


м„ң лЎ
м—°н•ҳкіӨлһҖмқҖ мӢқлҸ„нҳ‘м°©, м•”, мӢқлҸ„ 연축, н”јл¶ҖкІҪнҷ”мҰқ, мӢқлҸ„ мқҙмҷ„л¶ҲлҠҘмҰқ л“ұ м—¬лҹ¬ к°Җм§Җ мӣҗмқём—җ мқҳн•ҙ лӮҳнғҖлӮ мҲҳ мһҲлӢӨ[1]. Kommerell кІҢмӢӨмқҖ к·јмң„л¶Җ н•ҳн–үлҢҖлҸҷл§Ҙмқҳ нҷ•мһҘмқҙ нҠ№м§•мқё лҢҖлҸҷл§Ҙ к¶Ғмқҳ м„ мІңм„ұ мқҙмғҒмңјлЎң мқҙмғҒ мҮ„кіЁн•ҳлҸҷл§Ҙмқҙ лҸҷл°ҳлҗ мҲҳ мһҲлӢӨ[2]. л¬ҙмҰқмғҒмқј мҲҳ мһҲмңјлӮҳ кІҢмӢӨмқҙ мў…кІ©лҸҷ кө¬мЎ°л¬јмқё мӢқлҸ„лӮҳ кё°лҸ„ л“ұмқ„ м••л°•н•ЁмңјлЎңмҚЁ м—°н•ҳкіӨлһҖмқҙлӮҳ нҳёнқЎкіӨлһҖ л“ұмқҳ мҰқмғҒмқҙ лҸҷл°ҳлҗ мҲҳ мһҲмңјл©°, лҢҖлҸҷл§Ҙ л°•лҰ¬лӮҳ кІҢмӢӨмқҳ нҢҢм—ҙкіј к°ҷмқҖ м№ҳлӘ…м Ғмқё н•©лі‘мҰқмңјлЎң лӮҳнғҖлӮ мҲҳлҸ„ мһҲлӢӨ[3,4]. м Җмһҗл“ӨмқҖ мҡ°мёЎ лҢҖлҸҷл§Ҙ к¶Ғм—җм„ң лҸҷл°ҳлҗң Kommerell кІҢмӢӨмқҙ мӢқлҸ„лҘј м••л°•н•ҳм—¬ м—°н•ҳкіӨлһҖ л°Ҹ м—°н•ҳнҶөмңјлЎң л°ңнҳ„лҗң л“ңл¬ё мҰқлЎҖлҘј кІҪн—ҳн•ҳмҳҖкё°м—җ л¬ён—Ңкі м°°кіј н•Ёк»ҳ ліҙкі н•ҳлҠ” л°”мқҙлӢӨ.
ліё лЎ
23м„ё лӮЁмһҗк°Җ м—°н•ҳкіӨлһҖкіј м—°н•ҳнҶөмңјлЎң лӮҙмӣҗн•ҳмҳҖлӢӨ. м–ҙлҰҙ л•Ңл¶Җн„° мӢқмӮ¬н• л•Ңл§ҲлӢӨ м—°н•ҳнҶөкіј м—°н•ҳкіӨлһҖмқҙ мһҲм—ҲмңјлӮҳ л¬јмқ„ л§ҲмӢңл©ҙ нҳём „лҗҳм–ҙ нҠ№лі„н•ң кІҖмӮ¬лӮҳ м№ҳлЈҢ м—Ҷмқҙ м§ҖлӮҙлӢӨк°Җ кө° мӢ мІҙкІҖ진м—җм„ң м°ҚмқҖ нқүл¶Җ лӢЁмҲңмҙ¬мҳҒм—җм„ң нҸҗл¬ёмқҳ мқҙмғҒмҶҢкІ¬мқҙ ліҙм—¬ мқҙм—җ лҢҖн•ң нҸүк°ҖлҘј мң„н•ҙ м „мӣҗ лҗҳм—ҲлӢӨ. кіјкұ°л ҘмқҙлӮҳ к°ҖмЎұл Ҙм—җм„ң нҠ№мқҙмӮ¬н•ӯмқҖ м—Ҷм—ҲлӢӨ. нҷңл Ҙ 징нӣ„лҠ” нҳҲм•• 120/80 mmHg, л§Ҙл°• 79нҡҢ/분, нҳёнқЎмҲҳ 20нҡҢ/분, мІҙмҳЁ 36.4в„ғмҳҖлӢӨ. мӢ¬мқҢмқҙлӮҳ нҳёнқЎмқҢмқ„ нҸ¬н•Ён•ң мӢ мІҙ кІҖ진м—җм„ң нҠ№мқҙмҶҢкІ¬мқҙ кҙҖм°°лҗҳм§Җ м•Ҡм•ҳлӢӨ. лӮҙмӣҗн•ҳм—¬ мӢңн–үн•ң к°„кё°лҠҘ, мӢ кё°лҠҘ, нҳҲкө¬ кІҖмӮ¬лҘј нҸ¬н•Ён•ң нҳҲм•Ў кІҖмӮ¬лҠ” лӘЁл‘җ м •мғҒмқҙм—Ҳмңјл©°, мҶҢліҖ кІҖмӮ¬лҸ„ м •мғҒмқҙм—ҲлӢӨ.
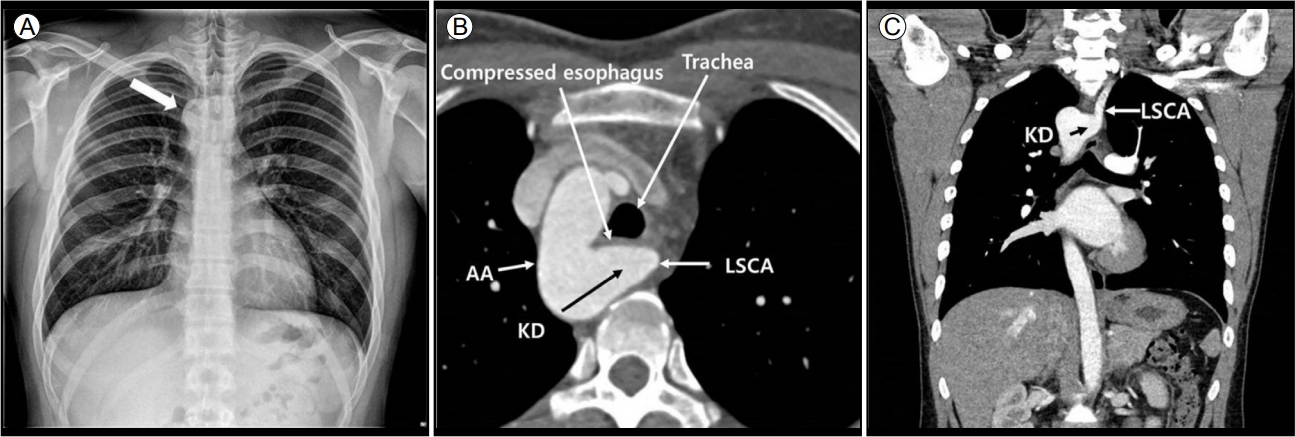
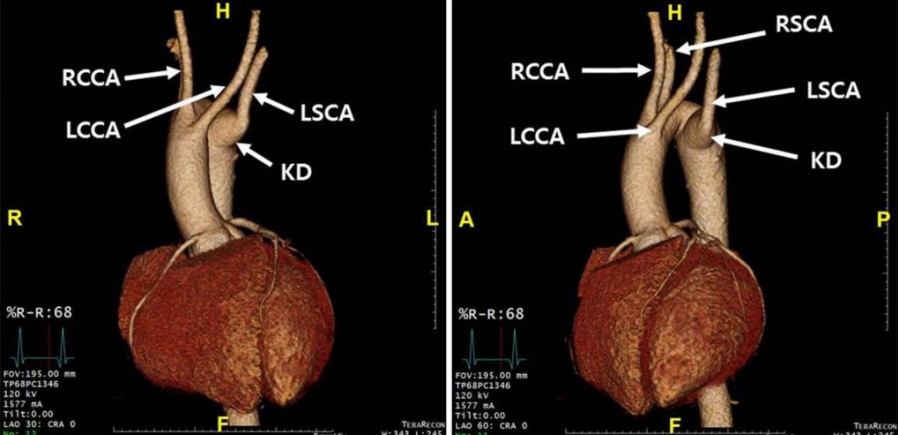
мӢ¬м „лҸ„лҠ” м •мғҒ лҸҷмңЁлҸҷмқҙм—Ҳкі , нқүл¶Җ лӢЁмҲңмҙ¬мҳҒм—җм„ң мҡ°мёЎ лҢҖлҸҷл§Ҙ к¶Ғмқҙ кҙҖм°°лҗҳм—ҲлӢӨ(Fig. 1A), м—°н•ҳкіӨлһҖмқҳ нҸүк°ҖлҘј мң„н•ҙ мӢңн–үн•ң мғҒл¶Җ мң„мһҘкҙҖ лӮҙмӢңкІҪм—җм„ң мғҒл¶Җ мӢқлҸ„к°Җ л°•лҸҷм„ұ кө¬мЎ°л¬јм—җ мқҳн•ң мҷёл¶Җ м••л°•мңјлЎң лӮҙк°•мқҙ мўҒм•„м ё мһҲлҠ” кІғмқҙ кҙҖм°°лҗҳм—ҲлӢӨ. мҡ°мёЎ лҢҖлҸҷл§Ҙ к¶Ғкіј мӢқлҸ„мқҳ мҷёл¶Җ м••л°•м—җ мқҳн•ң нҳ‘м°© нҸүк°ҖлҘј мң„н•ҙ мӢңн–үн•ң нқүл¶Җ мЎ°мҳҒ мҰқк°• м „мӮ°нҷ”лӢЁмёөмҙ¬мҳҒ(computed tomography, CT)м—җм„ң мҡ°мёЎ лҢҖлҸҷл§Ҙ к¶Ғкіј мҡ°мёЎ н•ҳн–үлҢҖлҸҷл§Ҙмқҳ к·јмң„л¶Җм—җм„ң м§ҒкІҪ 46 mm м •лҸ„лЎң нҷ•мһҘлҗң нҳҲкҙҖ(Kommerell кІҢмӢӨ)мқҙ кҙҖм°°лҗҳм—Ҳкі , мўҢмҮ„кіЁн•ҳлҸҷл§Ҙмқҙ мқҙ Kommerell кІҢмӢӨм—җм„ң кё°мӢңн•ҳлҠ” кІғмқ„ м•Ң мҲҳ мһҲм—ҲлӢӨ. лҳҗн•ң мӢқлҸ„к°Җ Kommerell кІҢмӢӨ л°Ҹ Kommerell кІҢмӢӨм—җм„ң мқҙмғҒм ҒмңјлЎң кё°мӢңн•ҳлҠ” мўҢмҮ„кіЁн•ҳлҸҷл§Ҙм—җ мқҳн•ҙ кё°кҙҖкіјмқҳ мӮ¬мқҙм—җм„ң мӢ¬н•ҳкІҢ лҲҢл Ө мһҲлҠ” кІғмқҙ кҙҖм°°лҗҳм—ҲлӢӨ(Fig. 1B, C). нҳҲкҙҖмқҳ кө¬мЎ°кё°мӢңн•ҳм§Җ м•Ҡкі к°Ғк°Ғ кё°мӢңн•ҳлҠ” кІғмқҙ кҙҖм°°лҗҳм—ҲлӢӨ(Fig. 2). мӢқлҸ„мЎ°мҳҒ кІҖмӮ¬м—җм„ң лҢҖлҸҷл§Ҙ к¶Ғ мң„м№ҳм—җм„ң мғҒл¶Җ мӢқлҸ„к°Җ мҷёл¶Җ м••л°•м—җ мқҳн•ҙ лӮҙк°•мқҙ мӢ¬н•ҳкІҢ мўҒ아진 кІғмқҙ кҙҖм°°лҗҳм—ҲлӢӨ(Fig. 3A, Supplement Video 1).
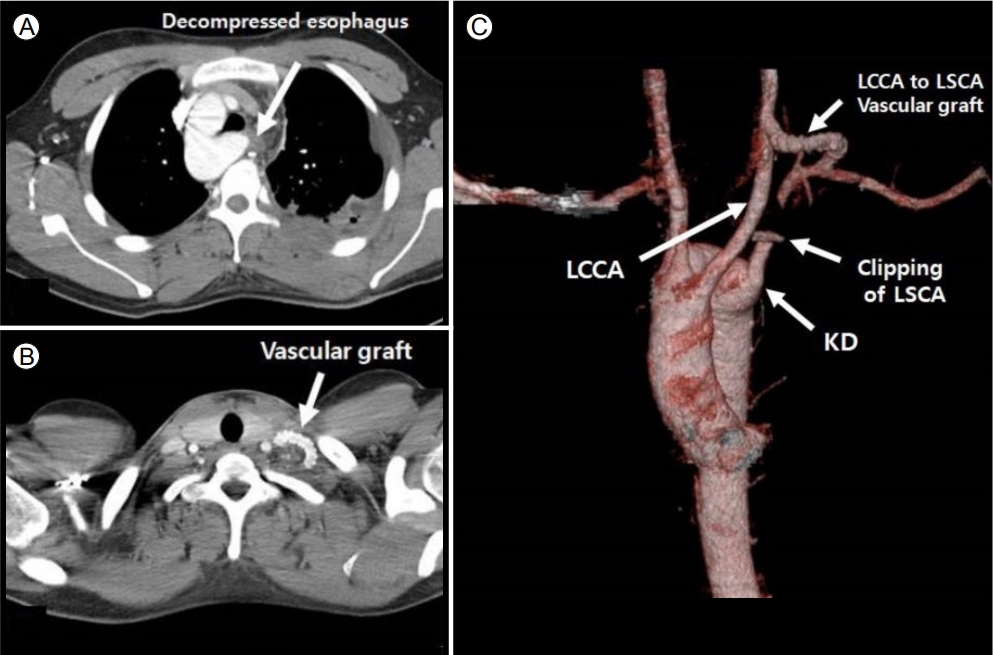
м—°н•ҳнҶөкіј м—°н•ҳкіӨлһҖмқҳ мӣҗмқёмқҙ Kommerell кІҢмӢӨм—җ мқҳн•ң мӢқлҸ„ м••л°•мқҳ мҰқмғҒмңјлЎң нҢҗлӢЁлҗҳм–ҙ нҷҳмһҗлҠ” мҲҳмҲ м Ғ м№ҳлЈҢлҘј мӢңн–ү л°ӣм•ҳлӢӨ. мҲҳмҲ мҶҢкІ¬м—җм„ң мӢқлҸ„к°Җ Kommerell кІҢмӢӨкіј Kommrell кІҢмӢӨм—җм„ң л№„м •мғҒмңјлЎң кё°мӢңн•ң мўҢмҮ„кіЁн•ҳлҸҷл§Ҙ л°Ҹ лҸҷл§ҘмқёлҢҖ(ligamentumaretriosum) мӮ¬мқҙм—җм„ң мҷёл¶Җ м••л°•м—җ мқҳн•ҙ мӢ¬н•ң нҳ‘м°©мқҙ л°ңмғқн•ң кІғмқ„ нҷ•мқён•ҳмҳҖлӢӨ. лҸҷл§ҘмқёлҢҖ м Ҳм ңн•ҳмҳҖмқ„ л•Ң мӢқлҸ„мқҳ м••л°•м—җ мқҳн•ң нҳ‘м°©мқҖ нҳём „лҗҳм—Ҳмңјл©°, к·јмң„л¶Җ мўҢмҮ„кіЁн•ҳлҸҷл§Ҙмқ„ кІ°м°°н•ҳкі (Fig. 4A), мўҢмҮ„кіЁн•ҳлҸҷл§Ҙмқ„ мўҢмҙқкІҪлҸҷл§Ҙм—җ 6 mm нҒ¬кё°мқҳ мқҙмӢқнҳҲкҙҖ(vascular graft)мқ„ мқҙмҡ©н•ҳм—¬ м—°кІ°н•ҳмҳҖлӢӨ(Fig. 4B, C).
мҲҳмҲ нӣ„ мӢңн–үн•ң мӢқлҸ„мЎ°мҳҒ кІҖмӮ¬м—җм„ң мҷёл¶Җ м••л°•м—җ мқҳн•ң мӢқлҸ„ нҳ‘м°©мқҙ м—Ҷмқҙ мЎ°мҳҒм ңк°Җ мһҳ нҶөкіјн•ҳлҠ” кІғмқ„ кҙҖм°°н• мҲҳ мһҲм—ҲлӢӨ(Fig. 3B, Supplement Video 2). нҷҳмһҗк°Җ мӢқмӮ¬н• л•Ңл§ҲлӢӨ л°ңмғқн•ҳлҚҳ м—°н•ҳкіӨлһҖкіј м—°н•ҳнҶөлҸ„ нҳём „лҗҳм–ҙ мҷёлһҳ кІҪкіј кҙҖм°° мӨ‘мқҙлӢӨ.
кІ° лЎ
кё°нҳ•м„ұ м—°н•ҳкіӨлһҖмқҖ н•ҳн–үлҢҖлҸҷл§ҘмңјлЎңл¶Җн„° мӢңмһ‘н•ҙм„ң мӢқлҸ„мқҳ нӣ„л°©мқ„ нҶөн•ҳлҠ” мқҙмғҒ мҮ„кіЁн•ҳлҸҷл§Ҙм—җ мқҳн•ҙ мӢқлҸ„к°Җ м••л°•лҗҳм–ҙ мқјм–ҙлӮҳлҠ” м—°н•ҳкіӨлһҖмңјлЎң 1794л…„ Bayford [5]м—җ мқҳн•ҙ мІҳмқҢ ліҙкі лҗҳм—ҲлӢӨ. мҡ°мёЎ мқҙмғҒ мҮ„кіЁн•ҳлҸҷл§ҘмқҖ м „мІҙ мқёкө¬мқҳ 0.5%, мўҢмёЎ мқҙмғҒ мҮ„кіЁн•ҳлҸҷл§ҘмқҖ 0.06%м—җм„ң 0.01% м •лҸ„ л°ңмғқн•ңлӢӨ[6]. лӮҙмӢңкІҪмҙҲмқҢнҢҢлҘј мқҙмҡ©н•ң м—°кө¬м—җм„ң м—°н•ҳкіӨлһҖ нҷҳмһҗмқҳ 0.36%м—җм„ң мқҙмғҒ мҮ„кіЁн•ҳлҸҷл§Ҙмқҙ мһҲлҠ” кІғмңјлЎң ліҙкі лҗң л°” мһҲлӢӨ[7]. Kommerell кІҢмӢӨмқҖ лҢҖлҸҷл§Ҙ к¶Ғмқҳ лҸҷл§Ҙ нҷ•мһҘмқҙ нҠ№м§•мқё л“ңл¬ё нҳҲкҙҖ кё°нҳ•мңјлЎң 1937л…„ Burckhard F. Kommerellм—җ мқҳн•ҙ мІҳмқҢ ліҙкі лҗҳм—Ҳмңјл©°, мўҢмёЎ лҢҖлҸҷл§Ҙ к¶Ғм—җ мқҙмғҒ мҡ°мҮ„кіЁн•ҳлҸҷл§Ҙмқ„ к°Җ진 нҷҳмһҗмҳҖлӢӨ[2]. л°°м•„м—җм„ң 6мҢҚмқҳ лҢҖлҸҷл§Ҙ к¶Ғмқҙ кё°кҙҖнҳ•м„ұ лӢЁкі„м—җм„ң л°ңмғқн•ҳлҠ”лҚ°, 4лІҲ мӣҗмӢң лҢҖлҸҷл§Ҙ к¶Ғмқҙ м„ұмқё лҢҖлҸҷл§Ҙ к¶Ғмқ„ нҳ•м„ұн•ңлӢӨ. мҡ°мёЎ 4лІҲм§ёк°Җ мқјл°ҳм ҒмңјлЎң мӮ¬лқјм§Җкі мўҢмёЎм—җ м•„м№ҳнҳ•мқ„ мқҙлЈЁлҠ” м •мғҒм Ғмқё лҢҖлҸҷл§Ҙ мЈјн–үмқҙ мғқкё°кІҢ лҗҳлҠ”лҚ°, мўҢмёЎмқҙ мӮ¬лқјм§Җкі мҡ°мёЎмқҙ лӮЁкІҢ лҗҳл©ҙ мҡ°мёЎ лҢҖлҸҷл§Ҙ к¶Ғмқҙ л°ңмғқн•ҳкІҢ лҗңлӢӨ[3]. EdwardsлҠ” мҡ°мёЎ лҢҖлҸҷл§Ҙ к¶Ғмқ„ 3к°Җм§Җ мң нҳ•мңјлЎң 분лҘҳн•ҳмҳҖлӢӨ. мІ« лІҲм§ёлҠ” мЈјмҡ” лҸҷл§Ҙмқҳ кұ°мҡё мғҒ 분기лЎң 59% м •лҸ„ лӮҳнғҖлӮҳл©°, л‘җ лІҲм§ёлҠ” мқҙмғҒ мўҢмҮ„кіЁн•ҳлҸҷл§Ҙмқҙ мһҲлҠ” кІғмңјлЎң 39.5%, м„ё лІҲм§ёлҠ” 분лҰ¬лҗң мўҢмҮ„кіЁн•ҳлҸҷл§Ҙмқҙ мһҲлҠ” кІғмңјлЎң 0.8%к°Җ лӮҳнғҖлӮңлӢӨ[8]. кІҢмӢӨмқҖ мўҢмёЎ лҢҖлҸҷл§Ҙ к¶Ғкіј мҡ°мёЎ лҢҖлҸҷл§Ҙк¶Ғ лӘЁл‘җм—җм„ң л°ңмғқн• мҲҳ мһҲмңјл©°, мқҙлЎңл¶Җн„° мқҙмғҒ мҮ„кіЁн•ҳлҸҷл§Ҙмқҙ л°ҳлҢҖмӘҪмңјлЎң мҳ¬лқјк°ҖкІҢ лҗңлӢӨ. л¬ҙмҰқмғҒмңјлЎң м§ҖлӮј мҲҳлҸ„ мһҲмңјл©°, кІҢмӢӨм—җ мқҳн•ң мў…кІ©лҸҷмқҳ кө¬мЎ°л¬ј м••л°•мңјлЎң мқён•ҙ мҰқмғҒмқҙ лӮҳнғҖлӮ мҲҳ мһҲлӢӨ. мҶҢм•„ нҷҳмһҗм—җм„ңлҠ” кё°лҸ„мқҳ м••л°• мҰқмғҒмқҙ мў…мў… лӮҳнғҖлӮ мҲҳ мһҲкі , м—°н•ҳкіӨлһҖкіј к°ҖмҠҙ л¶ҲнҺёк°җмқҖ м„ұмқё нҷҳмһҗм—җм„ң лҚ” нқ”н•ҳлӢӨ. м„ұмқёкё°м—җ нҳҲкҙҖмқҳ мЈҪмғҒ кІҪнҷ”м„ұ ліҖнҷ”, лҸҷл§ҘлҘҳ нҢҪлҢҖлЎң мқён•ҙ мЈјліҖ кө¬мЎ°л¬јмқҳ м••л°•мңјлЎң м—°н•ҳкіӨлһҖ, мІңлӘ…мқҢ, кё°м№Ё, мһ¬л°ңм„ұ нҸҗл ҙ, к°ҖмҠҙ нҶөмҰқмқҙ лӮҳнғҖлӮ мҲҳ мһҲмңјл©° лҸҷл§ҘлҘҳмқҳ нҢҢм—ҙ, лҢҖлҸҷл§Ҙ л°•лҰ¬ л“ұмқҙ н•©лі‘мҰқмңјлЎң лӮҳнғҖлӮ мҲҳ мһҲлӢӨ[3,4]. лҢҖлҸҷл§Ҙ к¶Ғ кё°нҳ•мқҖ нҢ”лЎңмӮ¬м§•мҰқ, нҸҗлҸҷл§Ҙ нҳ‘м°©мҰқ, мӮјмІңнҢҗ нҸҗмҮ„ л“ұмқҳ лӢӨм–‘н•ң м„ мІңм„ұ мӢ¬мһҘ кё°нҳ•кіј м—°кҙҖлҗҳм–ҙ мһҲлӢӨ[3,9]. лҢҖлҸҷл§Ҙ к¶Ғ кё°нҳ•мқҙ мһҲмқ„ кІҪмҡ°, м„ мІңм„ұ мӢ¬м§Ҳнҷҳмқҙ мһҲлҠ”м§Җ мһҳ мӮҙнҺҙліҙм•„м•ј н•ҳкІ лӢӨ. лҢҖлҸҷл§Ҙ к¶Ғмқҳ нҳҲкҙҖ мқҙмғҒмқҖ нқүл¶Җ Xм„ , лӮҙмӢңкІҪ, мӢқлҸ„ мЎ°мҳҒмҲ , мӢ¬мҙҲмқҢнҢҢ, мһҗкё°кіөлӘ…мҳҒмғҒ(magnetic resonance imaging) л°Ҹ м»ҙн“Ён„° лӢЁмёө мҙ¬мҳҒ нҳҲкҙҖ мЎ°мҳҒмҲ мқ„ нҸ¬н•Ён•ң лӢӨм–‘н•ң мҳҒмғҒ 진лӢЁмңјлЎң н• мҲҳ мһҲлӢӨ[10]. мҲҳмҲ мқҳ м Ғмқ‘мҰқмқҙ лӘ…нҷ•н•ҳкІҢ нҷ•лҰҪлҗҳм§ҖлҠ” м•Ҡм•ҳмңјлӮҳ, кё°лҸ„лӮҳ мӢқлҸ„мқҳ м••л°• мҰқмғҒмқҙ мһҲкұ°лӮҳ, л¬ҙмҰқмғҒ нҷҳмһҗмқҳ кІҪмҡ° Kommerell кІҢмӢӨмқҳ нҷ•мһҘмқҙ 3-5 cm мқҙмғҒмқҙкұ°лӮҳ лҢҖлҸҷл§Ҙ л°•лҰ¬ л“ұмқҳ н•©лі‘мҰқмқҙ лӮҳнғҖлӮң кІҪмҡ°м—җ мҲҳмҲ мқ„ к¶ҢмһҘн•ңлӢӨ[2,3]. ліё мҰқлЎҖмқҳ нҷҳмһҗм—җм„ңлҠ” мҡ°мёЎ лҢҖлҸҷл§Ҙ к¶Ғмқҙ мһҲмңјл©ҙм„ң Kommerell кІҢмӢӨм—җм„ң мқҙмғҒ мўҢмҮ„кіЁн•ҳлҸҷл§Ҙмқҙ кё°мӢңн•ҳкі мһҲм–ҙ Edward 분лҘҳм—җм„ң 2лІҲм§ё мң нҳ•мқҙл©ҙм„ң мқҙкІғм—җ мқҳн•ҙ мӢқлҸ„к°Җ лҲҢл Өм„ң м—°н•ҳкіӨлһҖкіј к°ҖмҠҙ л¶ҲнҺёк°җмқҙ мғқкІјлӢӨ. кё°лҸ„мқҳ м••л°• мҰқмғҒмқҖ м—Ҷм—Ҳкі , нҷҳмһҗлҠ” м–ҙл ёмқ„ л•Ңл¶Җн„° мӢқмӮ¬н• л•Ңл§ҲлӢӨ м—°н•ҳнҶөкіј м—°н•ҳкіӨлһҖмқҙ мһҲм—ҲмңјлӮҳ к·ёкІғмқҙ мӣҗлһҳ мӢқмӮ¬ мӢңм—җ лҠҗк»ҙм§ҖлҠ” лҠҗлӮҢмқҙлқјкі м•Ңкі мһҲм—ҲлӢӨ. м җм°Ё л¶ҲнҺёк°җмқҙ мӢ¬н•ҙм§Җкі кө° кІҖ진 нқүл¶Җ лӢЁмҲңмҙ¬мҳҒмқҳ мқҙмғҒмҶҢкІ¬мңјлЎң лі‘мӣҗм—җ лӮҙмӣҗн•ҳкІҢ лҗҳм—Ҳмңјл©°, мӢқлҸ„м••л°•м—җ мқҳн•ң мҰқмғҒм—җ лҢҖн•ҙ мҲҳмҲ м Ғ м№ҳлЈҢлЎң мҰқмғҒ нҳём „мқҙ лҗң мҰқлЎҖмқҙлӢӨ.
м—°н•ҳкіӨлһҖмқҖ л§Өмҡ° нқ”н•ң мһ„мғҒ мҰқмғҒмқј мҲҳ мһҲмңјлӮҳ нҷҳмһҗмқҳ мҰқмғҒ к°ңм„ мқ„ мң„н•ҙм„ңлҠ” мӣҗмқёмқ„ м•Ңм•„лӮҙлҠ” кІғмқҙ мӨ‘мҡ”н•ҳл©°, л“ңл¬ё мӣҗмқёмңјлЎң Kommerell кІҢмӢӨм—җ мқҳн•ң мӢқлҸ„ м••л°•лҸ„ к°җлі„н•ҙм•ј н• м§Ҳнҷҳл“Ө мӨ‘ н•ҳлӮҳлқјкі н• мҲҳ мһҲкІ лӢӨ.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






