


ņä£ ļĪĀ
ņŗ¼ļ░®ņäĖļÅÖņØĆ ņŻ╝ļĪ£ Ļ│ĀļĀ╣ņŚÉņä£ ļ░£ņāØĒĢśļŖö ņ¦ĆņåŹņä▒ ļČĆņĀĢļ¦źņØś Ļ░Ćņן ĒØöĒĢ£ ĒśĢĒā£ņØ┤ļŗż. ĻĘĖļ¤¼ļéś ņØ┤ļ¤¼ĒĢ£ ņŗ¼ļ░®ņäĖļÅÖņØĆ ņ”ØņāüņØ┤ ņŚåļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦ÄņĢä, Ļ▒┤Ļ░ĢĻ▓Ćņ¦äņØä ĒåĄĒĢśņŚ¼ ļ░£Ļ▓¼ņØä ĒĢśĻ▒░ļéś, ļŗżļźĖ ņ¦łļ│æņŚÉ ļīĆĒĢ£ Ļ▓Ćņé¼ ļÅäņżæ ņŗ¼ņĀäļÅä Ļ▓Ćņé¼ļĪ£ ņÜ░ņŚ░Ē׳ ļ░£Ļ▓¼ļÉśļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äļŗż. ĻĘĖļ¤╝ņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā ņŗ¼ļ░®ņäĖļÅÖņØĆ ĒŚłĒśłņä▒ ļćīņĪĖņżæņØä ļ╣äļĪ»ĒĢ£ ņāēņĀäņ”ØņØś ļ░£ņāØņØä ņ”ØĻ░Ćņŗ£Ēéżļ®░, ņŗ¼ļČĆņĀä, ņ╣śļ¦ż, ņ×ģņøÉņ£©ņØś ņ”ØĻ░Ć ļō▒ ĒÖśņ×ÉņØś ņŗ¼ĒśłĻ┤Ć Ļ┤ĆļĀ© ņśłĒøäļź╝ ņĢģĒÖöņŗ£ĒéżļŖö ņÜöņØĖņ£╝ļĪ£ ņ×æņÜ®ĒĢśĻ▓ī ļÉ£ļŗż[1,2]. ļö░ļØ╝ņä£ ņŗ¼ļ░®ņäĖļÅÖņØś ņ¦äļŗ©Ļ│╝ ņ╣śļŻīļŖö ĒÖśņ×Éļź╝ ņ▓śņØī ņĀæĒĢśĻ▓ī ļÉśļŖö ņØ╝ņ░© ņØśļŻīņØĖņŚÉņä£ļČĆĒä░ ņŗ£ņ×æļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż. ĻĘĖļ¤¼ĒĢ£ ņØśļ»ĖņŚÉņä£ ņŗ¼ļ░®ņäĖļÅÖņØś ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīļź╝ ļŗżņØīĻ│╝ Ļ░ÖņØĆ ļŗżņä» Ļ░Ćņ¦ĆņØś ļŗ©Ļ│äļĪ£ ļéśļłäņ¢┤ ņäżļ¬ģĒĢśĻ│Āņ×É ĒĢ£ļŗż(Fig. 1). 1) ņŗ¼Ļ░üĒĢ£ Ļ┤ĆļĀ© ņ”ØņāüņØś ņĪ░ņĀł, 2) Ļ┤ĆļĀ© ņ£äĒŚśņÜöņØĖ(Ļ░æņāüņäĀĻĖ░ļŖźĒĢŁņ¦äņ”Ø, ņłśņłĀ Ēøä ņāüĒā£)ņŚÉ ļÅÖļ░śļÉ£ ņŗ¼ĒśłĻ┤Ćņ¦łĒÖśņØś Ļ┤Ćļ”¼, 3) ņŗ¼ļ░®ņäĖļÅÖņ£╝ļĪ£ ņØĖĒĢ£ ļćīņĪĖņżæņØś ņśłļ░®, 4) ļ░ĢļÅÖņłśņØś ņĪ░ņĀł, 5) ņ”Øņāü ņĪ░ņĀłņØä ņ£äĒĢ£ ļ”¼ļō¼ ņĪ░ņĀł.
ņØ┤ņÖĆ Ļ░ÖņØĆ ņŗ¼ļ░®ņäĖļÅÖņŚÉ ļīĆĒĢ£ ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīļŖö Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉ ĻĘ╝Ļ▒░ĒĢ£ ņŗ¼ļ░®ņäĖļÅÖņØś ņØ╝Ļ┤ĆņĀüņØĖ ņ╣śļŻīņØś ĻĘ╝Ļ░äņØ┤ ļÉśļ®░ ĒÖśņ×ÉņØś ņ╣śļŻī ņä▒ņĀüņØä Ē¢źņāüņŗ£ĒéżļŖöļŹ░ ļÅäņøĆņØä ņżĆļŗż(Fig. 2) [3-6]. ĻĘĖļ”¼Ļ│Ā ņØ┤ļ¤¼ĒĢ£ ņ╣śļŻīļ▓ĢņØĆ ņäĖĻ│äļ│┤Ļ▒┤ĻĖ░ĻĄ¼(World Health Organization)ņŚÉņä£ ļ¦īņä▒ ņ¦łĒÖśņŚÉ ļīĆĒĢ£ ņĀäņØĖņĀüņØĖ ņĀæĻĘ╝Ļ│╝ ņ╣śļŻīļź╝ ņ£äĒĢśņŚ¼ ņĀ£ņĢłĒĢ£ ļé┤ņÜ®Ļ│╝ ņØ╝ņ╣śĒĢ£ļŗż[7]. ņŗ¼ĒśłĻ┤Ćņ¦łĒÖśņŚÉ ļīĆĒĢ£ ņŗ¼ļ░®ņäĖļÅÖņØś ņśüĒ¢źņØä ņĀĢĒÖĢĒ׳ ĒÅēĻ░ĆĒĢśĻĖ░ ņ£äĒĢ┤ņä£ļŖö, ņ┤łĻĖ░ ņ¦äļŗ© Ēøä, ĒŖ╣Ē׳ Ēæ£ 1ņŚÉņä£ ĻĖ░ņłĀļÉ£ ņāüĒÖ®ņ▓śļ¤╝ ņŗĀņåŹĒĢ£ ņ╣śļŻīĻ░Ć ĒĢäņÜöĒĢ£ Ļ▓ĮņÜ░ ņŗ¼ņןļé┤Ļ│╝ ņĀäļ¼Ė ņØśļŻīņ¦äņŚÉĻ▓ī ņØśļó░ĒĢśļŖö Ļ▓āņØ┤ ĒĢäņÜöĒĢśļŗż.
ļ┐Éļ¦ī ņĢäļŗłļØ╝, ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīļŖö ĻĖ░ņĪ┤ņØś ĒåĄņāüņĀüņØĖ ņŗ¼ļ░®ņäĖļÅÖņŚÉ ļīĆĒĢ£ ņ╣śļŻīņŚÉņä£ ļ│┤ņŚ¼ņ¦ĆļŖö ĒĢŁņØæĻ│ĀņĀ£ņÖĆ ņ”Øņāü ņĪ░ņĀłņØä ņ£äĒĢ£ ņĢĮļ¼╝ņØś ļČĆņĀüņĀłĒĢ£ ņé¼ņÜ®ņØś ĒĢ£Ļ│äļź╝ ĻĘ╣ļ│ĄĒĢśĻ│Ā, Ļ┤ĆļĀ© ņŗ¼ĒśłĻ┤Ćņ¦łĒÖśņØś ņ£äĒŚśņØä Ļ░Éņåīņŗ£ĒéżļŖö ļŹ░ ļÅäņøĆņØä ņżä ņłś ņ׳ļŗż. ļö░ļØ╝ņä£ ņŗ¼ļ░®ņäĖļÅÖņŚÉ ļīĆĒĢ£ ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīļŖö ĒÖśņ×Éļź╝ ņ▓śņØī ņĀæĒĢśĻ▓ī ļÉśļŖö ņØ╝ņ░© ņØśļŻīņ¦äņØś ĒśæņĪ░ļź╝ ĒĢäņÜöļĪ£ ĒĢśĻ▓ī ļÉśļ®░, ņØ┤Ēøä ĒÖśņ×Éļź╝ ĒżĒĢ©ĒĢ£ ņŗ¼ņןļé┤Ļ│╝, ņÖĖĻ│╝, ļćīņĪĖņżæ ņĀäļ¼ĖņØśņŚÉ ņØ┤ļź┤ĻĖ░Ļ╣īņ¦Ć ņĀäļ¼ĖņĀüņØĖ ņ¦äļŻīņØśļōżņØś ļŗżĒĢÖņĀ£ņĀü ņĀæĻĘ╝ņØ┤ ļÆżļö░ļź┤Ļ▓ī ļÉ£ļŗż(Table 2). ņØ┤ņŚÉ ļ│Ė ņ¦äļŻī ņ¦Ćņ╣©ņŚÉņä£ļŖö ņŗ¼ļ░®ņäĖļÅÖņØś ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīņŚÉ ļīĆĒĢ£ ņØśĒĢÖņĀü ĻĘ╝Ļ▒░ļź╝ ņé┤ĒÄ┤ļ│┤Ļ│Ā, ņŗ¼ļ░®ņäĖļÅÖņØś ļ░£ņāØĻ│╝ ņśłĒøäņŚÉ ņśüĒ¢źņØä ņŻ╝ļŖö ņÜöņØĖļōżņŚÉ ļīĆĒĢ£ ņóģĒĢ®ņĀüņØĖ ņ¦äļŗ©Ļ│╝ ņ╣śļŻī ņøÉņ╣ÖņŚÉ ļīĆĒĢśņŚ¼ ņĢīņĢäļ│┤Ļ│Āņ×É ĒĢ£ļŗż. ĻĘĖļ”¼Ļ│Ā ņŗ¼ļ░®ņäĖļÅÖņØś ĒåĄĒĢ®ņĀü ņ╣śļŻīņŚÉņä£ ņżæņÜöĒĢ£ ņČĢņØä ņØ┤ļŻ©Ļ│Ā ņ׳ļŖö ĒÖśņ×É ĻĄÉņ£ĪĻ│╝ ņ░ĖņŚ¼ ĻĘĖļ”¼Ļ│Ā ĻĘĖļōżņŚÉ ļīĆĒĢ£ ņ▓┤Ļ│äņĀüņØĖ ņČöņĀü Ļ┤Ćņ░░ņŚÉ ļīĆĒĢśņŚ¼ ņé┤ĒÄ┤ļ│┤Ļ│Āņ×É ĒĢ£ļŗż.
ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīņØś ņØśĒĢÖņĀü ĻĘ╝Ļ▒░ ļ░Å ĻĄ¼ņä▒ ņÜöņåī
ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīņØś ņØśĒĢÖņĀü ĻĘ╝Ļ▒░
ņŗ¼ļ░®ņäĖļÅÖņŚÉ ļīĆĒĢ£ ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīņŚÉļŖö ĒÖśņ×ÉņÖĆ ņØśļŻīņ¦ä ĻĘĖļ”¼Ļ│Ā ņØ┤ļź╝ ļÆĘļ░øņ╣©ĒĢśļŖö ļŗżņ¢æĒĢ£ ļ░®ņŗØņØś ņØśļŻī ĻĖ░ņłĀņĀüņØĖ ņÜöņåīļōżņØ┤ ĒżĒĢ©ļÉ£ļŗż. ņØ┤ļ¤░ ļ░®ņŗØņØś ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīļŖö Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉ ĻĘ╝Ļ▒░ĒĢ£ ņŗ¼ļ░®ņäĖļÅÖņØś ņØ╝Ļ┤ĆņĀüņØĖ ņ╣śļŻīņØś ĻĘ╝Ļ░äņØ┤ ļÉśļ®░ ĻČüĻĘ╣ņĀüņ£╝ļĪ£ ĒÖśņ×ÉņØś ņ╣śļŻī ņä▒ņĀüņØä Ē¢źņāüņŗ£ĒéżļŖöļŹ░ ļÅäņøĆņØä ņżĆļŗż[3-6]. ņŗ¼ļ░®ņäĖļÅÖņŚÉ ļīĆĒĢ£ ļ¼┤ņ×æņ£ä ļīĆņĪ░ ņŗżĒŚśņŚÉņä£, ĒåĄĒĢ®ņĀüņØĖ ņ¦łļ│æņØś ņ╣śļŻīļŖö ņØ╝ļ░śņĀüņØĖ ņ╣śļŻīņŚÉ ļ╣äĒĢśņŚ¼, ņŗ¼ĒśłĻ┤Ćņ¦łĒÖśņ£╝ļĪ£ ņØĖĒĢ£ ņ×ģņøÉĻ│╝ ņé¼ļ¦ØņØä 22Ļ░£ņøöĻ░ä 1/3Ļ╣īņ¦Ć Ļ░Éņåīņŗ£ņ╝░ļŗż[8]. ĻĘĖļ”¼Ļ│Ā ņŗ¼ļ░®ņäĖļÅÖņŚÉ ļīĆĒĢ£ ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīļŖö ļ╣äņÜ® ĒÜ©Ļ│╝ņĀüņØĖ ņĖĪļ®┤ņŚÉņä£ļÅä ĻĖŹņĀüņĀüņØĖ ĒÜ©Ļ│╝ļź╝ Ļ▒░ļæÉņŚłņ£╝ļ®░[9], ņØ┤ņŚÉ ļīĆĒĢ£ 2Ļ░£ņØś ļīĆĻĘ£ļ¬© Ļ┤Ćņ░░ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņØ╝ļ░śņĀüņØĖ ņŗ¼ļ░®ņäĖļÅÖņŚÉ ļīĆĒĢ£ ņ╣śļŻīņŚÉ ļ╣äĒĢśņŚ¼ ļé«ņØĆ ņ×ģņøÉņ£©[10,11], ļé«ņØĆ ļćīņĪĖņżæņØś ļ░£ņāØ[10]ņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż. ĻĘĖļ”¼Ļ│Ā ņŗ¼ļ░®ņäĖļÅÖĻ│╝ Ļ┤ĆļĀ©ĒĢ£ ņØæĻĖēņŗż ļé┤ņøÉ ļ╣äņ£©ņØś Ļ░Éņåī, ņŗ¼ĒśłĻ┤ĆĻ│ä ņ×ģņøÉ ļ╣äņ£©ņØś Ļ░Éņåī, ņé¼ļ¦ØļźĀņØś Ļ░Éņåī ļō▒ņØś ĒÜ©Ļ│╝ļź╝ ļ│┤ņŚ¼ņŻ╝ņŚłļŗż[12]. ņØ┤ņ▓śļ¤╝, ņāłļĪŁĻ▓ī ļ░£ņāØĒĢ£ ņŗ¼ļ░®ņäĖļÅÖņØś ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīļŖö ļ░ĢļÅÖņłś ņĪ░ņĀłĻ│╝ ļ”¼ļō¼ ņĪ░ņĀł ĻĘĖļ”¼Ļ│Ā ĒĢŁņØæĻ│Ā ņ╣śļŻīņŚÉ ņ׳ņ¢┤ņä£ ļČĆņĀüņĀłĒĢ£ ņ╣śļŻīļĪ£ ņØĖĒĢ£ ņŗ¼ĒśłĻ┤Ć ņé¼Ļ▒┤ņØś ņ”ØĻ░Ćļź╝ ņśłļ░®ĒĢśļŖö ļŹ░ņŚÉļÅä ļÅäņøĆņØä ņŻ╝ņŚłļŗż.
ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīņØś ĻĄ¼ņä▒ ņÜöņåī
ĒÖśņ×ÉņØś ņĀüĻĘ╣ņĀü ņ░ĖņŚ¼
ņŗ¼ļ░®ņäĖļÅÖĻ│╝ Ļ░ÖņØĆ ļ¦īņä▒ ņ¦łĒÖśņØĆ ĒÖśņ×É ņŖżņŖżļĪ£ ļ│æņŚÉ ļīĆĒĢ£ ņ¦ĆņŗØņØä ņל Ļ░¢ņČöĻ│Ā ņ╣śļŻī Ļ│╝ņĀĢņŚÉņä£ ņ×ÉņŗĀņØś ņ▒ģņ×äņØä ņØĖņ¦ĆĒĢśĻ│Ā ņ׳ļŖö Ļ▓ĮņÜ░ņŚÉ ļŹö ļéśņØĆ ņןĻĖ░ņĀü ņ╣śļŻī ĒÜ©Ļ│╝ļź╝ ĻĖ░ļīĆĒĢĀ ņłś ņ׳ļŗż[7]. ņ╣śļŻī Ļ▓░ņĀĢ ļŗ©Ļ│äņŚÉ ĒÖśņ×Éļź╝ ņ░ĖņŚ¼ņŗ£ĒéżļŖö ļō▒ ĒÖśņ×É ņżæņŗ¼ņØś ņ╣śļŻīļź╝ ĒĢśĻ▓ī ļÉśļ®┤ ņ╣śļŻīņł£ņØæļÅäļź╝ ļåÆņØ┤Ļ│Ā ĒÖśņ×É Ļ░£Ļ░£ņØĖņØś ņäĀĒśĖļÅäļéś ņÜöĻĄ¼ņé¼ĒĢŁ ļ░Å ņ×Éņ£©ĻČīņØä ņĪ┤ņżæĒĢĀ ņłś ņ׳ļŗż[13]. ņ╣śļŻī Ļ│╝ņĀĢņŚÉņä£ ĒÖśņ×ÉņØś ņŚŁĒĢĀņØä Ļ░ĢĒÖöĒĢśĻ│Ā ļŖźļÅÖņĀüņØĖ Ļ░£ņ×ģņØä ņŗ£ņ╝░ņØä ļĢī ņ╣śļŻī ņä▒ņĀüņØ┤ Ē¢źņāüļÉ©ņØ┤ ņ×ģņ”ØļÉ£ ļ░ö ņ׳ļŗż[14,15]. ĒÖśņ×É ņżæņŗ¼ ņ╣śļŻīļź╝ ņ£äĒĢ┤ņä£ļŖö ĒåĄĒĢ®ņĀü ĒÖśņ×É ĻĄÉņ£ĪņØä ĒåĄĒĢśņŚ¼ ĒÖśņ×É ņŖżņŖżļĪ£ ņ¦ĆņŗØņØä Ļ░¢ņČöļŖö Ļ▓āņØ┤ ļ░śļō£ņŗ£ ĒĢäņÜöĒĢśļŗż. ĻĘĖļ¤¼ļéś ņŗ¼ļ░®ņäĖļÅÖņ£╝ļĪ£ ņ╣śļŻīļ░øļŖö ĒÖśņ×ÉļōżņĪ░ņ░©ļÅä ņŚ¼ņĀäĒ׳ ņ¦łļ│æņŚÉ ļīĆĒĢ£ ņ¦ĆņŗØņØ┤ ļČĆņĪ▒ĒĢ£ Ļ▓āņØ┤ ĒśäņŗżņØ┤ļ®░[16], ļīĆĒĢ£ļČĆņĀĢļ¦źĒĢÖĒÜīņŚÉņä£ ņŗżņŗ£ĒĢ£ 2017ļģä ļīĆĻĄŁļ»╝ ļČĆņĀĢļ¦źņ¦łĒÖś ņØĖņŗØ ņĪ░ņé¼ ņé¼ņŚģņŚÉņä£ ņŗ¼ļ░®ņäĖļÅÖņŚÉ ļīĆĒĢ£ ņØĖņ¦Ćņ£©ņØĆ 10% ļ»Ėļ¦īņ£╝ļĪ£ ņ¦łĒÖśņŚÉ ļīĆĒĢ£ ĻĄÉņ£ĪņØ┤ ņŗ£ĻĖēĒĢ£ Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż. ņØ┤ņŚÉ ĒĢÖĒÜī ņĖĪņŚÉņä£ļŖö ņ¦łĒÖśņØś ņ£äĒŚśņØĖņ×É, Ļ┤ĆļĀ© ņ”ØņāüņØś ņØĖņ¦Ć, ņ╣śļŻī, ņ×ÉĻ░Ć Ļ┤Ćļ”¼ ļō▒ņØś ļé┤ņÜ®ņØä ĒżĒĢ©ĒĢśņŚ¼ ĒÖłĒÄśņØ┤ņ¦ĆņŚÉ Ļ░Ćņŗ£ņĀüņ£╝ļĪ£ ņĀĢļ│┤ļź╝ ņĀ£Ļ│ĄĒĢśĻ│Ā ļæÉĻĘ╝ļæÉĻĘ╝ ņ║ĀĒÄśņØĖ ļō▒ņØä ĒåĄĒĢśņŚ¼ ņØ╝ļ░śņØĖņØä ļīĆņāüņ£╝ļĪ£ ņØĖņ¦ĆļÅä Ē¢źņāüņØä ņ£äĒĢśņŚ¼ ļŗżĻ░üņĀü ļģĖļĀźņØä ĻĖ░ņÜĖņØ┤Ļ│Ā ņ׳ļŗż. ņ×ÉĻ░Ć Ļ┤Ćļ”¼ļŖö ņ╣śļŻī Ļ│╝ņĀĢņŚÉ ņל ņĀüņØæĒĢśĻ│Ā ĻĖłņŚ░ņØ┤ļéś ņ▓┤ņżæ ņĪ░ņĀł ļō▒ ņāØĒÖ£ ņŖĄĻ┤ĆņØä ļ│ĆĒÖöņŗ£ĒéżļŖö Ļ▓āņŚÉ ņØ╝ņ░©ņĀüņØĖ ļ¬®Ēæ£ļź╝ ļæÉļŖöļŹ░ ņØ┤ļź╝ ņ£äĒĢ┤ņä£ļŖö ņ╣śļŻī ļ░®ļ▓ĢņØ┤ļéś ļ¬®Ēæ£ņŚÉ ļīĆĒĢśņŚ¼ ĒÖśņ×É ņŖżņŖżļĪ£ ņל ņĢīĻ│Ā ņ׳ņ¢┤ņĢ╝ ĒĢ£ļŗż[17,18]. ņŗ¼ļ░®ņäĖļÅÖņØś ņ╣śļŻīņĀü ļ¬®Ēæ£ļŖö ļćīņĪĖņżæņØś ļ░£ņāØ ņ£äĒŚśņØä ļ¦ēĻ│Ā, Ļ┤ĆļĀ© ņ”ØņāüņØś ļ░£ĒśäņØä ņżäņØ┤ļ®░, ņŗ¼ĒśłĻ┤Ćņ¦łĒÖśņØś ļ░£ņāØņØä ņśłļ░®ĒĢśļŖöļŹ░ ņ׳ļŗż. ņØ┤ Ļ│╝ņĀĢņŚÉņä£ ņØśņé¼ļŖö ĒÖśņ×ÉņŚÉĻ▓ī ņ╣śļŻīņÖĆ Ļ┤ĆļĀ©ļÉ£ ĻĄ¼ņ▓┤ņĀüņØ┤Ļ│Ā ņĀĢĒÖĢĒĢ£ ņĀĢļ│┤ļź╝ ņĀ£Ļ│ĄĒĢśĻ│Ā, ĒÖśņ×ÉļŖö ņØ┤ņŚÉ ļīĆĒĢ£ ņČ®ļČäĒĢ£ ņØ┤ĒĢ┤ņÖĆ ņ×Éļ░£ņĀüņØĖ ņ╣śļŻīņØś ņ░ĖņŚ¼ļź╝ ĒåĄĒĢśņŚ¼ ļ│ĖņØĖņØś ņ¦łļ│æņŚÉ ļīĆĒĢ£ Ļ│ĄĒåĄņØś ņ▒ģņ×äņØśņŗØ(shared accountability)ņØä Ļ░Ćņ¦ĆļŖö Ļ▓āņØ┤ ņżæņÜöĒĢśļŗż[8,19,20].
ļŗżĒĢÖņĀ£ņĀü ņĀæĻĘ╝
ĒÖśņ×ÉņÖĆ ņ▓śņØī ņĀæĒĢśĻ▓ī ļÉśļŖö 1ņ░© ņØśļŻīņØĖ, ņŗ¼ņןļé┤Ļ│╝ ņĀäļ¼ĖņØś, ņŗ¼ĒśłĻ┤Ć ņÖĖĻ│╝ņØśņé¼, ļČĆņĀĢļ¦ź ņĀäļ¼ĖņØś, ļćīņĪĖņżæ ņĀäļ¼ĖņØśļź╝ ĒżĒĢ©ĒĢśļŖö ļŗżĒĢÖņĀ£ņĀü ņĀæĻĘ╝ņØĆ, ĒÖśņ×ÉĻ░Ć ņ╣śļŻīņŚÉ ņĀüĻĘ╣ņĀüņ£╝ļĪ£ ņ░ĖņŚ¼ĒĢĀ ņłś ņ׳ļÅäļĪØ ļÅäņÖĆņżä ņłś ņ׳ņ£╝ļ®░, ĒŖ╣Ē׳ ņ╣śļŻī Ļ▓░ņĀĢ ļŗ©Ļ│äņŚÉ ĒÖśņ×Éļź╝ ņ░ĖņŚ¼ņŗ£Ēé┤ņ£╝ļĪ£ņŹ© ĒÖśņ×ÉņØś ņ╣śļŻīņŚÉ ļīĆĒĢ£ ņł£ņØæļÅäļź╝ ļåÆņØ┤Ļ│Ā ņ╣śļŻī ĒÜ©Ļ│╝ļź╝ ļåÆņØ╝ ņłś ņ׳ļŗż[21,22]. ņĄ£ĻĘ╝ņŚÉļŖö ĒÖśņ×ÉņŚÉ ļīĆĒĢ£ ĻĄÉņ£Ī, ņ×ÉĻ░Ć Ļ┤Ćļ”¼ ļ░Å ņ╣śļŻī Ļ│╝ņĀĢ ņ░ĖņŚ¼ļź╝ ĒåĄĒĢ®ĒĢśļŖö ņ×äņāü ļ¬©ļŹĖņØ┤ ņĀ£ņŗ£ļÉśĻ│Ā ņ׳ņ£╝ļ®░ ņØ┤ļŖö ņŗ¼ļ░®ņäĖļÅÖņØś ņ╣śļŻīņŚÉ ņżæņÜöĒĢ£ Ļ░Ćņ╣śļź╝ ņ¦Ćļŗīļŗż[23]. ņØ┤ļĀćļō», ņŗ¼ļ░®ņäĖļÅÖņŚÉ ļīĆĒĢ£ ļŗżĒĢÖņĀ£ņĀü ņĀæĻĘ╝ņØĆ ņĀäļ¼ĖĒÖöļÉ£ ņØśĒĢÖņĀü ņ¦ĆņŗØļ┐Éļ¦ī ņĢäļŗłļØ╝, ĒÖśņ×ÉņÖĆ ņØśņé¼ ņé¼ņØ┤ņØś ņøÉĒÖ£ĒĢ£ ņØśņé¼ņåīĒåĄĻ│╝ ĻĄÉņ£ĪņØä ĒżĒĢ©ĒĢśļ®░, ņØ┤ Ļ│╝ņĀĢņŚÉņä£ ņØśņé¼ļź╝ ĒżĒĢ©ĒĢ£ ņĀäļ¼ĖĻ░ĆļōżņØś ņØśĒĢÖņĀü ņĪ░ņ¢Ėļ┐É ņĢäļŗłļØ╝, ļ╣äņØśļŻīņ¦äļōżņØś ĒÖśņ×ÉņŚÉ ļīĆĒĢ£ ņĀüĻĘ╣ņĀüņØĖ ĻĄÉņ£ĪĻ│╝ ĒśæņĪ░Ļ░Ć ĒĢäņÜöĒĢśļŗż.
1ņ░© ņØśļŻīņØĖņØś ņŚŁĒĢĀ
ņŗ¼ļ░®ņäĖļÅÖņØä ņ▓śņØī ņ¦äļŗ©ĒĢśĻ│Ā ņĀæĒĢśĻ▓ī ļÉśļŖö ņØ╝ņ░© ņØśļŻīņØĖņØś Ļ▓ĮņÜ░, ņŗ¼ļ░®ņäĖļÅÖņØś ņ▓½ ņ╣śļŻīņÖĆ ļćīņĪĖņżæņØś ņśłļ░®ņŚÉ Ļ┤ĆĒĢ£ ņØśĒĢÖņĀüņØĖ ņ¦ĆņŗØņØ┤ ĒĢäņÜöĒĢśļŗż. ņØ┤ Ļ│╝ņĀĢņŚÉņä£ ĒåĄĒĢ®ņĀüņØĖ ņŗ¼ļ░®ņäĖļÅÖņØś ņ╣śļŻīņĀü ņŗ£ņŖżĒģ£ņØĆ ņ▓śņØī ņØ╝ņ░© ņØśļŻīĻĖ░Ļ┤ĆņŚÉņä£ ņŗ¼ļ░®ņäĖļÅÖņŚÉ ļīĆĒĢ£ ņĀüņĀłĒĢ£ ņ▓½ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśĻ│Ā, ļČĆņĀĢļ¦ź ņĀäļ¼ĖĻ░ĆņŚÉĻ▓ī ņØśļó░ĒĢĀ ņłś ņ׳ļŖö ņ▓┤Ļ│äņĀüņØĖ ĻĖ░ļ░śņØä ņĀ£Ļ│ĄĒĢśĻ▓ī ļÉ£ļŗż[8,9,20].
ņØśļŻīņ¦äļōż Ļ░äņØś ņøÉĒÖ£ĒĢ£ ņØśņé¼ņåīĒåĄņØä ņ£äĒĢ£ ĻĖ░ņłĀņĀü ĒÖ£ņÜ®
ņŗ¼ļ░®ņäĖļÅÖņŚÉ Ļ┤ĆĒĢ£ ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīļź╝ ņ£äĒĢ┤ņä£ļŖö ĻĄ¼ņä▒ņøÉļōż Ļ░äņØś ņøÉĒÖ£ĒĢ£ ņØśņé¼ņåīĒåĄĻ│╝ ĻĄÉĒÖśņØ┤ ĒĢäņłśņĀüņØ┤ļŗż. ņØ┤ļź╝ ņ£äĒĢ┤ņä£ļŖö ĒÖśņ×ÉņÖĆ ņØśņé¼, ņØ╝ņ░© ņØśļŻīņØĖĻ│╝ ļČĆņĀĢļ¦ź ņĀäļ¼ĖĻ░Ć ņé¼ņØ┤ņØś ņ×Éņ£ĀļĪ£ņÜ┤ ņØśņé¼ ĻĄÉĒÖśņØä ņ£äĒĢ£ ĻĖ░ņłĀņĀü ņ¦ĆņøÉņØ┤ ĒĢäņÜöĒĢśļŗż. ņØ┤ Ļ│╝ņĀĢņŚÉņä£ ļööņ¦ĆĒäĖ ĒöäļĪ£ĻĘĖļשņØ┤ļéś ņŖżļ¦łĒŖĖĒÅ░ ņĢ▒ ļō▒ņØ┤ ļÅäņøĆņØä ņżä ņłś ņ׳ļŗż[24].
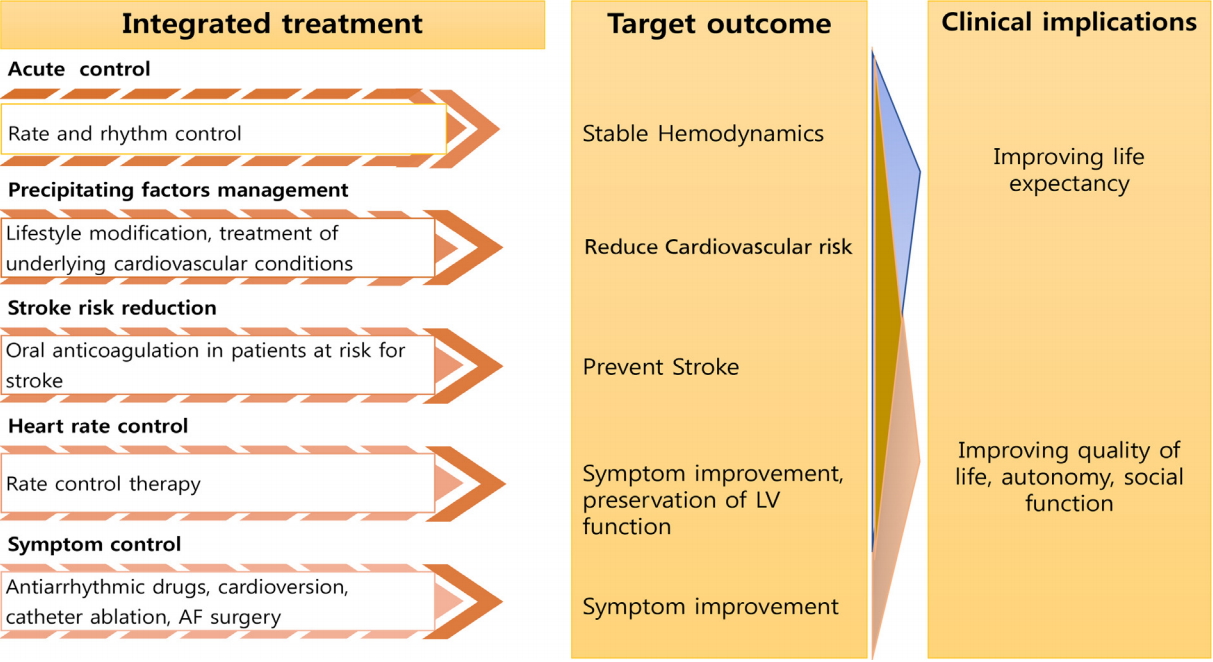
ņŗ¼ļ░®ņäĖļÅÖņŚÉ ļīĆĒĢ£ ĒåĄĒĢ®ņĀü ņ╣śļŻī ņĀüņÜ®
ņŗ¼ļ░®ņäĖļÅÖņŚÉ ļīĆĒĢ£ ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīļŖö ņØ┤ļźĖļ░ö ABC pathwayļĪ£ ņäżļ¬ģļÉśļŖöļŹ░, ļćīņĪĖņżæņØś ļ░£ņāØņØä Ēö╝ĒĢśĻ│Ā(Avoid stroke), Ļ┤ĆļĀ© ņ”ØņāüņØś ļ░£ņāØņØä ļ░®ņ¦ĆĒĢśļ®░(Better symptom management), ĻČüĻĘ╣ņĀüņ£╝ļĪ£ ņŗ¼ĒśłĻ┤Ćņ¦łĒÖśņØś ļ░£ņāØņØä ņżäņØ┤ĻĖ░(Cardiovascular and comorbidity risk reduction) ņ£äĒĢ£ Ļ▓āņØ┤ļŗż[25]. ņØ┤ļź╝ ņ£äĒĢ┤ņä£ļŖö ļ╣äļ¦ī, Ļ│ĀĒśłņĢĢ, ļŗ╣ļć©ņÖĆ Ļ░ÖņØĆ Ļ┤ĆļĀ© ņ¦łĒÖśņØś ņĀüĻĘ╣ņĀüņØĖ Ļ┤Ćļ”¼Ļ░Ć ņØ┤ļŻ©ņ¢┤ņĀĖņĢ╝ ĒĢśļ®░, ĒØĪņŚ░Ļ│╝ ņØīņŻ╝, ņÜ┤ļÅÖĻ│╝ Ļ░ÖņØĆ ņāØĒÖ£ņŖĄĻ┤Ć ĻĄÉņĀĢņØś ĻĄÉņĀĢņØ┤ ļÅÖņŗ£ņŚÉ ņØ┤ļŻ©ņ¢┤ņĀĖņĢ╝ ĒĢ£ļŗż(Table 2) [25-27].
ņŗ¼ļ░®ņäĖļÅÖņŚÉ ļīĆĒĢ£ ņ¦äļŗ©ņĀü ņĀæĻĘ╝
ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉņŚÉ ļīĆĒĢ£ ĒåĄĒĢ®ņĀü ĒÅēĻ░Ć
ņŗ¼ļ░®ņäĖļÅÖņØś ņ¢æņāü, ņ”Øņāü ļ░Å ņ£Āļ░£ ņÜöņØĖņŚÉ ļīĆĒĢ£ ļ¼Ėņ¦ä ļ░Å ļćīĻ▓ĮņāēņØä ĒżĒĢ©ĒĢ£ ņĀäņŗĀņāēņĀäņ”ØņØś Ļ│╝Ļ▒░ļĀźņŚÉ ļīĆĒĢ£ ĒÅēĻ░ĆĻ░Ć ņłśĒ¢ēļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż. ļŗ╣ļć©, Ļ│ĀĒśłņĢĢ, ļ¦īņä▒ĒÅÉņćäņä▒ĒÅÉņ¦łĒÖś, ļ╣äļ¦ī ļ░Å ņłśļ®┤ļ¼┤ĒśĖĒØĪņ”Ø, Ļ░æņāüņäĀĻĖ░ļŖźĒĢŁņ¦äĻ│╝ Ļ░ÖņØĆ ĻĖ░ņĀĆ ņ¦łĒÖś ļ░Å ņØīņŻ╝ļĀź Ēś╣ņØĆ ĒØĪņŚ░Ļ│╝ Ļ░ÖņØĆ ņāØĒÖ£ņŖĄĻ┤ĆņŚÉ ļīĆĒĢ£ ņ▓ĀņĀĆĒĢ£ ļ¼Ėņ¦äņØä ĒåĄĒĢśņŚ¼ ĻĄÉņĀĢ Ļ░ĆļŖźĒĢ£ ņøÉņØĖņØä ĒÅēĻ░ĆĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż[26-33]. ĻĄŁļé┤ ņĀä ĻĄŁļ»╝Ļ▒┤Ļ░ĢĻ▓Ćņ¦ä ņ×ÉļŻīņŚÉ ļīĆĒĢ£ Ēæ£ņżĆĒÖöļÉ£ ļŹ░ņØ┤Ēä░ļź╝ ĒåĄĒĢ£ ņ×ÉļŻī ļČäņäØņŚÉņä£ Ļ│ĀĒśłņĢĢņĀäļŗ©Ļ│ä, ļŗ╣ļć© ņĀäļŗ©Ļ│ä ĒÖśņ×ÉļōżņØś Ļ▓ĮņÜ░ ņāüņŖ╣ļÉ£ ĒśłņĢĢĻ│╝ Ļ│Ąļ│Ą Ēśłļŗ╣ļ¦īņ£╝ļĪ£ļÅä ņŗ¼ļ░®ņäĖļÅÖņØś ļ░£ņāØņØä ņ”ØĻ░Ćņŗ£ĒéżļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ņ£╝ļ®░[26], ļ╣äĻĄÉņĀü Ļ│ĀļÅä ļ╣äļ¦īņØ┤ ņĀüņØĆ ņĢäņŗ£ņĢä ĒÖśņ×ÉļōżņŚÉ ļīĆĒĢ£ ļČäņäØņŚÉņä£ļÅä ļ╣äļ¦īņØ┤ ļÅÖļ░śļÉĀ Ļ▓ĮņÜ░ ņŗ¼ļ░®ņäĖļÅÖņØś ļ░£ņāØņØ┤ ņ”ØĻ░ĆĒĢśĻ│Ā ņśłĒøäĻ░Ć ļéśņü£ Ļ▓āņ£╝ļĪ£ ņĪ░ņé¼ļÉśņŚłļŗż[27,34]. 12ņ£ĀļÅäņŗ¼ņĀäļÅäļź╝ ĒåĄĒĢśņŚ¼ ņŗ¼ņןņĀäļÅäņןņĢĀ, ĒŚłĒśłņä▒ņŗ¼ņ¦łĒÖś ļ░Å ĻĄ¼ņĪ░ņĀü ņŗ¼ņ¦łĒÖśņØś ņ£Āļ¼┤ļź╝ ĒÅēĻ░ĆĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż. Ļ▓ĮĒØēļČĆņŗ¼ņ┤łņØīĒīīļŖö ņŗ¼ļ░®ņäĖļÅÖņØś ņ╣śļŻī ļ░®ņ╣© Ļ▓░ņĀĢņØä ņ£äĒĢśņŚ¼ ļ¬©ļōĀ ĒÖśņ×ÉņŚÉĻ▓ī ņłśĒ¢ēļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż.
ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉņØś ņČöĻ░ĆņĀüņØĖ ņ¦äļŗ©ņĀü ļ░®ļ▓Ģ
ĒÖ£ļÅÖ ņżæ ņŗ¼ņĀäļÅäļŖö ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉņØś ļ¦źļ░Ģņłś ĒÅēĻ░Ć ļ░Å ņ”ØņāüĻ│╝ ņŗ¼ļ░®ņäĖļÅÖņØś Ļ┤ĆļĀ©ņä▒ņØä ĒÅēĻ░ĆĒĢśĻĖ░ņŚÉ ņ£ĀņÜ®ĒĢśļŗż. ĒŖ╣Ē׳ ĒÖ£ļÅÖ ņżæņŗ¼ņĀäļÅäĻ░Ć ņĀ£Ļ│ĄĒĢśļŖö ņÜ┤ļÅÖņØ┤ļéś ĒÖ£ļÅÖ ņżæņØś ļ¦źļ░ĢņłśņŚÉ ļīĆĒĢ£ ņĀĢļ│┤ļŖö ņĢĮļ¼╝ ņ╣śļŻīļź╝ ĒåĄĒĢ£ ļ¦źļ░Ģņłś ņĪ░ņĀłņØś ļ¬®Ēæ£Ļ░Ć ļŗ¼ņä▒ļÉśņŚłļŖöņ¦Ćļź╝ ĒÖĢņØĖĒĢśļŖöļŹ░ ņØ┤ņÜ®ļÉĀ ņłś ņ׳ļŗż. Ļ▓ĮņŗØļÅäņŗ¼ņ┤łņØīĒīīļŖö Ļ▓ĮĒØēļČĆņŗ¼ņ┤łņØīĒīīņŚÉ ļ╣äĒĢśņŚ¼ ņóīņŗ¼ļ░®ņØ┤ņØś ĻĖ░ļŖź ĒÅēĻ░Ć ļ░Å ņóīņŗ¼ļ░®ņØ┤ ļé┤ņØś ĒśłņĀä ņ£Āļ¼┤ ĒÅēĻ░ĆņŚÉ ņ£ĀņÜ®ĒĢśļŗż. ļö░ļØ╝ņä£ ņ╣©ņŖĄņĀüņØĖ ņ╣śļŻīņØĖ ļÅÖņ£©ļÅÖņĀäĒÖśņłĀņØ┤ļéś Ļ│ĀņŻ╝ĒīīņĀłņĀ£ņłĀņØä ņĢ×ļæö ĒÖśņ×ÉņŚÉņä£ Ļ▓ĮņŗØļÅäņ┤łņØīĒīīļź╝ ĒåĄĒĢ£ ņŗ¼ņןļé┤ ĒśłņĀäņØś ĒÅēĻ░ĆļŖö ĒĢäņłśņĀüņØ┤ļŗż(Table 3) [35,36]. ļćīĻ▓ĮņāēņØ┤ ņØśņŗ¼ļÉśļŖö ĒÖśņ×ÉļŖö ļćī ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśü Ēś╣ņØĆ ļćī ņ×ÉĻĖ░Ļ│Ąļ¬ģņśüņāüņØä ņØ┤ņÜ®ĒĢśņŚ¼ ļćīĻ▓Įņāē ņ£Āļ¼┤ļź╝ ĒÅēĻ░ĆĒĢśņŚ¼ņĢ╝ ĒĢśļ®░, ņØ┤ļź╝ ĒåĄĒĢśņŚ¼ ļćīĻ▓ĮņāēņØś ĻĖēņä▒ĻĖ░ ņ╣śļŻī ļ░Å ĒĢŁņØæĻ│ĀņĀ£ ņ╣śļŻī ļ░®ņ╣©ņØä ņłśļ”ĮĒĢśļŖöļŹ░ ļÅäņøĆņØä ļ░øņØä ņłś ņ׳ļŗż.
ņ▓┤Ļ│äņĀüņØ┤Ļ│Ā ļ¬®Ēæ£-ĻĘ╝Ļ▒░ ņżæņŗ¼ņØś ņČöņĀü Ļ┤Ćņ░░(goal-based follow-up)
ļīĆļČĆļČäņØś ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉļōżņØĆ ņ¦ĆņåŹņĀüņØĖ ņĄ£ņĀüņØś ņ╣śļŻīļź╝ ņ£äĒĢśņŚ¼ ņĀĢĻĖ░ņĀüņØĖ ņČöņĀü Ļ┤Ćņ░░ņØ┤ ĒĢäņÜöĒĢśļŗż. ņČöņĀü Ļ┤Ćņ░░ņØĆ ņØ╝ņ░© ņ¦äļŻī, ņŗ¼ņןļé┤Ļ│╝ ņĀäļ¼ĖņØś ļśÉļŖö ļČĆņĀĢļ¦ź ņĀäļ¼ĖņØśņŚÉĻ▓ī ļ░øņØä ņłś ņ׳ņ£╝ļ®░, ņČöņĀü Ļ┤Ćņ░░ ļÅÖņĢł ņ╣śļŻī Ļ│äĒÜŹņØś ņłśĒ¢ē, ĒÖśņ×ÉņØś ņ¦ĆņåŹņĀüņØĖ ņ░ĖņŚ¼ ĻĘĖļ”¼Ļ│Ā ĒĢäņÜöĒĢĀ Ļ▓ĮņÜ░ ņ╣śļŻīņØś ļ│ĆĻ▓ĮņØ┤ ĒĢäņÜöĒĢśļŗż. ņŗ¼ļ░®ņäĖļÅÖņØś ņ╣śļŻīļŖö ņśłĒøäņÖĆ Ļ┤ĆļĀ©ļÉ£ ņ╣śļŻī(ĒĢŁņØæĻ│Ā ņ╣śļŻī ļ░Å ņŗ¼ĒśłĻ┤Ćņ¦łĒÖśņØś ņ╣śļŻī)ņÖĆ ņ”ØņāüņØä ņÖäĒÖöņŗ£ĒéżļŖö ņ╣śļŻī(ņŗ¼ļ░Ģņłś ļśÉļŖö ņŗ¼ņ£©ļÅÖ ņĪ░ņĀł; Table 4)ļź╝ ĒżĒĢ©ĒĢ£ļŗż[25,37]. ņśłĒøäļź╝ Ē¢źņāüņŗ£ĒéżļŖö ņ╣śļŻīņŚÉ ļīĆĒĢ┤ņä£ļŖö ņ╣śļŻīņØś ņØ┤ļōØņŚÉ ļīĆĒĢśņŚ¼ ņ¦üņĀæņĀüņ£╝ļĪ£ ļŖÉļéä ņłś ņŚåņ£╝ļ»ĆļĪ£ ĒÖśņ×ÉņŚÉĻ▓ī ņČ®ļČäĒ׳ ņØ┤ĒĢ┤ĒĢĀ ņłś ņ׳ļÅäļĪØ ņØ┤ņŚÉ ļīĆĒĢ£ ņŻ╝ņØś Ļ╣ŖņØĆ ņäżļ¬ģņØ┤ ĒĢäņÜöĒĢśļŗż. ļśÉĒĢ£ ņŗ¼ņ£©ļÅÖ ņĪ░ņĀł ņ╣śļŻīļŖö ņŗ¼ļ░®ņäĖļÅÖņØ┤ ņØ╝ļČĆ ņ×¼ļ░£ĒĢśļŹöļØ╝ļÅä ņĀäļ░śņĀüņØĖ ļ╣łļÅäļéś ĻĖ░Ļ░ä ļō▒ņØ┤ Ļ░ÉņåīĒĢśņŚ¼ ņ”ØņāüņØ┤ ņĪ░ņĀłļÉśņŚłļŗżļ®┤ ņä▒Ļ│ĄņØ┤ļØ╝ ĒĢĀ ņłś ņ׳ļŗż. ĻĘĖļ”¼Ļ│Ā ņ╣śļŻīļź╝ ņŗ£ņ×æĒĢĀ ļĢī Ļ░£ļ│ä ĒÖśņ×Éļ¦łļŗż ņśłņāüļÉśļŖö ņØ┤ļōØņØä ņäżļ¬ģĒĢśļŖö Ļ▓āņØ┤ ĻĘ╝Ļ▒░ ņŚåļŖö ĻĖ░ļīĆļź╝ ļ░®ņ¦ĆĒĢśĻ│Ā ņéČņØś ņ¦łņØä ņĄ£ņĀüĒÖöĒĢśļŖöļŹ░ ļÅäņøĆņØ┤ ļÉ£ļŗż. ĻĘĖļ”¼Ļ│Ā ņŗ¼ļ░®ņäĖļÅÖĻ│╝ Ļ┤ĆļĀ©ĒĢśņŚ¼ ļÅÖļ░śļÉ£ ņ¦łĒÖśļōż(ļ╣äļ¦ī, Ļ│ĀĒśłņĢĢ, ņŗ¼ļČĆņĀä, ļŗ╣ļć©, ņłśļ®┤ļ¼┤ĒśĖĒØĪ)ņŚÉ ļīĆĒĢ£ ņ▓ĀņĀĆĒĢ£ Ļ┤Ćļ”¼Ļ░Ć ņäĀĒ¢ēļÉśņ¢┤ņĢ╝ ĒĢśļ®░[26,29,34,38,39], ĒØĪņŚ░, ņØīņŻ╝, ņÜ┤ļÅÖņŖĄĻ┤ĆĻ│╝ Ļ░ÖņØĆ ņāØĒÖ£ņŖĄĻ┤ĆņŚÉ ļīĆĒĢ£ ĻĄÉņĀĢļÅä ĒåĄĒĢ®ņĀüņ£╝ļĪ£ ņČöņĀü Ļ┤Ćņ░░ļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż[4,6].
Ļ▓░ ļĪĀ
ņŗ¼ļ░®ņäĖļÅÖņŚÉ ļīĆĒĢ£ ĒåĄĒĢ®ņĀüņØĖ ņ╣śļŻīļź╝ ņ£äĒĢ┤ņä£ļŖö ĒÖśņ×ÉĻ░Ć ļ│æņŚÉ ļīĆĒĢ£ ĻĖ░ļ│ĖņĀüņØĖ ņ¦ĆņŗØņØä Ļ░Ćņ¦ĆĻ│Ā ņĀüĻĘ╣ņĀüņ£╝ļĪ£ ņ╣śļŻīņØś ņżæņŗ¼ņŚÉ ņä£ņĢ╝ ĒĢ£ļŗż. ņØ┤ Ļ│╝ņĀĢņŚÉņä£ ņØśņé¼ļōżņŚÉ ņØśĒĢ£ ņĀäļ¼ĖņĀüņØĖ ņ¦ĆņŗØņØ┤, ĒÖśņ×ÉņÖĆ ņØśņé¼ ņé¼ņØ┤ņØś ņØśņé¼ņåīĒåĄĻ│╝ ĻĄÉņ£ĪņØä ĒåĄĒĢśņŚ¼ ĒÖśņ×ÉņŚÉĻ▓ī ņøÉĒÖ£ĒĢśĻ▓ī ņĀäļŗ¼ļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż. ĒÖśņ×Éļź╝ ņ▓śņØī ņĀæĒĢśĻ▓ī ļÉśļŖö 1ņ░© ņ¦äļŻīņØśņØś ņ¦äļŗ©ļČĆĒä░, ņ╣śļŻī ĻĘĖļ”¼Ļ│Ā ņ▓┤Ļ│äņĀüņØĖ ņČöņĀü Ļ┤Ćņ░░ņŚÉ ņØ┤ļź┤ĻĖ░Ļ╣īņ¦Ć ļŗ©Ļ│äņĀüņØ┤Ļ│Ā ĒåĄĒĢ®ņĀüņØĖ ņŗ¼ļ░®ņäĖļÅÖ Ļ┤Ćļ”¼ļŖö ņ¦łļ│æņØś ņ╣śļŻīņŚÉ ņ׳ņ¢┤ņä£ ļČĆņ×æņÜ®ņØä ņĄ£ņåīĒÖöĒĢśĻ│Ā, ļ│æņŚÉ ļīĆĒĢ£ ĒÖśņ×ÉļōżņØś ņØĖņ¦ĆļÅäļź╝ ļåÆņŚ¼ ņ╣śļŻī ņä▒Ļ│╝ļź╝ Ē¢źņāüņŗ£Ēé¼ Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






