


ņä£ ļĪĀ
ļ¦īņä▒ ņŗĀņ¦łĒÖśņØĆ ļŗ╣ļć©ļ│æ ļśÉļŖö Ļ│ĀĒśłņĢĢĻ│╝ Ļ░ÖņØĆ ļ¦īņä▒ ņ¦łĒÖśņŚÉņä£ ņŻ╝ļĪ£ ĻĖ░ņØĖĒĢśļ®░, ĻĄŁļé┤ņŚÉņä£ļŖö ļ¦ÉĻĖ░ ņŗĀņ¦łĒÖśņ£╝ļĪ£ ņ¦äĒ¢ēĒĢśņŚ¼ ņŗĀļīĆņ▓┤ņÜöļ▓ĢņØä ļ░øļŖö ĒÖśņ×É ņżæ ļŗ╣ļć©ļ│æņŚÉ ņØśĒĢ£ ļ╣äņ£©ņØ┤ 2010ļģä ņØ┤Ēøä ĻĖēĻ▓®ĒĢśĻ▓ī ņ”ØĻ░ĆĒĢśņŚ¼ Ēśäņ×¼ ļŗ╣ļć©ļ│æņØ┤ Ļ░Ćņן ĒØöĒĢ£ ņøÉņØĖ ņ¦łĒÖśņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[1]. ĒĢ£ĒÄĖ ļ¦īņä▒ ņŗĀņ¦łĒÖśņØĆ ļ¦ÉĻĖ░ ņŗĀļČĆņĀäņ£╝ļĪ£ņØś ņ¦äĒ¢ē, ņŗ¼ĒśłĻ┤Ć ņ¦łĒÖś ļ░£ņāØ ļ░Å ļåÆņØĆ ņé¼ļ¦ØļźĀĻ│╝ļÅä ņŚ░Ļ┤ĆļÉśņ¢┤ ņ׳ļŗż. Ēśäņ×¼Ļ╣īņ¦Ć ļ¦īņä▒ ņŗĀņ¦łĒÖśņØś ņĀüņĀłĒĢ£ ņ╣śļŻī ļ░Å Ļ┤Ćļ”¼ļĪ£ļŖö, ņĢīļČĆļ»╝ļć©ņØś ņ╣śļŻī(ņĢłņ¦ĆņśżĒģÉņŗĀņłśņÜ®ņ▓┤ņ░©ļŗ©ņĀ£ ļśÉļŖö ņĢłņ¦ĆņśżĒģÉņŗĀņĀäĒÖśĒÜ©ņåīņ¢ĄņĀ£ņĀ£), ņŗ¼ĒśłĻ┤Ć ņ£äĒŚśņØĖņ×ÉņØś ņĪ░ņĀł(ņØ┤ņāüņ¦Ćņ¦łĒśłņ”Ø, Ēśłļŗ╣ ļ░Å ĒśłņĢĢ Ļ┤Ćļ”¼)Ļ│╝ ĒĢ©Ļ╗ś ņ×Āņ×¼ņĀüņ£╝ļĪ£ ņŗĀļÅģņä▒ņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ļŖö ņĢĮņĀ£ņŚÉ ļīĆĒĢ£ ņŻ╝ņØś ļ░Å ņÜ®ļ¤ē ņĪ░ņĀł ļō▒ņØ┤ ņĀ£ņŗ£ļÉśĻ│Ā ņ׳ļŗż[2].
ņĄ£ĻĘ╝ sodium-glucose cotransporter 2 (SGLT2) ņ¢ĄņĀ£ņĀ£ņŚÉ Ļ┤ĆĒĢ£ ļīĆĻĘ£ļ¬© ņŗ¼ĒśłĻ┤Ć ņĢłņĀĢņä▒ ņŚ░ĻĄ¼ņŚÉņä£ Ēśłļŗ╣ Ļ░£ņäĀ ĒÜ©Ļ│╝ļŖö ļ¼╝ļĪĀ ņŗ¼ĒśłĻ┤Ć ņ¦łĒÖś ņé¼Ļ▒┤ ļ░Å ņé¼ļ¦ØļźĀņØä ļé«ņČśļŗżļŖö Ļ▓░Ļ│╝ļź╝ ļ│┤Ļ│ĀĒĢśņśĆļŗż[3-5]. ņØ┤ ņżæņŚÉņä£ canagliflozinĻ│╝ empagliflozinņØä ņØ┤ņÜ®ĒĢ£ ļ¼┤ņ×æņ£äĒÖö ļ╣äĻĄÉ ļīĆņĪ░ ņŚ░ĻĄ¼ņŚÉņä£ ņØ┤ņ░© Ļ▓░Ļ│╝ņ¦ĆĒæ£ļĪ£ņä£ ņŗĀĻĖ░ļŖź ļ│┤ĒśĖ ĒÜ©Ļ│╝ļź╝ ļ│┤ņŚ¼ņŻ╝ņŚłļŖöļŹ░, Ļ░üĻ░üņØś ņŗĀĻĖ░ļŖź ļ│ĄĒĢ® Ļ▓░Ļ│╝ņØś ĻĄ¼ņä▒ņŚÉ ņ׳ņ¢┤ņä£ļŖö ņ░©ņØ┤Ļ░Ć ņ׳ņŚłļŗż. EmpagliflozinņØä ņØ┤ņÜ®ĒĢ£ ņŚ░ĻĄ¼ļŖö ņŗĀĻĖ░ļŖź ņĢģĒÖöņØś ļ░£ņāØ ļśÉļŖö ņ¦äĒ¢ēņØä Ēśäņä▒ ņĢīļČĆļ»╝ļć©(ņåīļ│Ć ņĢīļČĆļ»╝-Ēü¼ļĀłņĢäĒŗ░ļŗī ļ╣äņ£© > 300 mg/dL), Ēśłņ▓Ł Ēü¼ļĀłņĢäĒŗ░ļŗī ņłśņ╣śņØś 2ļ░░ ņāüņŖ╣Ļ│╝ ĒĢ©Ļ╗ś ņśłņāü ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£©(estimated glomerular filtration rate, eGFR)ņØś Ļ░Éņåī(< 45 mL/min/1.73 m2), ņŗĀļīĆņ▓┤ņÜöļ▓ĢņØś ņŗ£ņ×æ ļśÉļŖö ņŗĀņ¦łĒÖśņ£╝ļĪ£ ņØĖĒĢ£ ņé¼ļ¦ØņØä Ļ▓░Ļ│╝ ņ¦ĆĒæ£ļĪ£ ņĀĢņØśĒĢśņśĆĻ│Ā[6], canagliflozinņØä ņØ┤ņÜ®ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņśłņāü ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£©ņØś 40% Ļ░Éņåī, ņŗĀļīĆņ▓┤ņÜöļ▓ĢņØś ņŗ£Ē¢ē ļśÉļŖö ņŗĀņ¦łĒÖśņ£╝ļĪ£ ņØĖĒĢ£ ņé¼ļ¦Øņ£╝ļĪ£ Ļ▓░Ļ│╝ ņ¦ĆĒæ£ļź╝ ņĀĢņØśĒĢśņśĆļŗż[5]. DapagliflozinņØä ņØ┤ņÜ®ĒĢ£ ņŗ¼ĒśłĻ┤Ć ņĢłņĀĢņä▒ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņŗĀĻĖ░ļŖźņŚÉ ļīĆĒĢ£ Ļ▓░Ļ│╝ļŖö ļ│┤Ļ│ĀĒĢśņ¦Ć ņĢŖņĢśļŗż[4]. ĒĢ£ĒÄĖ Ļ░ü ņŚ░ĻĄ¼ņŚÉ ĒżĒĢ©ļÉ£ ĒÖśņ×ÉĻĄ░ņØś ņ×äņāü ņ¢æņāü ļ░Å ņŗĀĻĖ░ļŖź ņāüĒā£Ļ░Ć ļŗżļź┤Ļ│Ā Ļ░ü ņŚ░ĻĄ¼ ļ│äļĪ£ ņČöņĀü Ļ┤Ćņ░░ ĻĖ░Ļ░äņØ┤ ļŗ¼ļØ╝ņä£ SGLT2 ņ¢ĄņĀ£ņĀ£Ļ░Ć ņŗĀĻĖ░ļŖź ņ×Éņ▓┤ņŚÉ ņ¢┤ļ¢ĀĒĢ£ ņśüĒ¢źņØä ļ»Ėņ╣śļŖöņ¦ĆņŚÉ ļīĆĒĢ┤ņä£ļŖö ņĢäņ¦ü Ļ▓░ļĪĀņØä ļé┤ļ”┤ ņłś ņŚåļŗż. ļö░ļØ╝ņä£ ņÜ░ļ”¼ļŖö Ēśäņ×¼ ĻĄŁļé┤ņŚÉņä£ ņĀ£2ĒśĢ ļŗ╣ļć©ļ│æ ĒÖśņ×ÉņŚÉĻ▓ī ņ▓śļ░®ņØ┤ Ļ░ĆļŖźĒĢ£ SGLT2 ņ¢ĄņĀ£ņĀ£ ņżæ ņ£äņĢĮ ļīĆļ╣ä 52ņŻ╝ ņØ┤ņāü ņČöņĀü Ļ┤Ćņ░░ĒĢ£ ļ¼┤ņ×æņ£ä ļīĆņĪ░ĻĄ░ ņŚ░ĻĄ¼(review, case series, single arm study ņĀ£ņÖĖ)ļōżņŚÉņä£ ņןĻĖ░Ļ░ä SGLT2 ņ¢ĄņĀ£ņĀ£ ņ╣śļŻīĻ░Ć ņŗĀņןĻĖ░ļŖźņŚÉ ļ»Ėņ╣śļŖö ĒÜ©Ļ│╝ļź╝ ļ®öĒāĆļČäņäØņØä ĒåĄĒĢ┤ ņĢīņĢäļ│┤Ļ│Āņ×É ĒĢ£ļŗż. ļśÉĒĢ£ ņĀ£2ĒśĢ ļŗ╣ļć©ļ│æ ĒÖśņ×ÉņŚÉņä£ ņןĻĖ░Ļ░ä SGLT2 ņ¢ĄņĀ£ņĀ£ ņé¼ņÜ®ņŚÉ ļö░ļźĖ ņØ┤ļōØĻ│╝ ņ£äĒĢ┤ņØś ĻĘĀĒśĢņØä Ļ│ĀļĀżĒĢśņŚ¼ ĻČīĻ│ĀņĢłņŚÉ ļ░śņśüĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ļ│Ė ļĪĀ
ĒĢĄņŗ¼ ņ¦łļ¼Ė ļ░Å ļ¼ĖĒŚī Ļ▓ĆņāēĻ│╝ ĒÅēĻ░Ć
ŌĆ£ņĀ£2ĒśĢ ļŗ╣ļć©ļ│æņŚÉņä£ ņןĻĖ░Ļ░äņØś SGLT2 ņ¢ĄņĀ£ņĀ£ ņ╣śļŻīļŖö ņŗĀņן ĻĖ░ļŖź Ļ░£ņäĀņŚÉ ļÅäņøĆņØ┤ ļÉśļŖöĻ░Ć?ŌĆØļź╝ ĒĢĄņŗ¼ ņ¦łļ¼Ėņ£╝ļĪ£ ĒĢśņŚ¼ ļ®öĒāĆļČäņäØņØä ņ£äĒĢ┤ ņĀäļ¼Ė ņé¼ņä£ņŚÉ ņØśĒĢ┤ ņ▓┤Ļ│äņĀüņØĖ ļ¼ĖĒŚī Ļ▓ĆņāēņØä ņŗ£Ē¢ēĒĢśņśĆļŗż. ļŹ░ņØ┤Ēä░ļ▓ĀņØ┤ņŖżļŖö PubMed, EMBASE, Cochrane libraryļź╝ ņØ┤ņÜ®ĒĢśņśĆĻ│Ā, 2015ļģä 1ņøö 1ņØ╝ļČĆĒä░ 2020ļģä 3ņøö 31ņØ╝Ļ╣īņ¦Ć ņśüļ¼Ėņ£╝ļĪ£ ļ░£Ēæ£ļÉ£ ļ¼ĖĒŚī ņżæ, ĻĄŁļé┤ņŚÉņä£ ņ▓śļ░® Ļ░ĆļŖźĒĢ£ SGLT2 ņ¢ĄņĀ£ņĀ£(dapagliflozin, empagliflozin, ipragliflozin, ertugliflozin)ļź╝ ņé¼ņÜ®ĒĢ£ ļ¼┤ņ×æņ£ä ļīĆņĪ░ ņ×äņāü ņŚ░ĻĄ¼ ņżæ ņĢĮņĀ£ ņ╣śļŻī ĻĖ░Ļ░äņØ┤ 52ņŻ╝ ņØ┤ņāüņØĖ ņŚ░ĻĄ¼ļ¦īņØä ĒżĒĢ©ĒĢśņśĆļŗż. ļ¼ĖĒŚīĻ│Āņ░░ Ļ▓░Ļ│╝, Ļ▓Ćņāē ņĪ░Ļ▒┤ņŚÉ ļö░ļØ╝ ņ£äņĢĮĻ│╝ ļ╣äĻĄÉļÉ£ ļ¼┤ņ×æņ£ä ļīĆņĪ░ ņ×äņāü ņŚ░ĻĄ¼ņØś Ļ▓░Ļ│╝Ļ░Ć ņ׳ļŖö dapagliflozin, empagliflozinļ¦ī ĒżĒĢ©ĒĢśņśĆĻ│Ā, ļ¼ĖĒŚī Ļ▓ĆņāēĻ│╝ ĒÅēĻ░Ćļź╝ ņ£äĒĢ£ population, intervention, comparator, outcomes (PICO)ļŖö Ēæ£ 1Ļ│╝ Ļ░Öļŗż.
ĻĘ╝Ļ▒░ņłśņżĆ: Ļ░£ļ│ä ņ¦ł ĒÅēĻ░Ć Ļ▓░Ļ│╝ ļ░Å ĒĢĄņŗ¼ ņ¦łļ¼ĖņŚÉ ļīĆĒĢ£ ĻĘ╝Ļ▒░ņłśņżĆ ĒÅēĻ░ĆņÖĆ ĻĘ╝Ļ▒░ņØś Ļ░ĢļÅäņÖĆ ĒĢ£Ļ│ä
ņØ┤ļōØņŚÉ Ļ┤ĆĒĢ£ 10Ļ░£ņØś ļ¼┤ņ×æņ£ä ļīĆņĪ░ ņ×äņāü ņŚ░ĻĄ¼ ņżæ 14Ļ░£ ļģ╝ļ¼Ė[4,6-18]ņØä ļČäņäØĒĢśĻ│Ā ļÅģļ”ĮļÉ£ 2ņØĖņØ┤ ĒÅēĻ░ĆĒĢśņśĆļŗż. Ļ░üĻ░üņØś ņŚ░ĻĄ¼ļōżņØĆ ļ╣äļÜżļ”╝ņŚÉ ļīĆĒĢ┤ņä£ļŖö ņżæĻ░ä Ēś╣ņØĆ ļåÆņØĆ ņ¦łļĪ£ ņל Ļ│äĒÜŹļÉśņŚłļŗżĻ│Ā ĒÅēĻ░ĆĒĢśņśĆņ£╝ļéś(Supplementary Fig. 1), ĒĢĄņŗ¼ ņ¦łļ¼ĖņØś ĻĘ╝Ļ▒░ņłśņżĆ(level of evidence) ĒÅēĻ░ĆņŚÉņä£ļŖö ļŗżņØīņØś ļæÉ Ļ░Ćņ¦Ć ņØ┤ņ£ĀļĪ£ ĒĢśĒ¢źņĪ░ņĀĢĒĢśņśĆļŗż.
1. ĻĘ╝Ļ▒░ņØś ņ¦üņĀæņä▒: ļīĆļČĆļČäņØś ņŚ░ĻĄ¼ņŚÉņä£ ņä£ņ¢æņØĖņØä ņŻ╝ ļīĆņāüņ×ÉļĪ£ ĒĢśņśĆĻ│Ā, ņŚ░ĻĄ¼ļ¦łļŗż ņĢäņŗ£ņĢäņØĖņØś ļ╣äņ£©ņØ┤ ļŗżņ¢æĒĢśņśĆņ£╝ļ®░, ņØ╝ļČĆņŚÉņä£ļŖö ņŗ¼ĒśłĻ┤Ć ņ¦łĒÖśņØä Ļ░Ćņ¦ä ļīĆņāüņ×Éļ¦ī ĒżĒĢ©ĒĢśļŖö ļō▒ ņŚ░ĻĄ¼ ļīĆņāü ņ¦æļŗ©ņØ┤ ļÅÖņØ╝ĒĢśņ¦Ć ņĢŖņĢśļŗż. ļśÉĒĢ£ ļīĆņāüņ×ÉņØś ĒÅēĻĘĀ ņ▓┤ņ¦łļ¤ēņ¦ĆņłśļŖö 30 kg/m2 ņĀĢļÅäļĪ£ ņÜ░ļ”¼ļéśļØ╝ ĒÖśņ×ÉļōżņØś ĒŖ╣ņä▒Ļ│╝ļŖö ņ░©ņØ┤Ļ░Ć ņ׳ņŚłļŗż. ņĢäņŗ£ņĢäņØĖņØś ļ╣äņ£©ņØ┤ 40% ņØ┤ņāüņØĖ 4Ļ░£ ņŚ░ĻĄ¼ļ¦īņØä ļČäņäØĒĢśļ®┤ SGLT2 ņ¢ĄņĀ£ņĀ£ņØś ņŗĀĻĖ░ļŖź ļ│┤ĒśĖ ĒÜ©Ļ│╝ļŖö ņżäņ¢┤ļōżņŚłļŗż.
2. ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ņØś ņĀĢļ░Ćņä▒: ĒÅēĻ░ĆņŚÉ ĒżĒĢ©ļÉ£ ņŚ░ĻĄ¼ļōżņØĆ ļ¼┤ņ×æņ£ä ļ░░ņĀĢĻ│╝ ļłłĻ░Ćļ”╝(blinding)ņØ┤ ņל ņ£Āņ¦ĆļÉśņŚłņ£╝ļéś, ņČöņĀü Ļ┤Ćņ░░ ĻĖ░Ļ░ä ļÅÖņĢł ĒāłļØĮņØ┤ ļ¦ÄņĢśļŗż. ņØ╝ļČĆ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ļō▒ļĪØļÉ£ ĒÖśņ×ÉņØś 20% ņĀĢļÅäļ¦ī ņóģļŻī ļĢīĻ╣īņ¦Ć ņČöņĀüļÉśņŚłĻ│Ā, ņ¢┤ļ¢ż ļīĆņāüņ×ÉĻ░Ć ĒāłļØĮĒĢśņśĆļŖöņ¦Ć ĻĘĖļ”¼Ļ│Ā ĒāłļØĮĒĢ£ ļīĆņāüņ×ÉļōżĻ│╝ ĻĘĖļĀćņ¦Ć ņĢŖņØĆ ļīĆņāüņ×Éļōż Ļ░äņŚÉ ņ░©ņØ┤Ļ░Ć ņ׳ļŖöņ¦Ć ņĢī ņłś ņŚåņŚłļŗż. ņ”ē, ļīĆņāüņ×ÉļōżņØś ĒāłļØĮļźĀņØ┤ ļåÆņĢä ņןĻĖ░Ļ░ä ņČöņĀü Ļ┤Ćņ░░ļÉ£ ļīĆņāüņ×ÉļōżņØś Ļ▓░Ļ│╝Ļ░Ć ņĀäņ▓┤ ļīĆņāüņ×ÉļōżņØś Ļ▓░Ļ│╝ļź╝ ļÆĘļ░øņ╣©ĒĢśļŖö ņČ®ļČäĒĢ£ ņĀĢļ│┤(ņé¼Ļ▒┤ņłś)ļØ╝Ļ│Ā ļ│┤ĻĖ░ ņ¢┤ļĀżņøĀļŗż. ļö░ļØ╝ņä£ ĻĘ╝Ļ▒░ņłśņżĆņØä ŌĆ£ļé«ņØī(low evidence)ŌĆØņ£╝ļĪ£ ĒÅēĻ░ĆĒĢśņśĆļŗż.
ņØ┤ļōØ(ĒÄĖņØĄ)
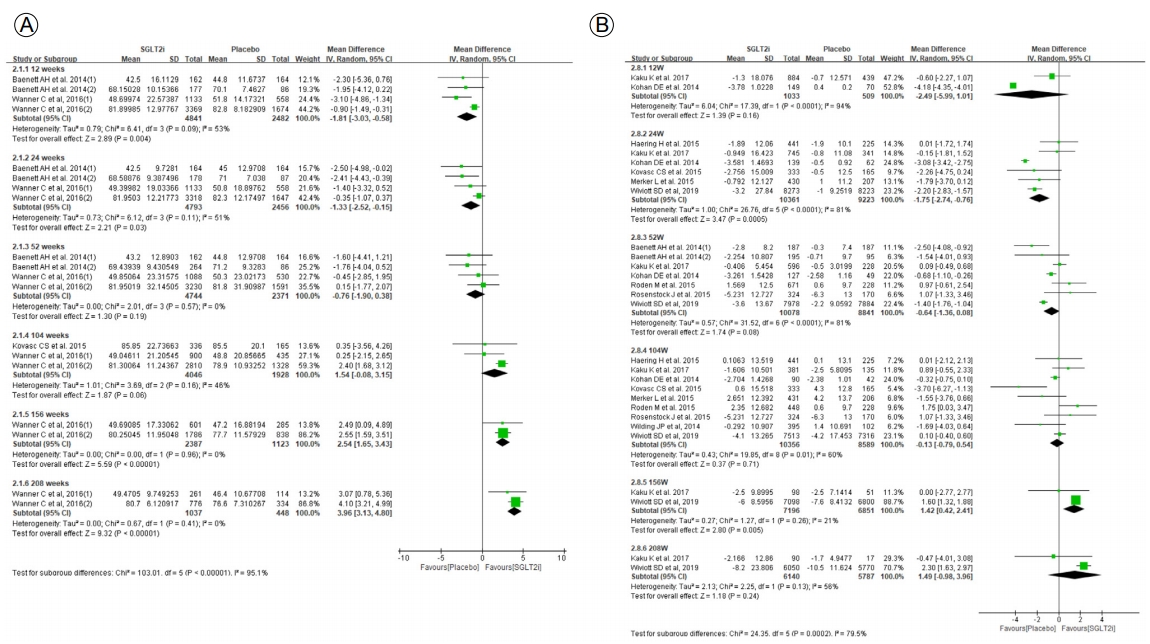
ņŗĀņןĻĖ░ļŖźņØś ņØ╝ņ░© Ļ▓░Ļ│╝ņ¦ĆĒæ£(primary outcome)ļĪ£ ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£©(mL/min/1.73 m2)ņØä ņäĀņĀĢĒĢśņśĆĻ│Ā, ņĄ£ļīĆ 208ņŻ╝Ļ╣īņ¦Ć ļ│┤Ļ│ĀļÉ£ Ļ▓░Ļ│╝ļōżņØä ļīĆņāüņ£╝ļĪ£ ļ®öĒāĆļČäņäØņØä ņŗżņŗ£ĒĢśņśĆļŗż. 12ņŻ╝ņÖĆ 24ņŻ╝ņŚÉņä£ļŖö ņżæņ×¼ĻĄ░ņØś ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£©ņØ┤ ļīĆņĪ░ĻĄ░ņŚÉ ļ╣äĒĢ┤ ļé«ņĢśĻ│Ā(12ņŻ╝: -1.81, 95% CI -3.03 to -0.58, 24ņŻ╝: -1.33, 95% CI -2.52 to -0.15), 52ņŻ╝ņÖĆ 104ņŻ╝ņŚÉņä£ļŖö ļīĆņĪ░ĻĄ░Ļ│╝ ņ░©ņØ┤Ļ░Ć ņŚåņŚłĻ│Ā(52ņŻ╝: -0.76, 95% CI -1.90 to 0.38, 104ņŻ╝: 1.54, 95% CI -0.08 to 3.15, 156ņŻ╝ņÖĆ 208ņŻ╝ņŚÉņä£ļŖö ļīĆņĪ░ĻĄ░ļ│┤ļŗż ņ£ĀņØśĒĢśĻ▓ī ļåÆņĢśļŗż(156ņŻ╝: 2.54, 95% CI 1.65 to 3.43, 208ņŻ╝: 3.96, 95% CI 3.13 to 4.80) (Fig. 1A). ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£©ņØś ļ│ĆĒÖö(mean change of eGFR, mL/min/1.73 m2) ļŖö 156ņŻ╝ņŚÉņä£ ņżæņ×¼ĻĄ░ņØ┤ ļīĆņĪ░ĻĄ░ļ│┤ļŗż ņ£ĀņØśĒĢśĻ▓ī ļåÆņĢśļŗż(156ņŻ╝: 1.42, 95% CI 0.42 to 2.41) (Fig. 1B).
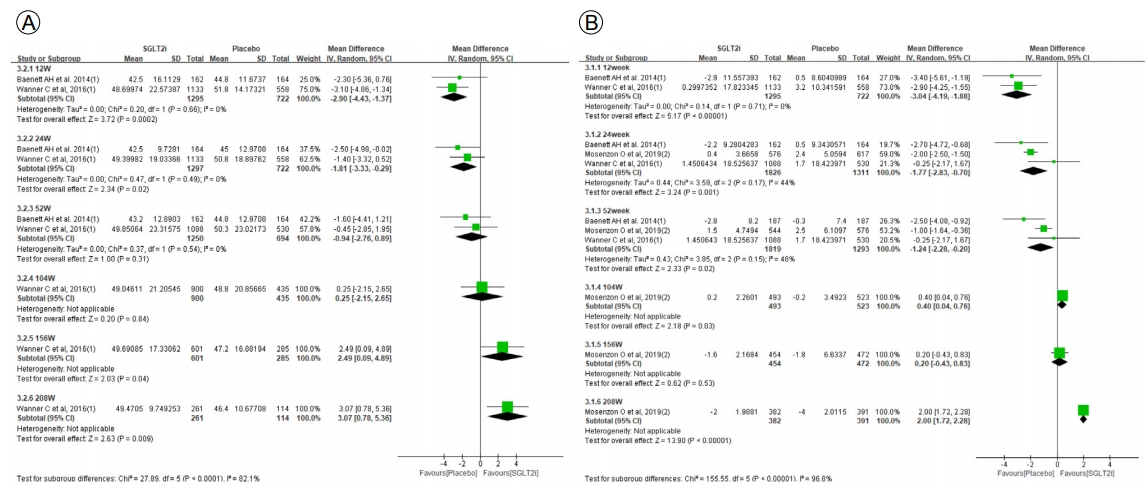
ļČäņäØ ļīĆņāüņ×É ņżæ ļ¦īņä▒ ņŗĀņ¦łĒÖś 3ĻĖ░(ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© 30-59 mL/min/1.73 m2) ļīĆņāüņ×Éļ¦īņØä ļö░ļĪ£ ļČäņäØĒĢśņśĆņØä ļĢī, 12ņŻ╝ņÖĆ 24ņŻ╝ņŚÉņä£ļŖö ņżæņ×¼ĻĄ░ņØś ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£©ņØ┤ ļīĆņĪ░ĻĄ░ņŚÉ ļ╣äĒĢ┤ ļé«ņĢśĻ│Ā(12ņŻ╝: -2.90, 95% CI -4.43 to -1.37, 24ņŻ╝: -1.81, 95% CI -3.33 to -0.29) 156ņŻ╝ņÖĆ 208ņŻ╝ņŚÉņä£ļŖö ņżæņ×¼ĻĄ░ņØś ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£©ņØ┤ ļīĆņĪ░ĻĄ░ņŚÉ ļ╣äĒĢ┤ ļåÆņØĆ Ļ▓ĮĒ¢źņØä ļ│┤ņśĆļŗż(156ņŻ╝: 2.49, 95% CI 0.09 to 4.89, 208ņŻ╝: 3.07, 95% CI 0.78 to 5.36) (Fig. 2A). ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© ļ│ĆĒÖö(mean change of eGFR, mL/min/1.73 m2) 208ņŻ╝ņ¦Ė ļīĆņĪ░ĻĄ░ļ│┤ļŗż ņżæņ×¼ĻĄ░ņŚÉņä£ ņ£ĀņØśļ»ĖĒĢ£ ĒÜ©Ļ│╝ ņČöņĀĢņ╣śļź╝ ļ│┤ņśĆļŗż(208ņŻ╝: 2.00, 95% CI 1.72 to 2.28) (Fig. 2B).
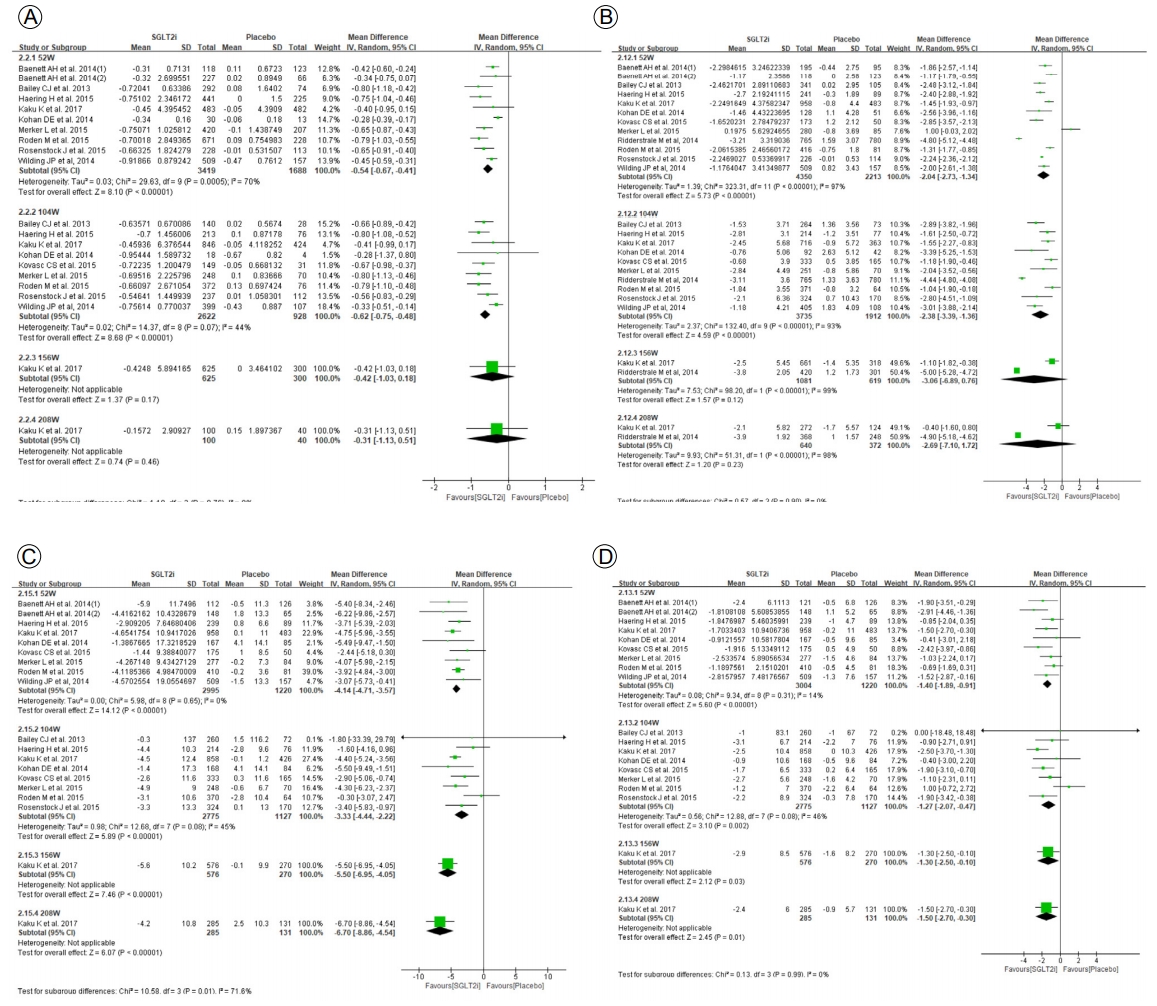
ņĀäņ▓┤ ļīĆņāüņ×ÉņŚÉņä£ ļŗ╣ĒÖöĒśłņāēņåī, ņ▓┤ņżæ, ĒśłņĢĢ ļ│ĆĒÖöļź╝ ļ╣äĻĄÉĒĢśņśĆņØä ļĢī, 104ņŻ╝ņ¦Ė ņżæņ×¼ĻĄ░ņŚÉņä£ ļŗ╣ĒÖöĒśłņāēņåī ļ│ĆĒÖöļŖö -0.62% (95% CI -0.75 to 0.48), ņ▓┤ņżæ ļ│ĆĒÖöļŖö -2.38 kg (95% CI -3.39 to -1.36), ņłśņČĢĻĖ░ ĒśłņĢĢ ļ│ĆĒÖöļŖö -3.33 mmHg (95% CI -4.44 to -2.22), ņØ┤ņÖäĻĖ░ ĒśłņĢĢ ļ│ĆĒÖöļŖö -1.27 mmHg (95% CI -2.07 to -0.47)ļĪ£ Ēśłļŗ╣, ņ▓┤ņżæ, ĒśłņĢĢņØĆ ļīĆņĪ░ĻĄ░ ļīĆļ╣ä ņżæņ×¼ĻĄ░ņŚÉņä£ ņ£ĀņØśļ»ĖĒĢ£ Ļ░Éņåīļź╝ ļ│┤ņśĆļŗż(Fig. 3). ņØ┤ņāüņŚÉņä£ ņĀ£2ĒśĢ ļŗ╣ļć©ļ│æ ĒÖśņ×ÉņŚÉņä£ ņןĻĖ░Ļ░ä SGLT2 ņ¢ĄņĀ£ņĀ£ ņ╣śļŻīļŖö ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© Ļ░Éņåīļź╝ ņ¢ĄņĀ£ĒĢśļŖö ĒÜ©Ļ│╝Ļ░Ć ņ׳ņØä Ļ▓āņ£╝ļĪ£ ĻĖ░ļīĆļÉ£ļŗż.
ņ£äĒĢ┤
ļīĆņĪ░ĻĄ░ļ│┤ļŗż ņżæņ×¼ĻĄ░ņŚÉņä£ ņ┤łļ░śĻĖ░ ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© Ļ░ÉņåīĻ░Ć ņ׳ņŚłņ£╝ļ®░(Fig. 1), ĒŖ╣Ē׳ ļ¦īņä▒ ņŗĀņ¦łĒÖś 3ĻĖ░ ĒÖśņ×ÉņŚÉņä£ļŖö SGLT2 ņ¢ĄņĀ£ņĀ£ ņé¼ņÜ® ņ┤łĻĖ░ņŚÉ ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© Ļ░ÉņåīĻ░Ć ļŹö Ēü¼Ļ▓ī ļéśĒāĆļé¼ļŗż(Fig. 3). ĒĢśņ¦Ćļ¦ī 2ļģä ņØ┤ņāü ņČöņĀü Ļ┤Ćņ░░ ĻĖ░Ļ░ä ļÅÖņĢł ĒāłļØĮļÉ£ ĒÖśņ×ÉĻ░Ć ļ¦ÄņĢä ņ┤łļ░śņŚÉ ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© Ļ░Éņåīļź╝ ļ│┤ņśĆļŹś ļīĆņāüņ×ÉļōżņŚÉņä£ ņØ┤Ēøä ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£©ņØ┤ ĒÜīļ│ĄļÉśņŚłļŖöņ¦Ć ņŚ¼ļČĆņŚÉ ļīĆĒĢ┤ņä£ļŖö ņĢī ņłś ņŚåņŚłĻĖ░ ļĢīļ¼ĖņŚÉ SGLT2 ņ¢ĄņĀ£ņĀ£ ņé¼ņÜ® ņŗ£ ņ┤łĻĖ░ņŚÉ ņŗĀņןĻĖ░ļŖźņØä ļ¬©ļŗłĒä░ļ¦üĒĢśĻ│Ā ņØ┤ĒøäņŚÉļÅä ņĀĢĻĖ░ņĀüņØ┤Ļ│Ā ņ¦ĆņåŹņĀüņØĖ ļ¬©ļŗłĒä░ļ¦üņØ┤ ĒĢäņÜöĒĢśļŗż.
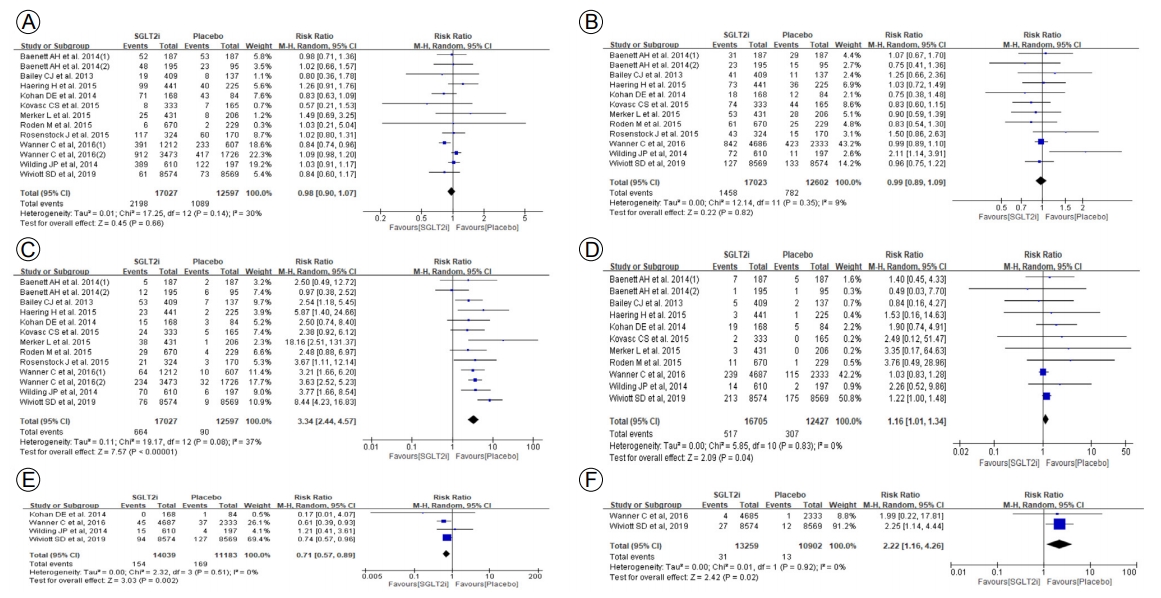
208ņŻ╝ Ļ┤Ćņ░░ ĻĖ░Ļ░ä ļÅÖņĢł ņżæņ×¼ĻĄ░ņŚÉņä£ ņĀĆĒśłļŗ╣ ļ░£ņāØ(RR 0.98, 95% CI 0.90 to 1.07), ņÜöļĪ£Ļ░ÉņŚ╝(RR 0.99, 95% CI 0.89 to 1.09)ņØś ņ£äĒŚśņØĆ ņ”ØĻ░ĆĒĢśņ¦Ć ņĢŖņĢśņ£╝ļéś, ņāØņŗØĻĖ░Ļ│ä Ļ░ÉņŚ╝(RR 3.34, 95% CI 2.44 to 4.57)Ļ│╝ ņłśļČä ļČĆņĪ▒(RR 1.16, 95% CI 1.01 to 1.34)ņØĆ ņØśļ»Ėņ׳Ļ▓ī ņ”ØĻ░ĆĒĢśņśĆļŗż. ļ░śļ®┤ ĻĖēņä▒ ņŗĀļČĆņĀä(RR 0.71, 95% CI 0.57 to 0.89), ļŗ╣ļć©ļ│æņä▒ņ╝ĆĒåżņé░ņ”Ø(RR 2.22, 95% CI 1.16 to 4.26)ņØś ļ░£ņāØņØĆ ĒåĄĻ│äņĀüņ£╝ļĪ£ļŖö ņ£ĀņØśļ»ĖĒĢśņśĆņ£╝ļéś ļ░£ņāØĻ▒┤ņłśĻ░Ć ļäłļ¼┤ ņĀüņ¢┤ņä£ ņ×äņāüņĀü ņ£ĀņØśņä▒ņØĆ ņŚåļŖö Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż(Fig. 4).
ĻČīĻ│Ā Ļ░ĢļÅä: ņØ┤ļōØĻ│╝ ņ£äĒĢ┤ņØś ĻĘĀĒśĢņŚÉ ļö░ļźĖ ĻČīĻ│Ā
ņĀ£2ĒśĢ ļŗ╣ļć©ļ│æ ĒÖśņ×ÉņŚÉņä£ 2ļģä Ēś╣ņØĆ ĻĘĖ ņØ┤ņāü ņןĻĖ░Ļ░ä SGLT2 ņ¢ĄņĀ£ņĀ£ ņ╣śļŻī ņŗ£ ņ£äņĢĮ ļīĆļ╣ä ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© Ļ░Éņåīļź╝ ņ¢ĄņĀ£ĒĢśļŖö ĒÜ©Ļ│╝Ļ░Ć ņ׳ņŚłļŗż(Figs. 1 and 2). ļśÉĒĢ£ ļŗ╣ĒÖöĒśłņāēņåīņØś Ļ░ÉņåīņÖĆ ĒĢ©Ļ╗ś ņ▓┤ņżæ, ņłśņČĢĻĖ░ ļ░Å ņØ┤ņÖäĻĖ░ ĒśłņĢĢņØś Ļ░ÉņåīļĪ£ ņØĖĒĢ£ ņČöĻ░Ć ņØ┤ļōØņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż(Fig. 3). SGLT2 ņ¢ĄņĀ£ņĀ£ ņ╣śļŻī ņŗ£ ļ░£ņāØĒĢĀ ņłś ņ׳ļŖö ņ£äĒĢ┤ļĪ£ļŖö ņāØņŗØĻĖ░Ļ│ä Ļ░ÉņŚ╝, Ēāłņłś ļō▒ņØ┤ ņ׳ņŚłņ£╝ļéś ņāØņŗØĻĖ░Ļ│ä Ļ░ÉņŚ╝ņØ┤ļéś ĒāłņłśļŖö ļ╣äĻĄÉņĀü Ļ░äļŗ©ĒĢ£ ņśłļ░®ņĀü ņĪ░ņ╣śņÖĆ ņ╣śļŻīļĪ£ ņēĮĻ▓ī Ļ░£ņäĀļÉśļ»ĆļĪ£ ņŗ¼Ļ░üĒĢ£ ņ£äĒĢ┤ļŖö ņĢäļŗī Ļ▓āņ£╝ļĪ£ ĒīÉļŗ©ļÉ£ļŗż(Fig. 4). ļö░ļØ╝ņä£ ņØ┤ļź╝ ņóģĒĢ®ĒĢ┤ ļ│╝ ļĢī ņØ┤ļōØņØ┤ ņ£äĒĢ┤ļź╝ ņĢ×ņäĀļŗżĻ│Ā ļ│╝ ņłś ņ׳ļŗż.
ĻĘĖļ¤¼ļéś 2ļģä ņØ┤ņāü ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£©ņØä ņןĻĖ░ ņČöņĀü Ļ┤Ćņ░░ĒĢ£ ņŚ░ĻĄ¼Ļ░Ć ņĀüĻ│Ā ĻĘĖļéśļ¦ł ņןĻĖ░Ļ░ä ņŚ░ĻĄ¼ļōżņŚÉņä£ļŖö ĒāłļØĮļźĀņØ┤ ļåÆņĢśļŗż. ĒĢ£ĒÄĖ ļ¦īņä▒ ņŗĀņ¦łĒÖś 3ĻĖ░ņŚÉņä£ļÅä ņØśļ»Ė ņ׳ļŖö ĒÜ©Ļ│╝ņČöņĀĢņ╣śļź╝ ļ│┤ņśĆņ£╝ļéś ņØ┤ ļČäņäØņŚÉ ĒżĒĢ©ļÉ£ ņŚ░ĻĄ¼Ļ░Ć ļŗ© 1Ļ░£ļ┐ÉņØ┤ņ¢┤ņä£(Fig. 2) ņżæļō▒ļÅäņØś ņŗĀĻĖ░ļŖź ņĀĆĒĢśļź╝ ļÅÖļ░śĒĢ£ ĒÖśņ×ÉņŚÉņä£ SGLT2 ņ¢ĄņĀ£ņĀ£ņØś ņŗĀņןĻĖ░ļŖźņŚÉ ļīĆĒĢ£ ĒÜ©Ļ│╝ļŖö ņČöĻ░ĆņĀüņØĖ ņŚ░ĻĄ¼ļź╝ ĒåĄĒĢ┤ ĒÖĢņØĖņØ┤ ĒĢäņÜöĒĢśļŗż. ļīĆņĪ░ĻĄ░ņŚÉ ļ╣äĒĢ┤ ņżæņ×¼ĻĄ░ņŚÉņä£ ņ┤łļ░śņŚÉ ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£©ņØ┤ Ļ░ÉņåīĒĢśņśĆļŖöļŹ░(Fig. 1), ļ¦īņä▒ ņŗĀņ¦łĒÖś 3ĻĖ░ ļīĆņāüņ×ÉļōżņØĆ ĻĘĖ Ļ░ÉņåīĻ░Ć ļŹö ņ╗Ėļŗż(Fig. 2). ļö░ļØ╝ņä£ SGLT2 ņ¢ĄņĀ£ņĀ£ ņ╣śļŻī ņŗ£ ņ┤łļ░śĻĖ░ ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© Ļ░ÉņåīņŚÉ ļīĆĒĢ£ ņ£äĒĢ┤Ļ░Ć ņĪ┤ņ×¼ĒĢśļ»ĆļĪ£ SGLT2 ņ¢ĄņĀ£ņĀ£ ņé¼ņÜ® ņŗ£ ņŗĀņןĻĖ░ļŖźņŚÉ ļīĆĒĢ£ ņĀĢĻĖ░ņĀüņØ┤Ļ│Ā ņ¦ĆņåŹņĀüņØ┤ ļ¬©ļŗłĒä░ļ¦üņØ┤ ļ¦żņÜ░ ņżæņÜöĒĢśļŗż.
ĒĢ£ĒÄĖ, ņĢäņŗ£ņĢäņØĖņØ┤ ļŗżņłś ĒżĒĢ©ļÉ£ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļŖö ņĀäņ▓┤ ļīĆņāüņ×ÉņØś ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ņÖĆ ļŗ¼ļ×ÉļŖöļŹ░ ņĀäņ▓┤ ļīĆņāüņ×É ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņ┤łļ░śĻĖ░ ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£©ņØ┤ Ļ░ÉņåīļÉśļŗżĻ░Ć ņŗ£Ļ░äņØ┤ ņ¦Ćļéśļ®┤ņä£ ĒÜīļ│ĄļÉśņ¢┤ 2ļģä ņ┤łĻ│╝ ņŗ£ Ļ░£ņäĀļÉśļŖö Ļ▓ĮĒ¢źņØä ļ│┤ņśĆļŖöļŹ░, ņĢäņŗ£ņĢäņØĖņØ┤ ļŗżņłś ĒżĒĢ©ļÉ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ļīĆņĪ░ĻĄ░Ļ│╝ ņżæņ×¼ĻĄ░ Ļ░ä ņ┤łļ░śĻĖ░ ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© Ļ░ÉņåīņØś ņ░©ņØ┤Ļ░Ć ņŚåņŚłĻ│Ā, 208ņŻ╝Ļ╣īņ¦Ć ņןĻĖ░Ļ░ä ņČöņĀü Ļ┤Ćņ░░ ĻĖ░Ļ░ä ļÅÖņĢłņŚÉļÅä ņ£ĀņØśļ»ĖĒĢ£ ņ░©ņØ┤Ļ░Ć ņŚåņŚłļŗż(ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© ļ│ĆĒÖö, -0.47 mL/min/1.73 m2 [95% CI, -4.01 to 3.08]) (Supplementary Fig. 2). ļö░ļØ╝ņä£ ņĢäņŗ£ņĢäņØĖņŚÉņä£ļÅä ņןĻĖ░Ļ░äņØś SGLT2 ņ¢ĄņĀ£ņĀ£ ņ╣śļŻīĻ░Ć ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© Ļ░Éņåīļź╝ ņ¢ĄņĀ£ĒĢśļŖö ĒÜ©Ļ│╝Ļ░Ć ņ׳ņØäņ¦ĆņŚÉ ļīĆĒĢ┤ņä£ļŖö ņĢäņ¦ü ļČłļČäļ¬ģĒĢśļŗż. ĻĘĖļ¤¼ļ»ĆļĪ£ Ē¢źĒøä ņĢäņŗ£ņĢäņØĖ, ĒŖ╣Ē׳ ĒĢ£ĻĄŁņØĖņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ ņČöĻ░ĆņĀüņØĖ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝Ļ░Ć ĒĢäņÜöĒĢśļŗż.
Ļ▓░ ļĪĀ
ņØ┤ļōØĻ│╝ ņ£äĒĢ┤ļź╝ ņóģĒĢ®ĒĢśņśĆņØä ļĢī, SGLT2 ņ¢ĄņĀ£ņĀ£ļŖö ņ£äņĢĮņŚÉ ļ╣äĒĢ┤ ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© Ļ░Éņåīļź╝ ņ¢ĄņĀ£ĒĢśļŖö ņØ┤ļōØņØ┤ ņ׳ņØä ņłś ņ׳ņ£╝ļéś ĻĘĖ ņØ┤ļōØņØ┤ ļÉśļŖö ļīĆņāüĻĄ░ņØ┤ ļ¬ģĒÖĢĒĢśņ¦Ć ņĢŖņ£╝ļ®░, ņŗ¼Ļ░üĒĢ£ ņ£äĒĢ┤ļŖö ņŚåņ£╝ļéś ņ┤łļ░śĻĖ░ ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© ņĀĆĒĢśĻ░Ć ņ׳ņØä ņłś ņ׳ņ£╝ļ»ĆļĪ£ ņĢĮņĀ£ ņé¼ņÜ® ņŗ£ņŚÉ ņŗĀņןĻĖ░ļŖźņŚÉ ļīĆĒĢ£ ļ¬©ļŗłĒä░ļ¦üĻ│╝ ņŻ╝ņØśĻ░Ć ĒĢäņÜöĒĢśļŗż. ļśÉĒĢ£ ņØ┤ļ¤¼ĒĢ£ ņØ┤ļōØĻ│╝ ņ£äĒĢ┤ņØś ĻĘĀĒśĢņŚÉ ņ׳ņ¢┤ņä£ ļČłĒÖĢņŗżņä▒ņØ┤ ņĪ┤ņ×¼ĒĢśļ»ĆļĪ£ ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© Ļ░Éņåī ņ¢ĄņĀ£ļź╝ ļ¬®ņĀüņ£╝ļĪ£ ļ¬©ļōĀ ņĀ£2ĒśĢ ļŗ╣ļć©ļ│æ ĒÖśņ×ÉņŚÉĻ▓ī SGLT2 ņ¢ĄņĀ£ņĀ£ ņé¼ņÜ®ņØä ĻČīĻ│ĀĒĢĀ ņłśļŖö ņŚåļŗż. ļö░ļØ╝ņä£ ĻČīĻ│Ā Ļ░ĢļÅäļŖö ŌĆ£weak recommendationŌĆØņ£╝ļĪ£ Ļ▓░ņĀĢĒĢśņśĆļŗż. ņØ┤ņŚÉ ņĄ£ņóģ ĻČīĻ│ĀņĢłņØĆ ļŗżņØīĻ│╝ Ļ░ÖņØ┤ Ļ▓░ņĀĢĒĢśņśĆļŗż.
ĻČīĻ│ĀņĢł
ņĀ£2ĒśĢ ļŗ╣ļć©ļ│æņŚÉņä£ ņןĻĖ░Ļ░äņØś SGLT-2 ņ¢ĄņĀ£ņĀ£ ņ╣śļŻīļŖö ņØ╝ļČĆ ļīĆņāüņ×ÉņŚÉņä£ ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© Ļ░Éņåīļź╝ ņ¢ĄņĀ£ĒĢśļŖö ĒÜ©Ļ│╝Ļ░Ć ņ׳ņ£╝ļ»ĆļĪ£, ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£©ņØä ņ¦ĆņåŹņĀüņ£╝ļĪ£ ņČöņĀü Ļ┤Ćņ░░ĒĢśļ®┤ņä£ SGLT-2 ņ¢ĄņĀ£ņĀ£ļź╝ ņé¼ņÜ®ĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢ£ļŗż(weak recommendation, low evidence).
ĻĖ░ ĒāĆ
ņĀ£2ĒśĢ ļŗ╣ļć©ļ│æ ĒÖśņ×ÉņŚÉĻ▓ī ņČöĻ░Ć ļ│æĒĢ®ņÜöļ▓Ģņ£╝ļĪ£ ņäĀĒāØĒĢĀ ņłś ņ׳ļŖö Ēśłļŗ╣Ļ░ĢĒĢśņĀ£ļōżņØĆ SGLT2 ņ¢ĄņĀ£ņĀ£ ņÖĖņŚÉļÅä Ļ▓ĮĻĄ¼ Ēśłļŗ╣Ļ░ĢĒĢśņĀ£ņÖĆ ņŻ╝ņé¼ņĀ£Ļ░Ć ņ׳ņ£╝ļéś, Ēśäņ×¼ļĪ£ņä£ļŖö ņןĻĖ░Ļ░ä ņŗĀņןĻĖ░ļŖź Ļ░£ņäĀĒÜ©Ļ│╝ļź╝ ņ×ģņ”ØĒĢ£ ĻĘ╝Ļ▒░Ļ░Ć ļČĆņĪ▒ĒĢśļ®░ ņé¼ĻĄ¼ņ▓┤ ņŚ¼Ļ│╝ņ£© ļ│ĆĒÖöļź╝ ļ│┤ĻĖ░ ņ£äĒĢ┤ņä£ļŖö ņĄ£ņåīĒĢ£ 1ļģä ņØ┤ņāüņØś ņןĻĖ░ņĀüņØĖ ņ╣śļŻī, ļÅÖļ░ś ņ£äĒŚśņØĖņ×ÉņØś ĻĄÉņĀĢ(Ļ│ĀĒśłņĢĢ, ņØ┤ņāüņ¦Ćņ¦łĒśłņ”Ø, ļ╣äļ¦ī ļō▒), ĻĖ░ĒāĆ ņŗĀņןĻĖ░ļŖź Ļ░£ņäĀņØ┤ ņ”Øļ¬ģļÉ£ ņĢĮņĀ£(ņĢłņ¦ĆņśżĒģÉņŗĀņĀäĒÖśņ¢ĄņĀ£ņĀ£, ņĢłņ¦ĆņśżĒģÉņŗĀņłśņÜ®ņ▓┤ņ░©ļŗ©ņĀ£ ļō▒)ņØś ņÜ░ņäĀņł£ņ£ä ļō▒ņØä ņČ®ļČäĒ׳ Ļ│ĀļĀżĒĢśņŚ¼ Ļ▓░ņĀĢĒĢ┤ņĢ╝ ĒĢ£ļŗż. SGLT2 ņ¢ĄņĀ£ņĀ£ Ēł¼ņŚ¼ Ēøä ĒÖśņ×ÉņØś ņŻ╝Ļ┤ĆņĀü ļČłĒÄĖĻ░É(ĻĖēĻ▓®ĒĢ£ ņ▓┤ņżæ Ļ░Éņåīļéś ļ╣łļć© ļō▒), ņÜöļĪ£Ļ░ÉņŚ╝, ļ╣äņÜ®, ņ┤łĻĖ░ ņŗĀņןĻĖ░ļŖź Ļ░ÉņåīņŚÉ ļīĆĒĢ┤ ņØśņé¼ņØś ļČĆļŗ┤Ļ░ÉņŚÉ ļīĆĒĢ£ Ļ│ĀļĀżĻ░Ć ĒĢäņÜöĒĢśļ®░, Ļ░ÉņŚ╝ņØ┤ļéś ĒāłņłśņŚÉ ļīĆĒĢ£ ļ¼ĖņĀ£ļŖö ĒÖśņ×ÉņŚÉĻ▓ī ļ»Ėļ”¼ ļ░£ņāØ Ļ░ĆļŖźņä▒ņØä ņČ®ļČäĒ׳ Ļ│Āņ¦ĆĒĢśĻ│Ā ņĪ░ĻĖ░ ļ░£Ļ▓¼ ļ░Å ņĀüņĀłĒĢ£ ņĪ░ņ╣śļĪ£ ĒĢ┤Ļ▓░ĒĢĀ ņłś ņ׳ļÅäļĪØ ĒĢ┤ņĢ╝ ĒĢ£ļŗż. ļśÉĒĢ£ ĻĖ░ņĪ┤ņØś ļīĆļČĆļČä ņןĻĖ░ ļīĆĻĘ£ļ¬© ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļōżņØĆ ņĢäņŗ£ņĢäņØĖņØś ļ╣äņ£©ņØ┤ ņĀüņØĆ ņä£ņ¢æņØĖ ņ£äņŻ╝ņØś Ļ▓░Ļ│╝ņØ┤ļ»ĆļĪ£ Ē¢źĒøä ĒĢ£ĻĄŁņØĖ ļīĆņāüņØś ņČöĻ░Ć ņŚ░ĻĄ¼Ļ░Ć ĒĢäņÜöĒĢśļŗż.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






