņØī(0%), ņĀäņĀüņ£╝ļĪ£ ļÅÖņØśĒĢśņ¦Ć ņĢŖņØī(0%), ļ¬©ļź┤Ļ▓ĀņØī(0%)
ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×É ņżæ ņŗØĒøä Ēżļ¦īĻ░É ļśÉļŖö ņĪ░ĻĖ░ ļ¦īļ│ĄĻ░ÉņØä ĒśĖņåīĒĢśļŖö PDS ņ£ĀĒśĢņØĆ ļ¦żņÜ░ ĒØöĒĢśļŗż[83]. ņ£äņĀĢņ▓┤ ņ”Øņāü(gastric stasis symptom)ĻĄ░Ļ│╝ EPSĻĄ░ņ£╝ļĪ£ ļéśļłäņ¢┤ ļČäņäØĒĢ£ ņØ╝ļ│ĖņØś ļīĆĻĘ£ļ¬© mosapride ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤, ņ£äņĀĢņ▓┤ ņ”ØņāüĻĄ░ņŚÉņä£ mosapride Ēł¼ņŚ¼Ļ░Ć ņØśļ»Ė ņ׳ļŖö ņ”Øņāü Ļ░£ņäĀņØä ļ│┤ņśĆļŗż[73]. ļśÉĒĢ£ EPSĻĄ░Ļ│╝ PDSĻĄ░ņØ┤ ļ¬©ļæÉ ĒżĒĢ©ļÉ£ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ 1ņØ╝ 3ĒÜī ļ│ĄņÜ®ĒĢśļŖö mosaprideņÖĆ 1ņØ╝ 1ĒÜī ļ│ĄņÜ®ĒĢśļŖö ņä£ļ░®ĒśĢ mosaprideņØä ļ╣äĻĄÉĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£, PDSĻĄ░ņŚÉņä£ ļ¬©ļæÉ ņ”Øņāü ĒśĖņĀäņØä ļ│┤ņśĆņ£╝ļéś ļæÉ ņĢĮņĀ£ Ļ░ä ņ░©ņØ┤ļŖö ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż[76]. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņŚÉņä£ itoprideņØś ĒÜ©Ļ│╝ņŚÉ ļīĆĒĢ£ ļ®öĒāĆļČäņäØņŚÉņä£ domperidoneĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ itoprideĻ░Ć ņŗØĒøä Ēżļ¦īĻ░ÉĻ│╝ ņĪ░ĻĖ░ ļ¦īļ│ĄĻ░ÉņŚÉņä£ ņ£ĀņØśĒĢ£ ĒÜ©Ļ│╝ļź╝ ļ│┤ņśĆļŗż[67].
AcotiamideļŖö ņןĻ┤Ć ņŗĀĻ▓ĮĻ│äņŚÉņä£ M1 ļ░Å M2 ļ¼┤ņŖżņ╣┤ļ”░ ņłśņÜ®ņ▓┤ņØś ĻĖĖĒĢŁņ×æņÜ®Ļ│╝ ņĢäņäĖĒŗĖņĮ£ļ”░ ļČäĒĢ┤ĒÜ©ņåīņŚÉ ļīĆĒĢ£ ņ¢ĄņĀ£ņ×æņÜ®ņØä ĒåĄĒĢ┤ ņĢäņäĖĒŗĖņĮ£ļ”░ ļČäļ╣äļź╝ ņ”ØĻ░Ćņŗ£ņ╝£ ņ£äņןĻ┤Ć ņÜ┤ļÅÖ ĒÖ£ļÅÖņØä ņ┤ēņ¦äņŗ£ĒéżļŖö ņĢĮņĀ£ņØ┤ļŗż[84]. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ acotiamideļź╝ 4ņŻ╝ ļÅÖņĢł Ēł¼ņĢĮĒĢ£ RCT Ļ▓░Ļ│╝, ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ņåīĒÖöļČłļ¤ē ņ”ØņāüņØś ņżæņ”ØļÅäĻ░Ć ĒśĖņĀäļÉśņŚłĻ│Ā[85], ņØ┤ļŖö acotiamideĻ░Ć ņ£äņĀüņØæĻ│╝ ņ£äļ░░ņČ£ļŖźņØä ĒśĖņĀäņŗ£ņ╝£ ņ”Øņāü Ļ░£ņäĀņØä Ļ░ĆņĀĖņśżĻĖ░ ļĢīļ¼ĖņØ┤ļØ╝Ļ│Ā ņĢīļĀżņĀĖ ņ׳ļŗż[86]. 7Ļ░£ņØś RCTņŚÉ ĻĘ╝Ļ▒░ĒĢ£ ļ®öĒāĆļČäņäØņŚÉņä£ļÅä acotiamideĻ░Ć ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ņä£ PDSņŚÉ Ļ┤ĆļĀ©ļÉ£ ņ”Øņāü ĒśĖņĀäņŚÉ ĒÜ©Ļ│╝ņĀüņØ┤ņŚłņ£╝ļ®░[87], ņéČņØś ņ¦łņŚÉ ņØśļ»Ė ņ׳ļŖö ĒśĖņĀäņØä ļ│┤ņśĆļŗż[88,89]. ĻĘĖļ¤¼ļéś ņØ┤ ņĢĮņØĆ ĻĄŁļé┤ņŚÉņä£ ņĢäņ¦ü ņé¼ņÜ®ņØ┤ ļČłĻ░ĆļŖźĒĢśĻ│Ā, ļŗżļźĖ ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£ņÖĆņØś ļ╣äĻĄÉ ņŚ░ĻĄ¼Ļ░Ć ļČĆņĪ▒ĒĢ£ ņāüĒā£ņØ┤ļŗż. ErythromycinņØĆ ņ£äļ░░ņČ£ņØä ņ┤ēņ¦äņŗ£ĒéżļŖö ļŹ░ ĒÜ©Ļ│╝ņĀüņØĖ ļ¬©ĒŗĖļ”░ ņłśņÜ®ņ▓┤ ņ×æņÜ®ņĀ£ņØ┤ļ®░, ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ĒīĮļ¦īĻ░É Ļ┤ĆļĀ© ņ”ØņāüņØś ĒśĖņĀäņØä ļ│┤ņśĆļŗż[90]. ĻĘĖļ¤¼ļéś RCTņŚÉņä£ļŖö ņ£äņĢĮĻ│╝ ļ╣äĻĄÉĒĢśņśĆņØä ļĢī erythromycin Ēł¼ņĢĮĻĄ░ņŚÉņä£ ņ£äļ░░ņČ£ņŚÉ ļīĆĒĢ┤ ĒåĄĻ│äņĀüņØĖ ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśĻ│Ā, Ēśäņ×¼ ĻĄŁļé┤ņŚÉņä£ ņé¼ņÜ®ļÉśņ¦Ć ņĢŖĻ│Ā ņ׳ļŗż[91].
9. ņןĻĖ░Ļ░ä ļÅäĒīīļ»╝ņłśņÜ®ņ▓┤ ĻĖĖĒĢŁņĀ£ ļ│ĄņÜ®ņØĆ ļ╣äĻ░ĆņŚŁņĀüņØĖ ņĢĮņĀ£ ļČĆņ×æņÜ®ņØä ņĢ╝ĻĖ░ĒĢĀ ņłś ņ׳ņ£╝ļ»ĆļĪ£ ļŗ©ĻĖ░Ļ░äņØś ņĄ£ņåī ņé¼ņÜ®ņØä Ļ│ĀļĀżĒĢ£ļŗż.
ŌĆó ĻČīĻ│Ā ļō▒ĻĖē: Ļ░ĢĒĢ©
ŌĆó ņ”ØĻ▒░ ņłśņżĆ: ļé«ņØī
ņ£äņĢĮ ļīĆļ╣ä ĒÜ©Ļ│╝Ļ░Ć ņ”Øļ¬ģļÉ£ ļīĆļČĆļČäņØś ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£ļŖö D2 ņłśņÜ®ņ▓┤(dopamine receptor type 2) ĻĖĖĒĢŁņĀ£ņØ┤ļŗż. MetoclopramideļŖö ņāüņÜ®ļ¤ēņØś Ēł¼ņĢĮņ£╝ļĪ£ļÅä ĻĖēņä▒ ĻĘ╝ĻĖ┤ņןņØ┤ņāüļ░śņØæ(tardive dyskinesia)ņØä ņĢ╝ĻĖ░ĒĢĀ ņłś ņ׳ļŗż. ņČöņ▓┤ņÖĖļĪ£Ļ│ä ņ£ĀĒĢ┤ĒÜ©Ļ│╝ņØś ņ£äĒŚśļÅäļŖö ļłäņĀü ņÜ®ļ¤ēņŚÉ ļö░ļØ╝ ņ”ØĻ░ĆĒĢśļ®░, ņØ╝ļ░śņĀüņ£╝ļĪ£ ļ╣äĻ░ĆņŚŁņĀüņØĖ Ļ▓ĮņÜ░Ļ░Ć ļ¦Äņ£╝ļ®░ ņ▓ŁņåīļģäĻĖ░ ĒÖśņ×ÉņŚÉņä£ ļŹö ĒØöĒĢśĻ▓ī ļ░£ņāØĒĢ£ļŗż[92]. Ēśäņ×¼ ņŗØĒÆłņØśņĢĮĒÆłņĢłņĀäņ▓śņŚÉņä£ ļŗ©ĻĖ░Ļ░ä(ņĄ£ļīĆ 5ņØ╝ ņØ┤ļé┤)ņØś ņé¼ņÜ®ņØä ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż.
DomperidoneņØĆ QT-Ļ░äĻ▓® ņŚ░ņן ņ”ØĒøäĻĄ░ ļ░Å ņ╣śļ¬ģņĀüņØĖ ļČĆņĀĢļ¦źņØä ņØ╝ņ£╝Ēé¼ ņłś ņ׳ļŗż[93,94]. ņŗØĒÆłņØśņĢĮĒÆłņĢłņĀäņ▓śļŖö ņØ╝ļ░śņĀüņØĖ ņåīĒÖöļČłļ¤ēņØś ņÖäĒÖö ļ¬®ņĀüņ£╝ļĪ£ ĒĢśļŻ© ņ┤Ø 30 mgņØä ņĄ£ļīĆ 1ņŻ╝Ļ╣īņ¦Ćļ¦ī ĒŚłņÜ®ĒĢśĻ│Ā ņ׳ļŗż. ļ¦īņØ╝ QT-Ļ░äĻ▓®ņŚ░ņןņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ļŖö ņĢĮļ¼╝ļōż(quinolone, clarithromycin, isoniazid, fluoxetine ļō▒)ņØä ļ│ĄņÜ® ņżæņØĖ ĒÖśņ×ÉņŚÉĻ▓ī domperidoneņØĆ ļŹöņÜ▒ ņ╣śļ¬ģņĀüņØ╝ ņłś ņ׳ļŗż. 5-10Ļ░£ņøö ļÅÖņĢł levosulpirideļź╝ ļ│ĄņÜ®ĒĢ£ 60ņäĖ ņØ┤ņāüņØś ĒÖśņ×É ņżæ ņØ╝ļČĆņŚÉņä£ ĒīīĒé©ņŖ©ņ”Ø, ļ¢©ļ”╝ Ļ░ÖņØĆ ņÜ┤ļÅÖ ņןņĢĀĻ░Ć ĒÖĢņØĖļÉśņŚłĻ│Ā, levosulpiride ņżæļŗ© ĒøäņŚÉļÅä ņØ┤ļ¤¼ĒĢ£ ņ”ØņāüņØ┤ ĒśĖņĀäļÉśņ¦Ć ņĢŖļŖö Ļ▓ĮņÜ░Ļ░Ć ņ׳ņ¢┤ Ļ│ĀļĀ╣ ĒÖśņ×ÉņŚÉĻ▓ī ņןĻĖ░Ļ░ä Ēł¼ņŚ¼ĒĢĀ ļĢī ņŻ╝ņØśĻ░Ć ĒĢäņÜöĒĢśļŗż[95].
ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ņĀ£ĻĘĀ ņ╣śļŻī
10. ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ņĀ£ĻĘĀ ņ╣śļŻīļŖö ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ņןĻĖ░ņĀüņØĖ ņ”Øņāü ņÖäĒÖöņŚÉ ļÅäņøĆņØ┤ ļÉśĻĖ░ ļĢīļ¼ĖņŚÉ ĻČīĻ│ĀĒĢ£ļŗż.
ŌĆó ĻČīĻ│Ā ļō▒ĻĖē: ņĢĮĒĢ©
ŌĆó ņ”ØĻ▒░ ņłśņżĆ: ļåÆņØī
ŌĆó ņĀäļ¼ĖĻ░Ć ņØśĻ▓¼: ņĀäņĀüņ£╝ļĪ£ ļÅÖņØśĒĢ©(18.5%), ļīĆņ▓┤ļĪ£ ļÅÖņØśĒĢ©(55.6%), ņØ╝ļČĆ ļÅÖņØśĒĢ©(25.9%), ļīĆņ▓┤ļĪ£ ļÅÖņØśĒĢśņ¦Ć ņĢŖņØī(0%), ņĀäņĀüņ£╝ļĪ£ ļÅÖņØśĒĢśņ¦Ć ņĢŖņØī(0%), ļ¬©ļź┤Ļ▓ĀņØī(0%)
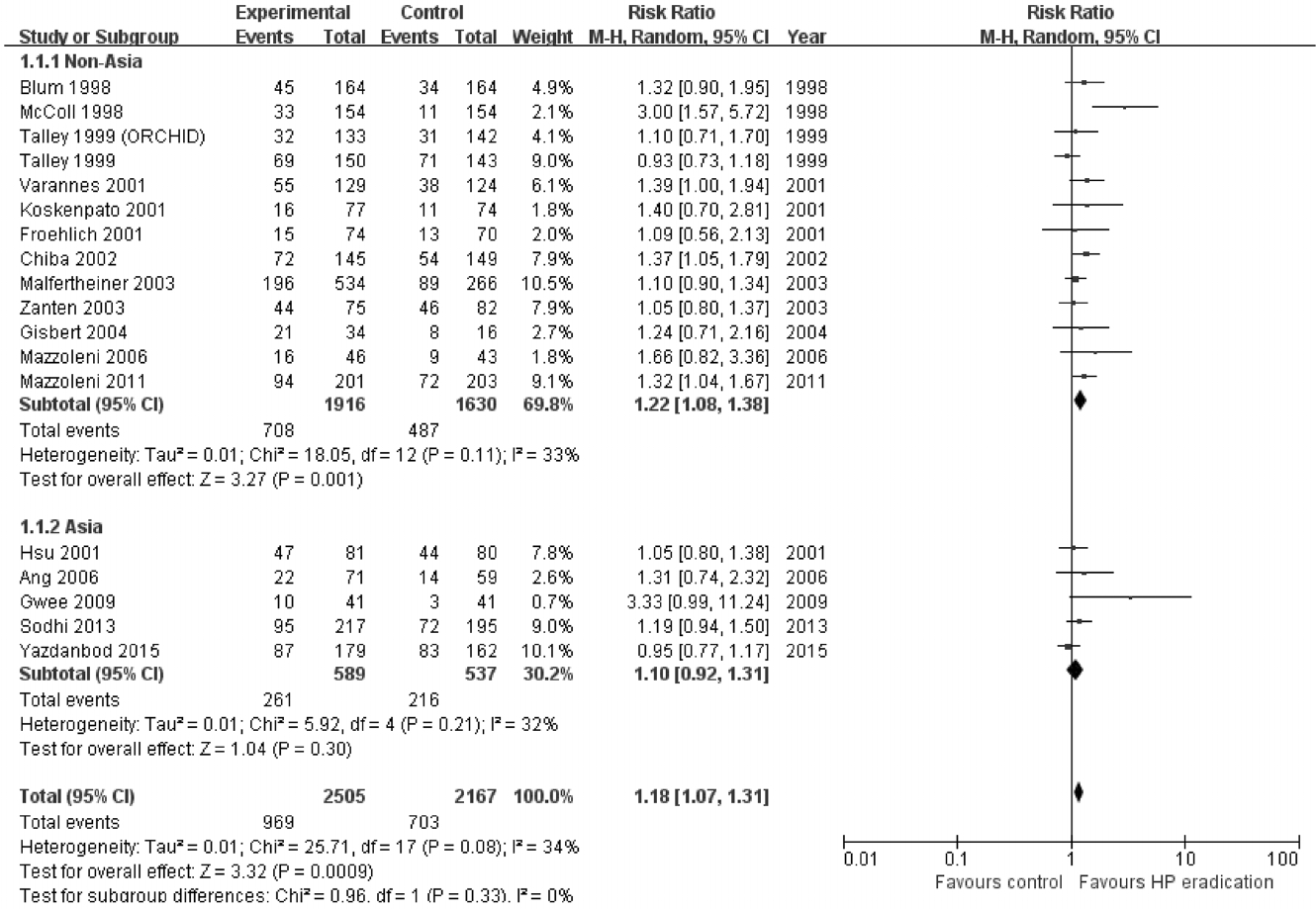
ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉ ļīĆĒĢ£ H. pylori ņĀ£ĻĘĀ ņ╣śļŻīņØś ĒÜ©Ļ│╝ļź╝ ļČäņäØĒĢ£ RCTļź╝ ļīĆņāüņ£╝ļĪ£ ņŗ£Ē¢ēĒĢ£ ļ®öĒāĆļČäņäØņŚÉ ļö░ļź┤ļ®┤, H. pylori ņĀ£ĻĘĀ ņ╣śļŻīĻĄ░ņŚÉņä£ 6Ļ░£ņøö ņØ┤ņāü ņןĻĖ░Ļ░ä ņČöņĀü Ļ┤Ćņ░░ņØä ĒĢśņśĆņØä ļĢī, ņ×æņ¦Ćļ¦ī ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢ£ ņåīĒÖöļČłļ¤ē ņ”Øņāü Ļ░£ņäĀņØ┤ Ļ┤Ćņ░░ļÉśņŚłņ£╝ļéś[18,96], 3Ļ░£ņøöņØś ļŗ©ĻĖ░Ļ░ä ņČöņĀü Ļ┤Ćņ░░ ņŗ£ņŚÉ ĻĘĖ ĒÜ©Ļ│╝ļŖö ņ£ĀņØśĒĢśņ¦Ć ņĢŖņĢśļŗż[96]. 14Ļ░£ņØś RCTļź╝ ļČäņäØĒĢ£ ĒĢ£ ļ®öĒāĆļČäņäØņŚÉņä£ļŖö ņĀ£ĻĘĀ ņ╣śļŻīĻĄ░ņŚÉņä£ ņåīĒÖöļČłļ¤ē ņ”ØņāüņØś ĒśĖņĀäņØä ļ│┤ņŚ¼ņŻ╝ņŚłņ£╝ļéś[18], 25Ļ░£ RCTļź╝ ļČäņäØĒĢ£ ļŗżļźĖ ļ®öĒāĆļČäņäØņŚÉņä£ļŖö ņ”Øņāü ĒśĖņĀäņØ┤ļéś ņéČņØś ņ¦łņØś ņ£ĀņØśĒĢ£ ņ░©ņØ┤Ļ░Ć ņŚåĻ│Ā ļČĆņ×æņÜ®ņØĆ ļåÆļŗżļŖö ņāüļ░śļÉ£ Ļ▓░Ļ│╝ļź╝ ļ│┤ņśĆļŗż[96]. ņ£Āļ¤ĮĻ│╝ ļ»ĖĻĄŁ ļ░Å ņ║ÉļéśļŗżņØś ņ¦äļŻī ņ¦Ćņ╣©ņŚÉņä£ļŖö ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ H.pylori ņĀ£ĻĘĀ ņ╣śļŻīļź╝ Ļ░ĢļĀźĒ׳ ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż[12,17].
ņØ┤ļ▓ł Ļ░£ņĀĢĒīÉņŚÉņä£ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ H. pylori ņĀ£ĻĘĀ ņ╣śļŻī ĒÜ©Ļ│╝ļź╝ ĒÖĢņØĖĒĢśĻĖ░ ņ£äĒĢśņŚ¼ 1997ļģä 1ņøöļČĆĒä░ 2017ļģä 12ņøöĻ╣īņ¦Ć ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×Éļź╝ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä 6Ļ░£ņøö ņØ┤ņāü ņČöņĀü Ļ┤Ćņ░░ĒĢ£ 18Ļ░£ņØś RCTņŚÉ ļīĆĒĢ£ ļ®öĒāĆļČäņäØņØä ņŗ£Ē¢ēĒĢśņśĆļŗż(Table 4, Figs. 4 and 5) [97-114]. H. pylori ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ĒĢ£ ĻĄ░ņŚÉņä£ ņåīĒÖöļČłļ¤ē ņ”ØņāüņØ┤ ņ£ĀņØśĒĢśĻ▓ī Ļ░£ņäĀļÉśņŚłņ£╝ļéś(RR 1.18, 95% CI = 1.07-1.31) ņŚ░ĻĄ¼Ļ░ä ņØ┤ņ¦łņä▒ņØĆ ņżæĻ░ä ņĀĢļÅäņśĆĻ│Ā(Žć2 = 25.7, p= 0.08, I2 = 34%) (Fig. 5), NNTļŖö 14ļ¬ģ(95% CI = 11-18)ņ£╝ļĪ£ ĻĘĖ ņ╣śļŻī ĒÜ©Ļ│╝ļŖö Ēü¼ņ¦Ć ņĢŖņĢśļŗż. ņŚ░ĻĄ¼Ļ░Ć ņŗ£Ē¢ēļÉ£ ņ¦ĆņŚŁņŚÉ ļö░ļØ╝ ĒĢśņ£ä ļČäņäØņØä ņŗ£Ē¢ēĒĢśņśĆļŖöļŹ░, ņĢäņŗ£ņĢäņŚÉņä£ 5 Ļ░£ņØś RCTĻ░Ć ņ׳ņŚłĻ│Ā ņĢäņŗ£ņĢä ņØ┤ņÖĖ ņ¦ĆņŚŁņŚÉņä£ 13Ļ░£ņØś RCTĻ░Ć ņ׳ņŚłļŗż. H. pylori ņĀ£ĻĘĀ ņ╣śļŻīļŖö ņĢäņŗ£ņĢä ņØ┤ņÖĖ ņ¦ĆņŚŁņØś ņŚ░ĻĄ¼ņŚÉņä£ ĒśäņĀĆĒĢ£ ņØ┤ņ¦łņä▒(Žć2 = 18.1, p= 0.11, I2 = 33%) ņŚåņØ┤ ņåīĒÖöļČłļ¤ē ņ”ØņāüņØä ņ£ĀņØśĒĢśĻ▓ī Ļ░£ņäĀņŗ£ņ╝░ļŗż(RR = 1.22; 95% CI = 1.08-1.38). ĻĘĖļ¤¼ļéś ņĢäņŗ£ņĢä ņ¦ĆņŚŁņŚÉņä£ ņłśĒ¢ēļÉ£ RCTļōżņØś ļ®öĒāĆļČäņäØ Ļ▓░Ļ│╝ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņŚÉ ļīĆĒĢ£ H.pylori ņĀ£ĻĘĀ ņ╣śļŻīņØś ĒÜ©Ļ│╝Ļ░Ć ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢśņ¦Ć ņĢŖņĢśņ£╝ļ®░(RR = 1.10, 95% CI = 0.92-1.31), ņŚ░ĻĄ¼ Ļ░äņØś ņØ┤ņ¦łņä▒ļÅä ļé«ņĢśļŗż(Žć2 = 5.9, p= 0.21, I2 = 32%).
ņÜöņĢĮĒĢśļ®┤ ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉņŚÉņä£ H. pylori ņĀ£ĻĘĀ ņ╣śļŻīļŖö ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢ£ ņ”Øņāü ĒśĖņĀäņØä ļ│┤ņśĆņ£╝ļéś NNTĻ░Ć Ēü¼Ļ│Ā, ņĢäņŗ£ņĢäņŚÉņä£ ņłśĒ¢ēļÉ£ RCTļź╝ ļīĆņāüņ£╝ļĪ£ ĒĢ£ ļ®öĒāĆļČäņäØņŚÉņä£ļŖö ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢśņ¦Ć ņĢŖņĢä ļåÆņØĆ H. pylori ņ£Āļ│æļźĀ, ņĀ£ĻĘĀ ņ╣śļŻīļĪ£ ņØĖĒĢ£ ņĢĮņĀ£ ļ╣äņÜ® ļ░Å ņĢĮļ¼╝ ļČĆņ×æņÜ®, ļé┤ņä▒ĻĘĀņØś ņČ£Ēśä ņ£äĒŚś, ņ×¼Ļ░ÉņŚ╝ņØś ņ£äĒŚś ļō▒ņØä Ļ│ĀļĀżĒĢśņŚ¼ ņØ┤ļ▓ł ņ¦Ćņ╣©ņŚÉņä£ļŖö ņĢĮĒĢ£ ĻČīĻ│Āļź╝ ņäĀĒāØĒĢśņśĆļŗż.
ņ£ä ĻĖ░ņĀĆļČĆ ņØ┤ņÖäņĀ£
11. ņ£ä ĻĖ░ņĀĆļČĆ ņØ┤ņÖäņĀ£ļŖö ņĀäļ░śņĀüņØĖ ņåīĒÖöļČłļ¤ē ņ”Øņāü, ņŗØĒøä Ēżļ¦īĻ░ÉĻ│╝ ņĪ░ĻĖ░ ļ¦īļ│ĄĻ░ÉņØś ĒśĖņĀäņŚÉ ļÅäņøĆņØ┤ ļÉśņ¢┤ ĻČīĻ│ĀĒĢ£ļŗż.
ŌĆó ĻČīĻ│Ā ļō▒ĻĖē: ņĢĮĒĢ©
ŌĆó ņ”ØĻ▒░ ņłśņżĆ: ņżæļō▒ļÅä
ņŗØĒøä ĻĘ╝ņ£äļČĆņØś ņØ┤ņÖä ņןņĢĀļŖö ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņØś ņĢĮ 40%ņŚÉņä£ ņ׳ņ£╝ļ®░, ņĪ░ĻĖ░ ļ¦īļ│ĄĻ░É, ņ▓┤ņżæĻ░Éņåī ļō▒ņØś ņ”ØņāüĻ│╝ Ļ┤ĆļĀ©ņØ┤ ņ׳ļŖö ļ│æĒā£ņāØļ”¼ĻĖ░ņĀäņØ┤ļŗż[115]. BuspironeĻ│╝ tandospironeņØĆ 5-HT1 ņłśņÜ®ņ▓┤ ņ×æņÜ®ņĀ£ņØ┤ļ®░ ņ£ä ĻĖ░ņĀĆļČĆļź╝ ņØ┤ņÖäņŗ£ĒéżļŖö ĒÜ©Ļ│╝ļź╝ ļéśĒāĆļéĖļŗż[116]. ĒĢ£ ņØ┤ņżæ ļ¦╣Ļ▓Ć ĻĄÉņ░©ņŚ░ĻĄ¼ņŚÉ ņØśĒĢśļ®┤ 4ņŻ╝ ļÅÖņĢłņØś buspirone Ēł¼ņŚ¼ļŖö ņ£ä ĻĖ░ņĀĆļČĆ ņØ┤ņÖäņØä ņ£ĀņØśĒĢśĻ▓ī ņ”ØĻ░Ćņŗ£ĒéżĻ│Ā, ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ņĀäļ░śņĀüņØĖ ņåīĒÖöļČłļ¤ē ņ”ØņāüņĀÉņłśņØś Ļ░£ņäĀĻ│╝ ņŗØĒøä Ēżļ¦īĻ░É, ņĪ░ĻĖ░ ļ¦īļ│ĄĻ░É, ļ│ĄļČĆĒīĮļ¦ī ļō▒ Ļ░£ļ│ä ņ”ØņāüņØś Ļ░£ņäĀņŚÉ ĒÜ©Ļ│╝ņĀüņØ┤ņŚłļŗż[117]. TandospironeņØä 4ņŻ╝ ļÅÖņĢł Ēł¼ņŚ¼ĒĢ£ RCT ņŚ░ĻĄ¼ņŚÉņä£ļÅä ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ tandospirone Ēł¼ņŚ¼ĻĄ░ņŚÉņä£ ļ│ĄļČĆ ņ”ØņāüĻ│╝ ņāüļ│ĄļČĆĒåĄņ”ØņØ┤ ņ£ĀņØśĒĢśĻ▓ī ĒśĖņĀäļÉśņŚłļŗż[118]. Cisapride, tegaserod, mosapride ļō▒ 5-HT4 ņłśņÜ®ņ▓┤ ņ×æņÜ®ņĀ£ļŖö ņŗØĒøä ņ£ä ĻĖ░ņĀĆļČĆ ņØ┤ņÖäņØä ņ”ØĻ░Ćņŗ£ĒéżļŖö ĒÜ©Ļ│╝ļź╝ ļéśĒāĆļé┤ļ®░, ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņØś ņØ╝ļČĆņŚÉņä£ ņ”ØņāüņØä ĒśĖņĀäņŗ£Ēé©ļŗż[69,119-121]. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉĻĄ░ņŚÉņä£ acotiamideļź╝ Ēł¼ņŚ¼ĒĢ£ Ēøä ļ│ĄļČĆ ņ┤łņØīĒīīļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ņ£ä ĻĖ░ņĀĆļČĆ ņØ┤ņÖä ņĀĢļÅäļź╝ ņĖĪņĀĢĒĢśņśĆņØä ļĢī ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ņ£ĀņØśĒĢśĻ▓ī ņ£ä ĻĖ░ņĀĆļČĆ ņØ┤ņÖäņØä ņ”ØĻ░Ćņŗ£ņ╝░ļŗż[122]. ņ£ä ņŗĀĒŗ░ĻĘĖļלĒö╝ Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢ£ ņ£äņĢĮ ļīĆņĪ░ĻĄ░ ņŚ░ĻĄ¼ņŚÉņä£ acotiamideļŖö ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ņ£ä ĻĖ░ņĀĆļČĆ ņØ┤ņÖäņØä ņ£ĀņØśĒĢśĻ▓ī ņ”ØĻ░Ćņŗ£ņ╝░ņ£╝ļ®░, ņ£äņןĻ┤Ć ņ┤Ø ņ”ØņāüņĀÉņłś ļ░Å ļČłņĢł ņĀÉņłśļź╝ ņ£ĀņØśĒĢśĻ▓ī ĒśĖņĀäņŗ£ņ╝░ļŗż[86]. ņØ╝ļČĆ ĒĢŁņÜ░ņÜĖņĀ£ļÅä ņ£ä ĻĖ░ņĀĆļČĆ ņØ┤ņÖäņØä ņ”ØĻ░Ćņŗ£ĒéżļŖö ĒÜ©Ļ│╝ļź╝ ļéśĒāĆļéĖļŗż. ņØ┤ņżæ ļ¦╣Ļ▓Ć ņ£äņĢĮ ļīĆņĪ░ĻĄ░ ņŚ░ĻĄ¼ņŚÉņä£ amitriptylineĻ│╝ escitalopramņØä 12ņŻ╝ ļÅÖņĢł Ēł¼ņŚ¼ĒĢśļ®┤ņä£ ļŗ©ņØ╝ Ļ┤æņ×É ļ░®ņČ£ ņ╗┤Ēō©Ēä░ļŗ©ņĖĄņ┤¼ņśü(single-photon emission computed tomography)ņ£╝ļĪ£ ņ£ä ĻĖ░ņĀĆļČĆ ņØ┤ņÖäņØä ņĖĪņĀĢĒĢśņśĆņØä ļĢī, ņØ┤ ņĢĮņĀ£ļōżņØĆ ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ņ£ä ĻĖ░ņĀĆļČĆ ņØ┤ņÖäņØä ņ£ĀņØśĒĢśĻ▓ī Ļ░£ņäĀņŗ£ņ╝░ļŗż[123].
ĒĢŁņÜ░ņÜĖņĀ£
12. ņé╝ĒÖśĻ│ä ĒĢŁņÜ░ņÜĖņĀ£ļŖö ņé░ļČäļ╣äņ¢ĄņĀ£ņĀ£, ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£ ļō▒ ĻĖ░ņĪ┤ņØś ņ╣śļŻīņŚÉ ļ░śņØæĒĢśņ¦Ć ņĢŖļŖö ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×É ņ╣śļŻīņŚÉ ļÅäņøĆņØä ņżä ņłś ņ׳ņ¢┤ ĻČīĻ│ĀĒĢ£ļŗż.
ŌĆó ĻČīĻ│Ā ļō▒ĻĖē: ņĢĮĒĢ©
ŌĆó ņ”ØĻ▒░ ņłśņżĆ: ņżæļō▒ļÅä
ŌĆó ņĀäļ¼ĖĻ░Ć ņØśĻ▓¼: ņĀäņĀüņ£╝ļĪ£ ļÅÖņØśĒĢ©(34.6%), ļīĆņ▓┤ļĪ£ ļÅÖņØśĒĢ©(53.9%), ņØ╝ļČĆ ļÅÖņØśĒĢ©(11.5%), ļīĆņ▓┤ļĪ£ ļÅÖņØśĒĢśņ¦Ć ņĢŖņØī(0%), ņĀäņĀüņ£╝ļĪ£ ļÅÖņØśĒĢśņ¦Ć ņĢŖņØī(0%), ļ¬©ļź┤Ļ▓ĀņØī(0%)
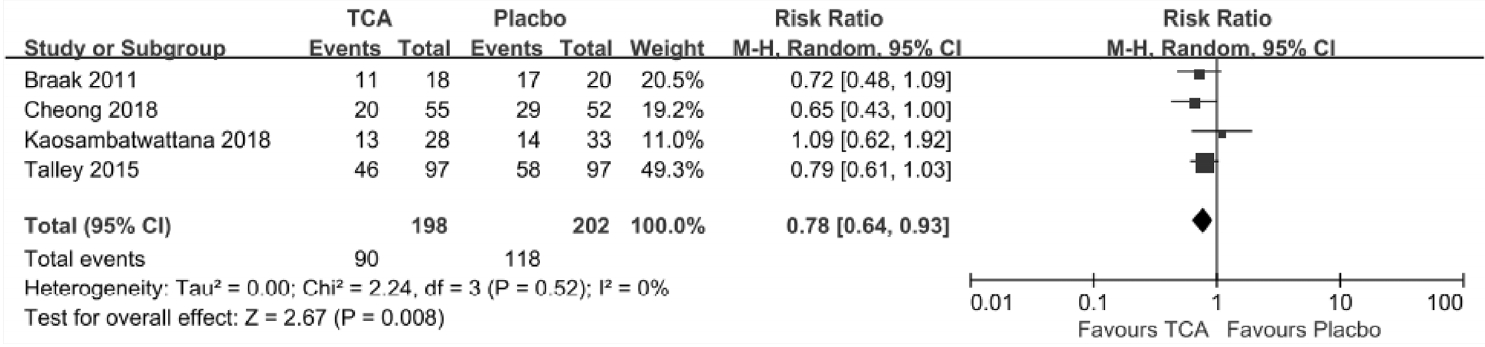
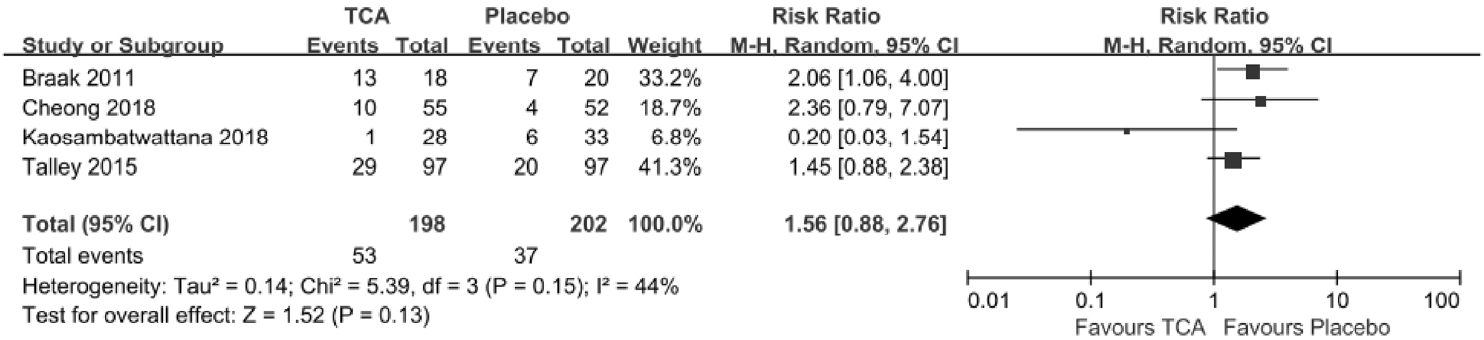
TCAļŖö ĻĖ░ļŖźņä▒ ņ£äņן ņןņĢĀĻ░Ć ņ׳ļŖö ĒÖśņ×ÉļōżņØś ņ”ØņāüņØä ĒśĖņĀäņŗ£ĒéżĻĖ░ ņ£äĒĢ┤ ņ×äņāüņŚÉņä£ ņé¼ņÜ®ļÉśĻ│Ā ņ׳ļŗż. ņĄ£ĻĘ╝ ĻĄŁļé┤ņŚÉņä£ ļ░£Ēæ£ļÉ£ Ļ│╝ļ»╝ņä▒ņןņ”ØĒøäĻĄ░ņØś ņ╣śļŻī ņ¦Ćņ╣©ņŚÉņä£ļÅä ĒĢŁņÜ░ņÜĖ ņ×æņÜ® ņØ┤ņÖĖņŚÉ ĒåĄņ”Ø ņĪ░ņĀł(pain modulation) ĻĖ░ņĀäņ£╝ļĪ£ ņ”ØņāüņØä ĒśĖņĀäņŗ£ņ╝£ TCA ņé¼ņÜ®ņØ┤ ĻČīĻ│ĀļÉ£ļŗżĻ│Ā ĻĖ░ņłĀĒĢśĻ│Ā ņ׳ļŗż[11]. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ TCAņÖĆ ņ£äņĢĮņØä ļ╣äĻĄÉĒĢ£ ļæÉ Ļ░£ņØś ņ▓┤Ļ│äņĀü ļ¼ĖĒŚīĻ│Āņ░░ ļģ╝ļ¼ĖņØ┤ ņĄ£ĻĘ╝ņŚÉ ļ░£Ēæ£ļÉśņŚłļŗż[124,125]. 4Ļ░£ņØś RCTļź╝ ĒżĒĢ©ĒĢ£ ņ▓½ ļ▓łņ¦Ė ļģ╝ļ¼ĖņŚÉņä£ TCAļŖö ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ņ╣śļŻīņŚÉ ļ░śņØæņØ┤ ņŚåļŖö ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉļōżņØś ņłśļź╝ Ļ░Éņåīņŗ£ĒéżļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ņ£╝ļ®░ (RR = 0.76; 95% CI = 0.62-0.94), NNTļŖö 7ļ¬ģņØ┤ņŚłļŗż(95% CI = 4-26) [124]. 3Ļ░£ņØś RCTļź╝ ĒżĒĢ©ĒĢ£ ļæÉ ļ▓łņ¦Ė ļģ╝ļ¼ĖņŚÉņä£ļÅä TCAļŖö ņåīĒÖöļČłļ¤ē ņ”ØņāüņØä ņżäņØ┤ļŖö ļŹ░ ĒÜ©Ļ│╝ņĀüņØĖ Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ņ£╝ļ®░(RR 0.74, 95% CI 0.61-0.91), NNTļŖö 6ļ¬ģņØ┤ņŚłļŗż(95% CI 6-18) [125]. ņĀĆņ×ÉļōżņØĆ ņ£äņØś ņŻ╝ņĀ£ņÖĆ Ļ┤ĆļĀ©ĒĢśņŚ¼ ņØ┤ņĀä ļ¼ĖĒŚīĻ│Āņ░░ņŚÉņä£ļŖö ĒżĒĢ©ļÉśņ¦Ć ņĢŖņĢśļŹś 1Ļ░£ņØś RCT [126]ļź╝ ĒżĒĢ©ĒĢśņŚ¼ ņ▓┤Ļ│äņĀü ļ¼ĖĒŚīĻ│Āņ░░Ļ│╝ ļ®öĒāĆļČäņäØņØä ĒĢśņśĆļŗż. ĻĘĖ Ļ▓░Ļ│╝, TCAļŖö ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉļōżņØś ņ”Øņāü ĒśĖņĀäņŚÉ ĒÜ©Ļ│╝ņĀüņØ┤ņŚłļŗż(RR = 0.78, 95% CI = 0.64-0.93, p= 0.008) (Fig. 6). ĻĘĖļ”¼Ļ│Ā TCAņØś ņé¼ņÜ®ņ£╝ļĪ£ ņØĖĒĢ┤ ļČĆņ×æņÜ®ņØ┤ ļ░£ņāØĒĢĀ ĒÖĢļźĀņØĆ ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ļåÆņ¦Ć ņĢŖņØĆ Ļ▓āņØä ĒÖĢņØĖĒĢśņśĆļŗż(RR = 1.56, 95% CI = 0.88-2.76, p= 0.13)(Fig. 7).
ņĢäņŗ£ņĢäņŚÉņä£ ņŗ£Ē¢ēļÉ£ ņŚ░ĻĄ¼ļōżļĪ£ļŖö ļČłņØæņä▒ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉļōżņØä ļīĆņāüņ£╝ļĪ£ TCAņÖĆ ņ£äņĢĮņØś ĒÜ©Ļ│╝ļź╝ ļ╣äĻĄÉĒĢ£ 2Ļ░£ņØś RCTĻ░Ć ņ׳ņŚłļŗż[126,127]. ņ▓½ ļ▓łņ¦Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö imipramineĻ│╝ ņ£äņĢĮņØä 12ņŻ╝Ļ░ä Ēł¼ņŚ¼ĒĢśņŚ¼ imipramineņØ┤ ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ņåīĒÖöļČłļ¤ē ņ”ØņāüņØś Ļ░£ņäĀņŚÉ ĒÜ©Ļ│╝Ļ░Ć ņ׳ņØīņØä ĒÖĢņØĖĒĢśņśĆļŗż[126]. NortriptylineĻ│╝ ņ£äņĢĮņØä 8ņŻ╝ ļÅÖņĢł Ēł¼ņŚ¼ĒĢ£ ļśÉ ļŗżļźĖ ņŚ░ĻĄ¼ņŚÉņä£ļŖö nortriptylineņØ┤ ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ņåīĒÖöļČłļ¤ē ņ”ØņāüņØä Ļ░Éņåīņŗ£Ēé┤ņØä ņ”Øļ¬ģĒĢśņ¦Ć ļ¬╗ĒĢśņśĆļŗż[127]. Talley ļō▒[128]ņØĆ TCAĻ░Ć PDS ņ”ØņāüņØ┤ ņ׳ļŖö ĒÖśņ×Éļōż ļ│┤ļŗżļŖö ņåīĒÖöņä▒ ĻČżņ¢æņØś ņ”ØņāüĻ│╝ Ļ░ÖņØĆ EPS ĒÖśņ×ÉļōżņŚÉņä£ ļŹö ĒÜ©Ļ│╝ņĀüņ×äņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż. ņÜöņĢĮĒĢśļ®┤, TCAļŖö ĻĖ░ņĪ┤ņØś ņ╣śļŻīņŚÉ ļ░śņØæņØ┤ ņŚåļŖö ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ ņ╣śļŻī ĒÜ©Ļ│╝ļź╝ ĻĖ░ļīĆĒĢĀ ņłś ņ׳ņ£╝ļ®░, ĒŖ╣Ē׳ EPS ņĢäĒśĢņØś ĒÖśņ×ÉļōżņŚÉĻ▓ī ļŹöņÜ▒ ĒÜ©Ļ│╝ņĀüņØ╝ Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż. ļ╣äļĪØ ņØ┤ ņŚ░ĻĄ¼ņŚÉņä£ļŖö TCAņØś ļČĆņ×æņÜ®ņØ┤ ņ£äņĢĮĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ĒåĄĻ│äņĀüņØĖ ņ░©ņØ┤Ļ░Ć ņŚåņŚłņ£╝ļéś, ņ×äņāüņŚÉņä£ TCAļź╝ ņé¼ņÜ®ĒĢĀ ļĢīņŚÉļŖö ņĢĮļ¼╝ ļČĆņ×æņÜ®ņŚÉ ļīĆĒĢ£ ņŻ╝ņØśļź╝ ĻĖ░ņÜĖņŚ¼ņĢ╝ ĒĢ£ļŗż.
ĻĖ░ĒāĆ ņĢĮņĀ£
17Ļ░£ņØś RCTņŚÉ ļīĆĒĢ£ ļ®öĒāĆļČäņäØņŚÉņä£, rebamipideļŖö ņ£äņĢĮ ļśÉļŖö ļīĆņĪ░ĻĄ░Ļ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ņåīĒÖöļČłļ¤ē ņ”ØņāüņØä 23% Ļ░£ņäĀĒĢśņśĆļŗż. ĒŖ╣Ē׳ ĻĖ░ņ¦łņĀüņØĖ ņøÉņØĖņØś ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉņØś Ļ▓ĮņÜ░ ņ”ØņāüņØ┤ 28% Ļ░ÉņåīĒĢśņŚ¼ ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢśņśĆņ¦Ćļ¦ī ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉļŖö ņ£ĀņØśĒĢ£ Ļ░£ņäĀņØ┤ ņŚåņŚłļŗż[129]. SucralfateļŖö ņĀ£ņé░ņĀ£ļĪ£, ļ╣äĻČżņ¢æņä▒ ņåīĒÖöļČłļ¤ē ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ 2Ļ░£ņØś ņ£äņĢĮ ļīĆņĪ░ĻĄ░ ņŚ░ĻĄ¼Ļ░Ć ņ׳ļŗż.ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ 3ņŻ╝ ļÅÖņĢłņØś sucralfateļŖö ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ņ”Øņāü Ļ░£ņäĀņŚÉ ĒÜ©Ļ│╝ņĀüņØ┤ņ¦Ć ļ¬╗ĒĢśņśĆļŗż[130]. ļ░śļ®┤ ļŗżļźĖ ņŚ░ĻĄ¼ņŚÉņä£4ņŻ╝ ļÅÖņĢł sucralfate ļ│ĄņÜ®ņØĆ ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ņØśļ»Ė ņ׳ļŖö ņ”Øņāü Ļ░£ņäĀņØä ļ│┤ņśĆļŗż[131]. 2Ļ░£ņØś ņŚ░ĻĄ¼ļź╝ ņóģĒĢ®ĒĢ£ ļČäņäØņŚÉņä£ sucralfateĻ░Ć ņ”ØņāüņØä ĒśĖņĀäņŗ£ņ╝░ņ¦Ćļ¦ī ĒåĄĻ│äņĀüņ£╝ļĪ£ ņØśļ»ĖļŖö ņŚåņŚłļŗż[132].
SimethiconeņŚÉ ļīĆĒĢ£ 2Ļ░£ņØś ņŚ░ĻĄ¼Ļ░Ć ņ׳ļŗż. Simethicone (80 mg 1ņØ╝ 3ĒÜī)Ļ│╝ cisapride (10 mg 1ņØ╝ 3ĒÜī)ļź╝ ļ¼┤ņ×æņ£äļĪ£ ļ╣äĻĄÉĒĢ£ Ļ▓░Ļ│╝ simethiconeņØĆ cisaprideļ│┤ļŗż 2ņŻ╝ņÖĆ 4ņŻ╝ņŚÉ ļ│ĄļČĆĒīĮļ¦ī ņ”ØņāüņŚÉ ļŹö ĒÜ©Ļ│╝ņĀüņØ┤ņŚłĻ│Ā, ņŚŁļźś ņ”ØņāüņØĆ 2ņŻ╝ņŚÉļ¦ī ĒÜ©Ļ│╝ņĀüņØ┤ņŚłļŗż[133]. ņØ┤ ņŚ░ĻĄ¼ņŚÉ ĻĘ╝Ļ▒░ĒĢśņŚ¼ 8ņŻ╝ ļÅÖņĢł ņĢĮņĀ£ļź╝ Ēł¼ņŚ¼ĒĢśĻ│Ā ņ”Øņāü ļ│ĆĒÖöļź╝ ĒÖĢņØĖĒĢśļŖö ņ£äņĢĮ ļīĆņĪ░ ņŚ░ĻĄ¼Ļ░Ć ņŗ£Ē¢ēļÉśņŚłļŗż[134]. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ simethiconeĻ│╝ cisaprideļŖö ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ņ”ØņāüņØä Ļ░£ņäĀņŗ£ņ╝░ņ£╝ļ®░, ĒŖ╣Ē׳ simethiconeņØĆ cisaprideņÖĆ ļ╣äĻĄÉĒĢśņŚ¼ ņ▓½ 2ņŻ╝ ļÅÖņĢł ņ”ØņāüĻ░£ņäĀ ĒÜ©Ļ│╝Ļ░Ć ļŹö ņÜ░ņłśĒĢśņśĆļŗż. SimethiconeņØ┤ ņåīĒÖöļČłļ¤ēņŚÉ ņ×æņÜ®ĒĢśļŖö ĻĖ░ņĀäņØĆ ņĀĢĒÖĢĒ׳ ņĢīļĀżņĀĖ ņ׳ņ¦ĆļŖö ņĢŖņ£╝ļéś, simethiconeņØ┤ ņןņŚÉņä£ ĒØĪņłśļÉśņ¦Ć ņĢŖĻ│Ā, ņןļé┤ Ļ░ĆņŖżļź╝ Ļ░Éņåīņŗ£Ēéżļ»ĆļĪ£ ļé┤ņןĒåĄĻ░üĻ│╝ļ»╝(visceral hyperalgesia)Ļ│╝ Ļ┤ĆļĀ©ļÉ£ Ļ░ĆņŖżĒīĮņ░ĮņŚÉ ĒÜ©Ļ│╝ņĀüņ£╝ļĪ£ ņ×æņÜ®ĒĢĀ Ļ▓āņ£╝ļĪ£ ņāØĻ░üĒĢ£ļŗż.
ņĀĢņŗĀ ņ╣śļŻī
13. ņĀĢņŗĀ ņ╣śļŻīļŖö ņĢĮļ¼╝ ņ╣śļŻīņŚÉ ļ░śņØæņØ┤ ņŚåļŖö ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņØś ņ”Øņāü ĒśĖņĀäņŚÉ ļÅäņøĆņØä ņŻ╝ļ»ĆļĪ£ ĻČīĻ│ĀĒĢĀ ņłś ņ׳ļŗż.
ŌĆó ĻČīĻ│Ā ļō▒ĻĖē: ņĢĮĒĢ©
ŌĆó ņ”ØĻ▒░ ņłśņżĆ: ņżæļō▒ļÅä
ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉļŖö ņ”ØņāüņØ┤ ņŚåļŖö Ļ▓ĮņÜ░ļ│┤ļŗż ļČłņĢł, ņÜ░ņÜĖ, ņŗ¼ļ”¼ņĀü ņŖżĒŖĖļĀłņŖżņÖĆ Ļ░ÖņØĆ ņĀĢņŗĀņĀü ļ¼ĖņĀ£ļź╝ ļŹö ļ¦ÄņØ┤ Ļ░Ćņ¦ĆĻ│Ā ņ׳ļŗż[135]. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉņŚÉ ļīĆĒĢ£ ņĀĢņŗĀ ņ╣śļŻīņŚÉļŖö ļÅÖņĀü ņĀĢņŗĀ ņ╣śļŻī(dynamic psychotherapy), ņĄ£ļ®┤ ņ╣śļŻī(hypnotherapy), Ē¢ēļÅÖ ņ╣śļŻī(behavioral treatments)ņÖĆ ņØĖņ¦Ć-Ē¢ēļÅÖ ņ╣śļŻī(cognitive-behavioral therapy)Ļ░Ć ĒżĒĢ©ļÉ£ļŗż[136-138]. ņĄ£ļ®┤ ņ╣śļŻīĻ░Ć ņØ╝ļ░ś ņ╣śļŻīņŚÉ ļ╣äĒĢ┤ ĒÜ©Ļ│╝ņĀüņØ┤ļØ╝ļŖö 1Ļ░£ņØś ņŚ░ĻĄ¼Ļ░Ć ņ׳ņ¦Ćļ¦ī, ņ▓┤Ļ│äņĀü ļ¼ĖĒŚīĻ│Āņ░░ņŚÉņä£ļŖö ļ╣äĻČżņ¢æņä▒ ņåīĒÖöļČłļ¤ēņŚÉ ļīĆĒĢ£ ņĀĢņŗĀ ņ╣śļŻīņØś ĒÜ©Ļ│╝Ļ░Ć ņ×ģņ”ØļÉśņ¦Ć ņĢŖņĢśļŗż[136,139].
ĒĢ£ RCT ņŚ░ĻĄ¼ņŚÉņä£ ņĀĢņŗĀ ņ╣śļŻīņÖĆ ĒĢ©Ļ╗ś 4Ļ░£ņøö ļÅÖņĢł Ļ░ĢĒÖöļÉ£ ņ╣śļŻī(ņÜ┤ļÅÖĻ│╝ Ļ░ÉĻ░ü ĻĖ░ļŖźņØś ņØ┤ņāüņŚÉ ļīĆĒĢ┤ Ļ▓Ćņé¼ĒĢśĻ│Ā ņØ┤ļź╝ ļ¬®Ēæ£ļĪ£ ņäżņĀĢĒĢśņŚ¼ ņĢĮļ¼╝ ņ╣śļŻī)ļź╝ ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØ┤ ĻĖ░ņĪ┤ ņ╣śļŻīņŚÉ ļ░śņØæĒĢśņ¦Ć ņĢŖļŖö ņåīĒÖöļČłļ¤ē ņ”ØņāüņØä ĒÜ©Ļ│╝ņĀüņ£╝ļĪ£ Ļ░Éņåīņŗ£ņ╝░ļŗż. ņČöĻ░ĆņĀüņØĖ ņØĖņ¦Ć-Ē¢ēļÅÖ ņ╣śļŻīļŖö ļÅÖļ░śļÉ£ ļČłņĢłĻ│╝ ņÜ░ņÜĖ ņ”ØņāüņØä ņĪ░ņĀłĒĢśļŖö ļŹ░ ĒÜ©Ļ│╝ņĀüņØ╝ ņłś ņ׳Ļ▓Āļŗż[140]. ļŗżļźĖ ļ¼┤ņ×æņ£ä ļīĆņĪ░ĻĄ░ ņŚ░ĻĄ¼ņŚÉņä£ļŖö 10ņŻ╝ļÅÖņĢł ņĢĮļ¼╝ ņ╣śļŻīņÖĆ ĒĢ©Ļ╗ś ņĀĢņŗĀ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØ┤ ņĢĮļ¼╝ ņ╣śļŻīļ¦ī ņŗ£Ē¢ēĒĢśļŖö Ļ▓ĮņÜ░ļ│┤ļŗż ņåīĒÖöļČłļ¤ē ņ”ØņāüĻ│╝ ņØ┤ņÖĆ ņŚ░Ļ┤ĆļÉ£ ņéČņØś ņ¦łņØä ĒśĖņĀäņŗ£ĒéżļŖö ļŹ░ ĒÜ©Ļ│╝ņĀüņØ┤ņŚłļŗż[141].
ņĄ£ĻĘ╝ ņ▓┤Ļ│äņĀü ļ¼ĖĒŚīĻ│Āņ░░ņŚÉņä£ļŖö ņĀĢņŗĀ ņ╣śļŻīĻ░Ć ņåīĒÖöļČłļ¤ē ņ”ØņāüņØä ņØśļ»Ė ņ׳Ļ▓ī ĒśĖņĀäņŗ£ĒéżļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż(RR = 0.53, 95% CI = 0.44-0.65, NNT 3). ņØ┤ Ļ│Āņ░░ņØĆ 789ļ¬ģņØś ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉņØś ņ”Øņāü Ļ░£ņäĀņØä ņØ┤ļČäļ▓Ģņ£╝ļĪ£ ĻĖ░ņłĀĒĢ£ ņŚ░ĻĄ¼ļōżņØä ĒżĒĢ©ĒĢśņśĆļŗż[17]. ņĀĢņŗĀ ņ╣śļŻīņØś Ļ▓░Ļ│╝ļŖö ņłśļ®┤ņØś ņ¦łņØ┤ ļéśņüśĻ▒░ļéś(OR = 7.68, 95% CI = 1.83-32.25) Ļ▓░Ēś╝ ņāüĒā£Ļ░Ć ņøÉĒÖ£ĒĢśņ¦Ć ļ¬╗ĒĢ£ Ļ▓ĮņÜ░(OR = 1.22, 95% CI = 1.10-1.36)ņÖĆ ļČĆņĀĢņĀüņØĖ ņŚ░Ļ┤Ćņä▒ņØä ļ│┤ņśĆĻ│Ā, ņÖĖĒ¢źņĀüņØĖ ņä▒Ļ▓®ņØä ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░(OR = 0.86, 95% CI = 0.76-0.96)ņÖĆļŖö ĻĖŹņĀĢņĀüņØĖ ņŚ░Ļ┤Ćņä▒ņØä ļéśĒāĆļāłļŗż[142]. ņØ┤ļ¤¼ĒĢ£ Ļ▓░Ļ│╝ļōżņØä Ļ│ĀļĀżĒĢśļ®┤ ņĀĢņŗĀ ņ╣śļŻīļŖö ņĢĮļ¼╝ ņ╣śļŻīņŚÉ ļ░śņØæĒĢśņ¦Ć ņĢŖĻ│Ā, ĒŖ╣Ē׳ ņĀĢņŗĀņĀü ņÜöņØĖĻ│╝ ņŚ░Ļ┤ĆļÉśņ¢┤ ļéśĒāĆļéĀ ņłś ņ׳ļŖö ņŗ¼ĒĢ£ ņ”ØņāüņØä ļ│┤ņØ┤ļŖö ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉņØś ņ╣śļŻīņŚÉ Ļ│ĀļĀżļÉĀ ņłś ņ׳Ļ▓Āļŗż.
ņŗØņØ┤
14. Ļ│Āņ¦Ćļ░®ņŗØņØä Ēö╝ĒĢśļŖö ļō▒ ņŗØņØ┤ ņĪ░ņĀłņØĆ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ņ”Øņāü ĒśĖņĀäņŚÉ ļÅäņøĆņØä ņŻ╝ļ»ĆļĪ£ ĻČīĻ│ĀĒĢĀ ņłś ņ׳ļŗż.
ŌĆó ĻČīĻ│Ā ļō▒ĻĖē: ņĢĮĒĢ©
ŌĆó ņ”ØĻ▒░ ņłśņżĆ: ļé«ņØī
ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņŚÉņä£ ņŗØņØ┤ ņĪ░ņĀłņØĆ ņżæņÜöĒĢ£ ņŚŁĒĢĀņØä ĒĢĀ Ļ▓āņ£╝ļĪ£ ĻĖ░ļīĆļÉ£ļŗż. ĻĘĖļ¤¼ļéś ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņŚÉņä£ ņØīņŗØĻ│╝ņØś ņŚ░Ļ┤Ćņä▒ņŚÉ ļīĆĒĢ£ ļ¼ĖĒŚīņ×ÉļŻīļŖö ņĢäņ¦ü ļČĆņĪ▒ĒĢśĻ│Ā ņØ╝ņ╣śļÉśņ¦Ć ņĢŖļŖö Ļ▓░Ļ│╝ļź╝ ļ│┤ņØĖļŗż. ņØ╝ļ░śņĀüņ£╝ļĪ£ ņåīĒÖöļČłļ¤ē ņ”ØņāüņØä ņ£Āļ░£ĒĢśļŖö ņØīņŗØņØĆ Ēö╝ĒĢśļŖö Ļ▓āņØ┤ ņóŗļŗż. ĒŖ╣Ē׳ Ļ│Āņ¦Ćļ░®ņŗØņØ┤ļŖö ņåīĒÖöļČłļ¤ē ņ”ØņāüņØä ņ£Āļ░£ĒĢśĻ▒░ļéś ņĢģĒÖöņŗ£Ēé¼ ņłś ņ׳ļŗż. ņŗŁņØ┤ņ¦Ćņןļé┤ ņ¦Ćļ░®ņØĆ ņ£ä ĒīĮņ░ĮņŚÉ ļīĆĒĢ£ ņśłļ»╝ļÅäļź╝ ņ”ØĻ░Ćņŗ£ņ╝£ ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉņŚÉņä£ ļ│ĄļČĆ ĒīĮļ¦īĻ│╝ ļČłĒÄĖĻ░ÉņØä ņ£Āļ░£ĒĢ£ļŗż[143]. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ ņŗØĒøä Ēżļ¦īĻ░ÉņØ┤ļéś ĒīĮļ¦īĻ░ÉņØĆ Ļ│Āņ¦Ćļ░®ņŗØņØ┤ņÖĆ ņ¦üņĀæņĀüņØĖ ņŚ░Ļ┤Ćņä▒ņØä ļ│┤ņØĖļŗż[144]. ļśÉĒĢ£ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉņä£ Ļ│Āņ¦Ćļ░®ņŗØņØ┤ļŖö Ļ▒┤Ļ░ĢĒĢ£ ņé¼ļ×īņŚÉ ļ╣äĒĢ┤ ĻĄ¼ņŚŁĻ│╝ ļ│ĄĒåĄņØä ņ£Āļ░£ĒĢśņśĆļŗż[145]. ņÜ░ņ£Ā, ņ£ĀņĀ£ĒÆł, ļ░ĆĻ░ĆļŻ© ņØīņŗØ, ļ¦żņÜ┤ ņØīņŗØļÅä ņåīĒÖöļČłļ¤ē ņ”ØņāüņØä ņØ╝ņ£╝Ēé¼ ņłś ņ׳ņ£╝ļ®░[146,147], Ēāäņé░ ņØīļŻīļéś ņ╗żĒö╝ļÅä ņ”ØņāüņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ļŗż[147,148].
Ļ▓░ ļĪĀ
40ņäĖ ņØ┤ņāüņØś ņåīĒÖöļČłļ¤ē ĒÖśņ×ÉņŚÉņä£ ĻĖ░ņ¦łņĀü ņøÉņØĖ, ĒŖ╣Ē׳ ņ£äņĢöņØä ļ░░ņĀ£ĒĢśĻĖ░ ņ£äĒĢ┤ ņāüļČĆņ£äņןĻ┤Ć ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢ┤ņĢ╝ ĒĢ£ļŗż. ĻĖ░ņ¦łņĀü ņøÉņØĖņØä ļ░░ņĀ£ĒĢ£ ĒøäņŚÉ ņ”ØņāüņØ┤ ļ¦īņä▒ņØ┤Ļ▒░ļéś ļ░śļ│ĄļÉśļŖö Ļ▓ĮņÜ░, ņ”ØņāüņŚÉ ļö░ļØ╝ EPS ņĢäĒśĢĻ│╝ PDS ņĢäĒśĢņ£╝ļĪ£ ĻĄ¼ļČäĒĢśņŚ¼ ņ╣śļŻīĒĢ£ļŗż. EPS ņĢäĒśĢņØś ĒÖśņ×ÉļōżņØĆ ņÜ░ņäĀ PPIļĪ£ ņ╣śļŻīĒĢ£ļŗż. PDS ņĢäĒśĢņØś ĒÖśņ×ÉļōżņØĆ ļÅäĒīīļ»╝ D2 ņłśņÜ®ņ▓┤ ĻĖĖĒĢŁņĀ£ņÖĆ 5-HT4 ņłśņÜ®ņ▓┤ ņ×æņÜ®ņĀ£ņÖĆ Ļ░ÖņØĆ ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£ļź╝ ņé¼ņÜ®ĒĢ£ļŗż. ņØ╝ļČĆ ļÅäĒīīļ»╝ D2 ņłśņÜ®ņ▓┤ ĻĖĖĒĢŁņĀ£ļŖö ņןĻĖ░Ļ░ä ņé¼ņÜ®ĒĢśļŖö ļÅÖņĢł ļČĆņ×æņÜ®ņØä ņØ╝ņ£╝Ēé¼ ņłś ņ׳ņ£╝ļ»ĆļĪ£ ņŻ╝ņØśĒĢ┤ņä£ ņé¼ņÜ®ĒĢ┤ņĢ╝ ĒĢ£ļŗż. H. pylori ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ļīĆĒĢ£ ļ®öĒāĆļČäņäØņØĆ ņåīĒÖöļČłļ¤ē ņ”ØņāüņØ┤ ņןĻĖ░ņĀüņ£╝ļĪ£ ĒśĖņĀäļÉśļŖö ĒÜ©Ļ│╝ļź╝ ļ│┤ņŚ¼ņż¼ņ¦Ćļ¦ī, ļÅÖņ¢æņØĖņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ĻĘĖ ĒÜ©Ļ│╝Ļ░Ć ļČłļČäļ¬ģĒĢśņŚ¼ ĻĄŁļé┤ņŚÉņä£ RCT ņŚ░ĻĄ¼Ļ░Ć ĒĢäņÜöĒĢśļŗż. H. pylori ņĀ£ĻĘĀ ņ╣śļŻīļŖö PPIņÖĆ ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£Ļ░Ć ĒÜ©Ļ│╝ņĀüņØ┤ņ¦Ć ņĢŖņØĆ Ļ▓ĮņÜ░ ļśÉļŖö ļ¦īņä▒ ņåīĒÖöļČłļ¤ē ņ”ØņāüņØ┤ ņ׳ļŖö ņĀŖņØĆ ĒÖśņ×ÉņŚÉĻ▓ī ņĀüņÜ®ĒĢĀ ņłś ņ׳ļŗż. TCAļŖö ņé░ļČäļ╣äņ¢ĄņĀ£ņĀ£ļéś ņ£äņןĻ┤Ć ņÜ┤ļÅÖņ┤ēņ¦äņĀ£ ļō▒ņŚÉ ļ░śņØæņØ┤ ņŚåņØä ļĢī ņé¼ņÜ®ĒĢśņŚ¼ ļ│╝ ņłś ņ׳Ļ│Ā ņ”Øņāü ĒśĖņĀäņŚÉ ĒÜ©Ļ│╝ņĀüņØ┤ļŗż. ļśÉĒĢ£ ņ”ØņāüņØś ņ×¼ļ░£ņØä Ēö╝ĒĢśĻĖ░ ņ£äĒĢ┤ ņĢĮļ¼╝ ņ╣śļŻīļ┐É ņĢäļŗłļØ╝ ņŗØņØ┤ ņĪ░ņĀłņØ┤ļéś ņŖżĒŖĖļĀłņŖż Ļ┤Ćļ”¼Ļ░Ć ņżæņÜöĒĢśĻ│Ā ļ¼┤ņŚćļ│┤ļŗż ĒÖśņ×ÉņŚÉĻ▓ī ņ¦łļ│æņØś ĒŖ╣ņä▒ņØä ĻĄÉņ£ĪĒĢśņŚ¼ ņĢłņŗ¼ņŗ£ĒéżĻ│Ā ņ¦łļ│æņØä ņØ┤ĒĢ┤ĒĢśļÅäļĪØ ĒĢśļŖö Ļ▓ā(reassurance)ņØ┤ ņżæņÜöĒĢśļŗż.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






