


ņä£ ļĪĀ
ņĀäņŗĀĒÖŹļ░śļŻ©ĒæĖņŖż(systemic lupus erythematosus, SLE)ļŖö ņŚ¼ļ¤¼ ĻĖ░Ļ┤ĆņØä ņ╣©ļ▓öĒĢśļŖö ņĀäņŗĀņĀü ņ×ÉĻ░Ćļ®┤ņŚŁ ņ¦łĒÖśņ£╝ļĪ£ ļŗżņ¢æĒĢ£ ņ×ÉĻ░ĆĒĢŁņ▓┤ņÖĆ ļ®┤ņŚŁļ│ĄĒĢ®ņ▓┤ ĒśĢņä▒ņŚÉ ņØśĒĢ┤ ņĪ░ņ¦ü ņåÉņāüņØ┤ ļéśĒāĆļé£ļŗż[1]. ĒĢśļéśņØś ņןĻĖ░ Ļ│äĒåĄ(organ system)ņØä ņ╣©ļ▓öĒĢśļŖö ņןĻĖ░ ĒŖ╣ņØ┤ ņ×ÉĻ░Ćļ®┤ņŚŁ ņ¦łĒÖśĻ│╝ ļŗ¼ļ”¼ ĒÖśņ×Éļ¦łļŗż Ļ░üĻĖ░ ļŗżņ¢æĒĢ£ ņ×äņāü ņ”Øņāüņ£╝ļĪ£ ļ░£ļ│æĒĢĀ ņłś ņ׳ņ£╝ļ®░, ņ¦łļ│æ Ļ▓ĮĻ│╝ņŚÉ ļö░ļØ╝ ļéśĒāĆļéśļŖö ņ×äņāü ņ”ØņāüĻ│╝ ņåīĻ▓¼ļÅä ļ¦żņÜ░ ļŗżņ¢æĒĢśļŗż. ņØ╝ļ░śņĀüņ£╝ļĪ£ ņĀäņŗĀ ņ”Øņāü, Ēö╝ļČĆņĀÉļ¦ē ņ”Øņāü, ĻĘ╝Ļ│©Ļ▓®Ļ│ä ņ”ØņāüņØ┤ ĒØöĒĢśļéś, ņŗĀņןĻ│╝ Ļ░ÖņØĆ ņŗĀņ▓┤ ņŻ╝ņÜö ņןĻĖ░ļÅä ļŗżņ¢æĒĢśĻ▓ī ņ╣©ļ▓öĒĢĀ ņłś ņ׳ļŗż. ļÅÖņØ╝ĒĢ£ ņןĻĖ░ Ļ│äĒåĄ ļé┤ņŚÉņä£ļÅä ņä£ļĪ£ ļŗżļźĖ ņ”ØņāüņØ┤ ļéśĒāĆļéĀ ņłś ņ׳ņ£╝ļ®░, ņØ┤ļōż ņ”ØņāüņØĆ ĒŖ╣ņĀĢ ņ×ÉĻ░ĆĒĢŁņ▓┤ņÖĆ Ļ┤ĆļĀ©ļÉśĻĖ░ļÅä ĒĢ£ļŗż. ĒÖśņ×ÉņØś Ēśłņ▓ŁņŚÉņä£ ļ░£Ļ▓¼ļÉśļŖö ļŗżņ¢æĒĢ£ ņ×ÉĻ░ĆĒĢŁņ▓┤ļŖö ņ¦äļŗ©ņĀü Ļ░Ćņ╣śļź╝ Ļ░¢ņ¦Ćļ¦ī ĒĢŁĒĢĄĒĢŁņ▓┤ņØś Ļ▓ĮņÜ░, ņŚ¼ļ¤¼ ņ×ÉĻ░Ćļ®┤ņŚŁ ņ¦łĒÖśņŚÉņä£ļÅä ļéśĒāĆļéś ĒŖ╣ņØ┤ļÅäĻ░Ć ļ¢©ņ¢┤ņ¦Ćļ®░ ņ¦łĒÖś ĒŖ╣ņØ┤ ĒĢŁņ▓┤ļĪ£ ņĢīļĀżņ¦ä ĒĢŁdsDNAĒĢŁņ▓┤, ĒĢŁSmĒĢŁņ▓┤ ļō▒ņØĆ ņØ╝ļČĆ ĒÖśņ×ÉņŚÉņä£ļ¦ī ņ¢æņä▒ņØä ļ│┤ņŚ¼ ļ»╝Ļ░ÉļÅäĻ░Ć ļ¢©ņ¢┤ņ¦ĆļŖö ļŗ©ņĀÉņØ┤ ņ׳ļŗż[2,3].
SLE ņ¦äļŗ© ĻĖ░ņżĆņ£╝ļĪ£ Ļ░Ćņן ļäÉļ”¼ ņØ┤ņÜ®ļÉśņ¢┤ ņś© Ļ▓āņØĆ 1982ļģä ļ»ĖĻĄŁļźśļ¦łĒŗ░ņŖżĒĢÖĒÜī(American College of Rheumatology, ACR)ņØś ļČäļźś ĻĖ░ņżĆ[4]ņØä ņØ╝ļČĆ Ļ░£ņĀĢĒĢ£ 1997ļģä ACR ļČäļźś ĻĖ░ņżĆņØ┤ļŗż[5]. ņØ┤Ēøä ņäĖĻ│ä ļŻ©ĒæĖņŖż ņĀäļ¼ĖĻ░Ć ļ¬©ņ×ä(Systemic Lupus International Collaborating Centers, SLICC)ņŚÉņä£ ņØ┤ņĀäņØś ļČäļźś ĻĖ░ņżĆņØä ļ│┤ņÖäĒĢśņŚ¼ 2012ļģä SLICC ļČäļźś ĻĖ░ņżĆņØä ļ░£Ēæ£ĒĢśņśĆņ£╝ļ®░[6], ņĄ£ĻĘ╝ ACR Ļ│╝ ņ£Āļ¤Įļźśļ¦łĒŗ░ņŖżĒĢÖĒÜī(European League Against Rheumatism, EULAR)ņŚÉņä£ļŖö ĻĘ╝Ļ▒░ņŚÉ ĻĖ░ļ░śĒĢśĻ│Ā ņĀäļ¼ĖĻ░Ć ņØśĻ▓¼ņØä ņĀłņČ®ĒĢśņŚ¼ ĒĢŁļ¬®ņŚÉ ļö░ļØ╝ Ļ░Ćņżæņ╣śļź╝ ļČĆņŚ¼ĒĢ£ ņāłļĪ£ņÜ┤ 2019ļģä EULAR/ACR ļČäļźś ĻĖ░ņżĆņØä ļ░£Ēæ£ĒĢśņśĆļŗż[7]. SLE ļČäļźś ĻĖ░ņżĆļōżņØĆ ņ×äņāü ņŚ░ĻĄ¼ ņłśĒ¢ēņØä ņ£äĒĢ┤ Ļ│ĀņĢłļÉśņŚłņ¦Ćļ¦ī, ņ¦äļŻī ĒśäņןņŚÉņä£ SLE ĒÖśņ×Éļź╝ Ļ░Éļ│ä ņ¦äļŗ©ĒĢśļŖöļŹ░ ņé¼ņÜ®ĒĢśĻ│Ā ņ׳ņ£╝ļ®░, ņ¦äļŗ©ņØś ļ»╝Ļ░ÉļÅäņÖĆ ĒŖ╣ņØ┤ļÅäļź╝ ļåÆņØ┤Ļ│Ā ņĪ░ĻĖ░ ņ¦äļŗ©ņ£©ņØä Ē¢źņāüņŗ£ĒéżĻĖ░ ņ£äĒĢ┤ Ļ░£ņĀĢļÉśņ¢┤ ņÖöļŗż. ņØ┤ļōżņØĆ ļŗżņ¢æĒĢ£ Ēśłņ▓ŁĒĢÖņĀü ņåīĻ▓¼ ļ░Å ņĀäĒśĢņĀü ņ”ØņāüņØś ļ¬®ļĪØņ£╝ļĪ£ ĻĄ¼ņä▒ļÉśņ¢┤ ņ׳ņ£╝ļ®░, ĒĢ┤ļŗ╣ ĒĢŁļ¬®ļōżņØś ņĀÉņłś ņ┤ØĒĢ®ņØ┤ ņĀĢĒĢ┤ņ¦ä ņĀÉņłśļź╝ ļäśņ£╝ļ®┤ SLEļĪ£ ļČäļźśĒĢ£ļŗż. ņ£ĀņØ╝ĒĢ£ ņśłņÖĖļŖö ņĪ░ņ¦üĒĢÖņĀüņ£╝ļĪ£ ĒÖĢņ¦äļÉ£ ļŻ©ĒæĖņŖżņŗĀņŚ╝ņØ┤ ņ×ÉĻ░ĆĒĢŁņ▓┤ļź╝ ļÅÖļ░śĒĢśĻ│Ā ņ׳ļŖö Ļ▓ĮņÜ░ļĪ£ 2012ļģä SLICC ļČäļźś ĻĖ░ņżĆņŚÉņä£ ņĀ£ņŗ£ĒĢśĻ│Ā ņ׳ļŗż. Ļ░£ņĀĢļÉ£ 2019ļģä EULAR/ACR ļČäļźś ĻĖ░ņżĆņØĆ ņØ┤ņĀäņØś ļČäļźś ĻĖ░ņżĆĻ│╝ ļŗ¼ļ”¼ ANAļź╝ ņ¦äņ×ģ ĻĖ░ņżĆ(entry criterion)ņ£╝ļĪ£ ņĀ£ņĀĢĒĢśņśĆĻ│Ā Ļ░ü ĒĢŁļ¬®ņŚÉ Ļ░Ćņżæņ╣śļź╝ ļČĆņŚ¼ĒĢśņśĆņ£╝ļ®░, ļČäļźś ĻĖ░ņżĆņØś ļÅÖņØ╝ ņśüņŚŁ ļé┤ ĒĢŁļ¬®ļōż ņżæ Ļ░Ćņן ļåÆņØĆ ņĀÉņłśļ¦īņØä ĒĢ®ņé░ĒĢśļŖö Ļ▓āņØ┤ ĒŖ╣ņ¦ĢņØ┤ļŗż[7]. ļ│ĖĻ│ĀņŚÉņä£ļŖö ņØ┤ņĀäņØś SLE ļČäļźś ĻĖ░ņżĆļōżņØä ļ╣äĻĄÉ┬ĘļČäņäØĒĢśĻ│Ā ņāłļĪ£ņÜ┤ 2019ļģä EULAR/ACR ļČäļźś ĻĖ░ņżĆņØä ņåīĻ░£ĒĢśĻ│Āņ×É ĒĢ£ļŗż. ņØ┤ņÖĆ ĒĢ©Ļ╗ś ņāłļĪ£ņÜ┤ ļČäļźś ĻĖ░ņżĆņØä ļæśļ¤¼ņŗ╝ ļģ╝ļ×ĆĻ│╝ ņ£ĀņÜ®ņä▒ņŚÉ ļīĆĒĢ┤ņä£ļÅä ņé┤ĒÄ┤ļ│┤Ļ│Āņ×É ĒĢ£ļŗż.
ļ│Ė ļĪĀ
1997ļģä Ļ░£ņĀĢļÉ£ ACR ļČäļźś ĻĖ░ņżĆ
1982ļģä ACRņŚÉņä£ ļ░£Ēæ£ĒĢ£ SLE ļČäļźś ĻĖ░ņżĆņØĆ ņ┤Ø 11Ļ░£ ĻĖ░ņżĆņ£╝ļĪ£ ņØ┤ļŻ©ņ¢┤ņĀĖ ņ׳ņ£╝ļ®░, 4Ļ░£ņØś Ēö╝ļČĆņĀÉļ¦ē Ļ┤ĆļĀ© ĻĖ░ņżĆ ļ░Å ņŗ¼ņן Ēś╣ņØĆ ĒÅÉ, ņŗĀņן, ņżæņČöņŗĀĻ▓ĮĻ│ä, Ļ┤ĆņĀł ņ╣©ļ▓öņŚÉ ļīĆĒĢ£ 4Ļ░£ ĻĖ░ņżĆ, ĒśłņĢĪ ļ░Å ļ®┤ņŚŁ Ļ▓Ćņé¼ ņåīĻ▓¼, ANA ņ¢æņä▒ņØä ĒżĒĢ©ĒĢśļŖö ļéśļ©Ėņ¦Ć 3Ļ░£ ĻĖ░ņżĆņ£╝ļĪ£ ĻĄ¼ņä▒ļÉśņ¢┤ ņ׳ļŗż[4]. 11Ļ░£ņØś ĻĖ░ņżĆ ņżæ 4Ļ░£ ņØ┤ņāüņØä ļ¦īņĪ▒ĒĢśļŖö Ļ▓ĮņÜ░ SLEļĪ£ ļČäļźśĒĢśņśĆļŖöļŹ░, ņØ┤ļōżņØ┤ ļ¬©ļæÉ ļÅÖņŗ£ņŚÉ ņĪ┤ņ×¼ĒĢĀ ĒĢäņÜöļŖö ņŚåņ£╝ļ®░, Ļ│╝Ļ▒░ņŚÉ ņĪ┤ņ×¼Ē¢łļŹś ņ”ØņāüļÅä ĒĢ©Ļ╗ś Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢ£ļŗż. ņØ┤ ļČäļźś ĻĖ░ņżĆņØĆ 10ļģä ņØ┤ņāü Ēæ£ņżĆņ£╝ļĪ£ ņé¼ņÜ®ļÉśņŚłņ£╝ļéś ņØ┤Ēøä Ļ░£ļ░£ļÉ£ ņāłļĪ£ņÜ┤ ņ×ÉĻ░ĆĒĢŁņ▓┤ Ļ▓Ćņé¼ļ▓ĢņØä ļ░śņśüĒĢśņŚ¼ 1997ļģä Ļ░£ņĀĢļÉśņŚłļŗż(Table 1). 1997ļģä Ļ░£ņĀĢļÉ£ ACR ļČäļźś ĻĖ░ņżĆņŚÉņä£ļŖö ļ¦Éņ┤łĒśłņĢĪ ļÅäļ¦ÉņŚÉņä£ Ļ┤Ćņ░░ĒĢśļŹś LE ņäĖĒż Ļ▓Ćņé¼Ļ░Ć ņéŁņĀ£ļÉśĻ│Ā, ļīĆņŗĀ ĒĢŁņØĖņ¦Ćņ¦łĒĢŁņ▓┤ Ļ▓Ćņé¼Ļ░Ć ņČöĻ░ĆļÉśņŚłļŗż. ĒĢŁņØĖņ¦Ćņ¦łĒĢŁņ▓┤ Ļ▓Ćņé¼ ļ░®ļ▓Ģņ£╝ļĪ£ņä£ ĒĢŁcardiolipin ĒĢŁņ▓┤, lupus anticoagulant Ļ▓Ćņé¼ ņ¢æņä▒ņØ┤ ņČöĻ░ĆļÉśņŚłņ£╝ļ®░, ņØ┤ņĀäņØś ļ¦żļÅģļ░śņØæ ņ£äņ¢æņä▒ņØĆ ĒĢŁņØĖņ¦Ćņ¦łĒĢŁņ▓┤ Ļ▓Ćņé¼ ļ░®ļ▓Ģ ņżæ ĒĢśļéśļĪ£ ņ£Āņ¦ĆļÉśņŚłļŗż[8]. ĒĢŁņØĖņ¦Ćņ¦łĒĢŁņ▓┤ Ļ▓Ćņé¼ņØś ņČöĻ░ĆļŖö SLEņØś ļ░£ļ│æļźĀĻ│╝ ņ£Āļ│æļźĀ ļ│ĆĒÖöņŚÉļÅä ņśüĒ¢źņØä ļ»Ėņ│żņ£╝ļ®░[9], ņŗ¼ĒśłĻ┤ĆĻ│ä ņ¦łĒÖśņ£╝ļĪ£ ņØĖĒĢ£ ņé¼ļ¦ØļźĀņØ┤ ņ”ØĻ░ĆĒĢśļ®┤ņä£ ĒĢŁņØĖņ¦Ćņ¦łĒĢŁņ▓┤ļź╝ Ļ░¢ļŖö SLE ĒÖśņ×ÉņØś ĒĢŁĒśłņĀä ņ╣śļŻīņŚÉļÅä Ļ┤Ćņŗ¼ņØä Ļ░¢Ļ▓ī ļÉśņŚłļŗż[10]. 1997ļģä ACR ļČäļźś ĻĖ░ņżĆņØä ļäÉļ”¼ ņé¼ņÜ®ĒĢśĻ▓ī ļÉśļ®┤ņä£ ļ¬ć Ļ░Ćņ¦Ć ļ¼ĖņĀ£ņĀÉļōżņØ┤ ņĀ£ĻĖ░ļÉśņŚłļŗż. ņ┤Ø 11Ļ░Ćņ¦Ć ĻĖ░ņżĆ ņżæ Ēö╝ļČĆņĀÉļ¦ē Ļ┤ĆļĀ© ĻĖ░ņżĆņØ┤ 4Ļ░£ļź╝ ņ░©ņ¦ĆĒĢśņŚ¼ Ēö╝ļČĆ ņ”ØņāüņŚÉ Ļ│╝ļŗżĒĢ£ ņĀÉņłśļź╝ ļČĆņŚ¼ĒĢśļŖö ņĀÉ, ņĪ░ņ¦ü Ļ▓Ćņé¼ļź╝ ĒåĄĒĢ┤ ĒÖĢņØĖļÉśņŚłņ£╝ļéś 3Ļ░£ ņØ┤ĒĢśņØś ĻĖ░ņżĆļ¦īņØä ļ¦īņĪ▒ĒĢśļŖö ĒÖśņ×É Ēś╣ņØĆ ņ¦łļ│æ ņ┤łĻĖ░ ĒÖśņ×Éļź╝ ņ¦äļŗ©ĒĢśĻĖ░ ņ¢┤ļĀżņÜ┤ ņĀÉ, ņŗĀĻ▓ĮņĀĢņŗĀĒĢÖņĀü ĻĖ░ņżĆņŚÉ ļ░£ņ×æĻ│╝ ņĀĢņŗĀļ│æ ļæÉ Ļ░Ćņ¦Ćļ¦īņØ┤ ĒżĒĢ©ļÉ£ ņĀÉ ĻĘĖļ”¼Ļ│Ā ņ¦łļ│æĒÖ£ņä▒ļÅäļź╝ ļ░śņśüĒĢśļŖö ļ│┤ņ▓┤ Ļ▓Ćņé¼Ļ░Ć ĒżĒĢ©ļÉśņ¦Ć ņĢŖņĢśļŗżļŖö ņĀÉ ļō▒ņØ┤ļŗż[11]. ņØ┤ļź╝ ļ│┤ņÖäĒĢśĻĖ░ ņ£äĒĢ┤ 2012ļģä SLICCņŚÉņä£ Ļ░£ņĀĢļÉ£ SLE ļČäļźś ĻĖ░ņżĆņØä ļ░£Ēæ£ĒĢśņśĆļŗż[6].
2012ļģä SLICC ļČäļźś ĻĖ░ņżĆ
2012 SLICC ļČäļźś ĻĖ░ņżĆņØĆ 11Ļ░£ņØś ņ×äņāü ĻĖ░ņżĆĻ│╝ 6Ļ░£ņØś ļ®┤ņŚŁ ĻĖ░ņżĆņ£╝ļĪ£ ĻĄ¼ņä▒ļÉśņ¢┤ ņ׳ņ£╝ļ®░, Ļ░üĻ░ü 1Ļ░£ ņØ┤ņāüņØś ņ×äņāüĻ│╝ ļ®┤ņŚŁ ĻĖ░ņżĆņØä ļ¦īņĪ▒ĒĢśĻ│Ā, ņ┤Ø 4Ļ░£ ņØ┤ņāüņØś ĻĖ░ņżĆņØä ņČ®ņĪ▒ĒĢĀ ļĢī SLEļĪ£ ļČäļźśĒĢ£ļŗż. ņØ┤ ņÖĖņŚÉ ANA Ēś╣ņØĆ ĒĢŁdsDNAĒĢŁņ▓┤Ļ░Ć ņ¢æņä▒ņØ┤ļ®┤ņä£ ņĪ░ņ¦üĒĢÖņĀüņ£╝ļĪ£ ļŻ©ĒæĖņŖżņŗĀņŚ╝ņØ┤ ĒÖĢņ¦äļÉ£ Ļ▓ĮņÜ░ņŚÉļŖö ņ£äņØś 4Ļ░Ćņ¦Ć ĻĖ░ņżĆņØä ņČ®ņĪ▒ņŗ£Ēéżņ¦Ć ļ¬╗ĒĢ┤ļÅä SLEļĪ£ ņ¦äļŗ© Ļ░ĆļŖźĒĢśņŚ¼ ļŻ©ĒæĖņŖżņŗĀņŚ╝ņŚÉ ņ¦äļŗ©ņĀüņØĖ Ļ░Ćņżæņ╣śļź╝ ņŻ╝ņŚłļŗż(Table 2). SLE ņ”ØņāüņØä ļŹö ņל ņØ┤ĒĢ┤ĒĢśĻ▓ī ļÉśĻ│Ā, ļŗżņ¢æĒĢ£ ļ®┤ņŚŁĒĢÖņĀü Ļ▓Ćņé¼Ļ░Ć ļ░£ņĀäĒĢ©ņŚÉ ļö░ļØ╝ ņØ┤ļź╝ ļČäļźś ĻĖ░ņżĆņŚÉ ļ░śņśüĒĢśĻ▓ī ļÉśņŚłļŗż. 1997 ACR ļČäļźś ĻĖ░ņżĆĻ│╝ ļ¦łņ░¼Ļ░Ćņ¦ĆļĪ£ 4Ļ░£ņØś Ēö╝ļČĆ Ļ┤ĆļĀ© ĻĖ░ņżĆņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ņ£╝ļéś, ĻĖēņä▒Ļ│╝ ņĢäĻĖēņä▒ ļŻ©ĒæĖņŖż Ēö╝ļČĆļ│æļ│ĆņØä ĒĢśļéśņØś ĻĖ░ņżĆņ£╝ļĪ£ ņĘ©ĻĖēĒĢśņśĆĻ│Ā, ļ░śĒØöņØ┤ ņŚåļŖö Ēāłļ¬©ļź╝ ļ│äļÅäņØś ĒĢŁļ¬®ņ£╝ļĪ£ ņČöĻ░ĆĒĢśņśĆļŗż. ļ░▒ĒśłĻĄ¼ Ļ░Éņåī, ļ”╝ĒöäĻĄ¼ Ļ░Éņåī, ĒśłņåīĒīÉ Ļ░Éņåīļź╝ ĒĢśļéśņØś ĒśłņĢĪĒĢÖņĀü ĻĖ░ņżĆņ£╝ļĪ£ ļ¼ČņŚłļŹś 1997 ACR ļČäļźś ĻĖ░ņżĆĻ│╝ ļŗ¼ļ”¼ ņØ┤ļōż ĒĢŁļ¬®ņØä ļČäļ”¼ĒĢśņŚ¼ ļÅģļ”ĮņĀü ĻĖ░ņżĆņ£╝ļĪ£ ņĘ©ĻĖēĒĢśņśĆņ£╝ļ®░, ņŗĀĻ▓ĮņĀĢņŗĀĒĢÖņĀü ĻĖ░ņżĆņŚÉņä£ļŖö ĻĖ░ņĪ┤ņØś Ļ▓ĮļĀ©ņØ┤ļéś ņĀĢņŗĀļ│æ ņÖĖņŚÉ ļŗżļ░£ņä▒ ļŗ©ņŗĀĻ▓ĮņŚ╝(mononeuritis multiplex), ņ▓ÖņłśņŚ╝(myelitis), ļ¦Éņ┤ł Ēś╣ņØĆ ļæÉĻ░£ ņŗĀĻ▓Įļ│æņ”Ø(peripheral or cranial neuropathy) ĒĢŁļ¬®ņØä ņČöĻ░ĆĒĢśņŚ¼ ņŗĀĻ▓ĮĻ│ä ņ”ØņāüņØä ņóĆ ļŹö ļŗżņ¢æĒĢśĻ▓ī ļ░śņśüĒĢśĻ│Āņ×É ĒĢśņśĆļŗż[12]. ļśÉĒĢ£ ļ®┤ņŚŁ ĻĖ░ņżĆņŚÉņä£ Ļ░üĻ░üņØś ņ×ÉĻ░ĆĒĢŁņ▓┤ļź╝ Ļ░£ļ│ä ĒĢŁļ¬®ņ£╝ļĪ£ ļČäļ”¼ĒĢśņśĆĻ│Ā ĒĢŁņØĖņ¦Ćņ¦łĒĢŁņ▓┤ Ļ▓Ćņé¼ ļ░®ļ▓Ģņ£╝ļĪ£ ĒĢŁbeta2GP1 ĒĢŁņ▓┤Ļ░Ć ņČöĻ░ĆļÉśņŚłņ£╝ļ®░, ļ│┤ņ▓┤ņÖĆ ņ¦üņĀæ ņ┐░ņŖż Ļ▓Ćņé¼ļź╝ ĒżĒĢ©ĒĢśņśĆļŗż. SLICC ļČäļźś ĻĖ░ņżĆņØś ņ¦äļŗ© ņä▒ļŖźņØĆ 1997 ACR ĻĖ░ņżĆņŚÉ ļ╣äĒĢ┤ ĒŖ╣ņØ┤ļÅäļŖö ļé«ņ¦Ćļ¦ī(83% vs. 96%), ļ»╝Ļ░ÉļÅäĻ░Ć ļŹö ļåÆĻ▓ī ļ│┤Ļ│ĀļÉśņŚłļŗż(97% vs. 84%) [6].
1997ļģä ACR ĻĖ░ņżĆĻ│╝ 2012ļģä SLICC ĻĖ░ņżĆņØś ņĀ£ĒĢ£ņĀÉ
1997ļģä ACR ļČäļźś ĻĖ░ņżĆņØĆ ĒŖ╣ņØ┤ļÅäļŖö ļåÆņ¦Ćļ¦ī(96%) ļ»╝Ļ░ÉļÅäĻ░Ć ļŗżņåī ļ¢©ņ¢┤ņ¦Ćļ®░(83%), 11Ļ░£ ĻĖ░ņżĆņŚÉ ņ¦äļŗ©ņĀüņØĖ Ļ░Ćņżæņ╣śļź╝ ņĀäĒśĆ ļ░śņśüĒĢśņ¦Ć ņĢŖļŖö ļ¼ĖņĀ£ņĀÉņØ┤ ņ׳ļŗż. ņśłļź╝ ļōżļ®┤ ņĪ░ņ¦üĒĢÖņĀüņ£╝ļĪ£ ĒÖĢņØĖļÉ£ ļŻ©ĒæĖņŖżņŗĀņŚ╝ņØ┤ļéś ĒśłĻĄ¼Ļ░Éņåīņ”Ø ļō▒ņØĆ SLEņŚÉ ņóĆ ļŹö ņ¦äļŗ©ņĀüņØĖ ņØśļ»Ėļź╝ Ļ░Ćņ¦ĆļŖö ņåīĻ▓¼ņ£╝ļĪ£ ļ│╝ ņłś ņ׳ļŖöļŹ░, ņØ┤ņŚÉ ļīĆĒĢ£ Ļ│ĀļĀż ņŚåņØ┤ Ļ░ü ĻĖ░ņżĆņØś ņĀÉņłśļź╝ ļÅÖņØ╝ĒĢśĻ▓ī ņé░ņĀĢĒĢśļŖö ļ¼ĖņĀ£ņĀÉņØ┤ ņ׳ņŚłļŗż. 2012 SLICC ĻĖ░ņżĆņØĆ 1997 ACR ĻĖ░ņżĆņŚÉ ļ╣äĒĢ┤ ļ»╝Ļ░ÉļÅäļź╝ Ēü¼Ļ▓ī Ļ░£ņäĀĒĢśņśĆņ¦Ćļ¦ī(97%), ļ░śļīĆļĪ£ ĒŖ╣ņØ┤ļÅäĻ░Ć ļé«ņĢäņ¦ĆļŖö(84%) ĒĢ£Ļ│äļź╝ ļ│┤ņśĆļŗż[6]. ņØ┤ļōżņØä ņ”Øņāü ļ░£Ēśä 5ļģä ņØ┤ļé┤ņØĖ ĒÖśņ×ÉļōżņŚÉĻ▓ī ņĀüņÜ®ĒĢśņśĆņØä ļĢī SLE ņ¦äļŗ©ņŚÉ ļīĆĒĢ£ ļ»╝Ļ░ÉļÅäļŖö 1997 ACR ĻĖ░ņżĆņØĆ 76%, 2012 SLICC ĻĖ░ņżĆņØĆ 89.3%ļĪ£ ļæÉ ļČäļźś ĻĖ░ņżĆ ļ¬©ļæÉ ņ¦łļ│æ ņ┤łĻĖ░ ĒÖśņ×ÉņŚÉ ļīĆĒĢ£ ņ¦äļŗ©ņØ┤ ņĀ£ĒĢ£ņĀüņØ┤ļØ╝Ļ│Ā ĒĢĀ ņłś ņ׳ļŗż[13]. ļśÉĒĢ£ ņØ┤ ļČäļźś ĻĖ░ņżĆļōżņØĆ Ļ░ü ĒĢŁļ¬®ļōżņØ┤ ņä£ļĪ£ ļÅģļ”ĮņĀüņØ┤ļØ╝ļŖö Ļ░ĆņĀĢņØä ļ░öĒāĢņ£╝ļĪ£ ĒĢśĻ│Ā ņ׳ļŖöļŹ░, ļ│äĻ░£ļĪ£ ņĘ©ĻĖēĒĢśĻ│Ā ņ׳ļŖö ĒĢŁļ¬®ļōżņØ┤ ņŗżņĀ£ļĪ£ļŖö ļÅÖņØ╝ĒĢ£ ĒśäņāüĻ│╝ ņŚ░Ļ┤ĆļÉśņ¢┤ ļéśĒāĆļéśļŖö Ļ▓āņØ┤ļØ╝ļ®┤ Ļ░ü ĒĢŁļ¬®ņŚÉ Ļ│╝ļŗżĒĢ£ ņĀÉņłśļź╝ ļČĆņŚ¼ĒĢśļŖö Ļ▓░Ļ│╝ļź╝ ņ┤łļלĒĢĀ Ļ░ĆļŖźņä▒ņØ┤ ņ׳ļŗż. ņŚ¼ļ¤¼ ņĀäļ¼ĖĻ░ĆļōżņØĆ Ļ┤æĻ│╝ļ»╝ņä▒Ļ│╝ ļŻ©ĒæĖņŖżĒÖŹļ░śņ▓śļ¤╝ ņØ╝ļČĆ ņ”ØņāüļōżņØĆ Ļ░ÖņØĆ ĒśäņāüņØś Ļ▓░Ļ│╝ļĪ£ ļÅÖļ░śļÉśļŖö Ļ▓āņØ┤ļØ╝Ļ│Ā ņ¦ĆņĀüĒĢ┤ņÖöļŗż[14,15]. Touma ļō▒[16]ņØĆ SLE ļČäļźś ĻĖ░ņżĆņØś ĒĢŁļ¬® Ļ░äņŚÉ ņŗżņĀ£ļĪ£ ĻĄ░ņ¦æ(cluster) ĒśäņāüņØ┤ ņ׳ļŖöņ¦Ć ņĢīņĢäļ│┤Ļ│Āņ×É ĻĄŁņĀ£ ņĪ░ĻĖ░ ļŻ©ĒæĖņŖż ņĮöĒśĖĒŖĖņŚÉņä£ ņØ┤ļ¤¼ĒĢ£ Ēøäļ│┤ ĻĖ░ņżĆļōżņØś ņŚ░Ļ┤Ćņä▒ņØä ņĪ░ņé¼ĒĢśņśĆĻ│Ā, Euro-Lupus ņĮöĒśĖĒŖĖ ļŹ░ņØ┤Ēä░ļź╝ Ļ▓Ćņ”Ø ņĮöĒśĖĒŖĖļĪ£ ņĀüņÜ®ĒĢśņŚ¼ ĒÅēĻ░ĆĒĢśņśĆļŗż. ĻĘĖ Ļ▓░Ļ│╝ ļ░£ņ¦äņØĆ Ļ┤æĻ│╝ļ»╝ņä▒, Ēāłļ¬©, ĻĄ¼Ļ░ĢĻČżņ¢æĻ│╝ ļÅÖļ░śļÉśļ®░, Ēśłņ▓ŁĒĢÖņĀü ņåīĻ▓¼ ņżæ anti-SmņØĆ anti-dsDNAņÖĆ, anti-RNPņÖĆ anti-RoļŖö anti-LaņÖĆ ļÅÖļ░śĒĢśņŚ¼ ļéśĒāĆļéśĻ│Ā, ĒĢŁņØĖņ¦Ćņ¦łĒĢŁņ▓┤ļōżļÅä ņØ┤ļ¤¼ĒĢ£ ĻĄ░ņ¦æņØ┤ ņ׳ņØīņØä ņĢī ņłś ņ׳ņŚłļŗż[16]. ļö░ļØ╝ņä£ Ēö╝ļČĆņĀÉļ¦ē ĻĖ░ņżĆĻ│╝ ĒśłņĢĪĒĢÖņĀü ĻĖ░ņżĆ, ĒŖ╣ņĀĢ ņ×ÉĻ░ĆĒĢŁņ▓┤ĻĄ░ņŚÉņä£ļŖö ņ¦Ćļéśņ╣£ ņĀÉņłś ļČĆņŚ¼ļź╝ Ēö╝ĒĢśĻĖ░ ņ£äĒĢ┤ Ļ░ÖņØĆ ņśüņŚŁ ļé┤ņØś ĒĢŁļ¬®ļōż ņżæ Ļ░Ćņן ļåÆņØĆ ņĀÉņłśļ¦īņØä ĒĢ®ņé░ĒĢśļŖö Ļ▓āņØ┤ ĒĢ®ļ”¼ņĀüņØ┤ļØ╝Ļ│Ā Ļ▓░ļĪĀņ¦ĆņŚłņ£╝ļ®░, ņØ┤ļŖö 2019 EULAR/ACR ļČäļźś ĻĖ░ņżĆņŚÉņä£ ņĀÉņłś ļČĆĻ│╝ ļ░®ņŗØņØś ĻĘ╝Ļ▒░Ļ░Ć ļÉśņŚłļŗż.
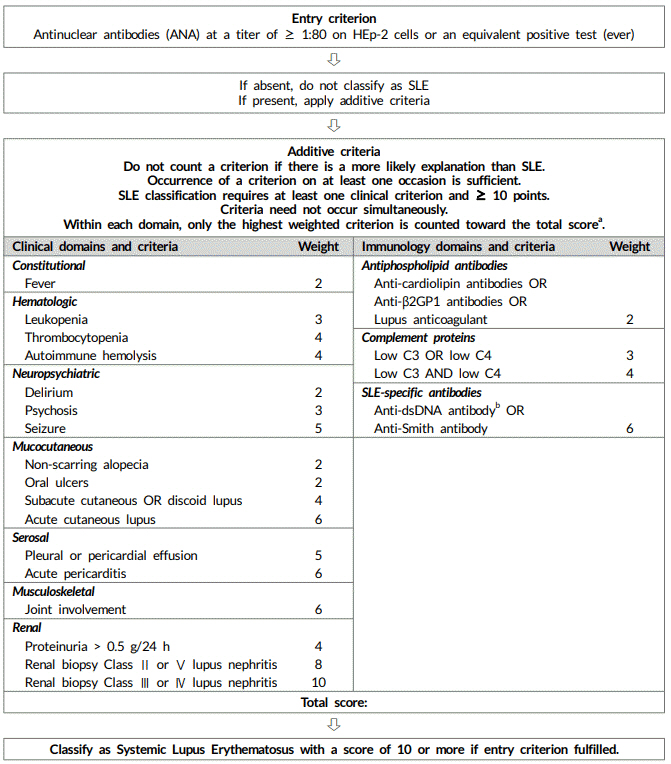
2019 EULAR/ACR ļČäļźś ĻĖ░ņżĆ
ĻĖ░ņĪ┤ņØś SLE ļČäļźś ĻĖ░ņżĆļōżņØĆ ņ┤łĻĖ░ļ│┤ļŗżļŖö ņ£Āļ│æ ĻĖ░Ļ░äņØ┤ ĻĖ┤ ĒÖśņ×ÉļōżņŚÉ ļŹö ņĀüĒĢ®ĒĢśļŗżļŖö ņĀÉņŚÉņä£ ļ░£ļ│æ ņ┤łĻĖ░ ĒÖśņ×ÉļÅä ņ¦äļŗ©ĒĢĀ ņłś ņ׳ļŖö ņāłļĪ£ņÜ┤ ļČäļźś ĻĖ░ņżĆņØś ĒĢäņÜöņä▒ņØ┤ ņĀ£ĻĖ░ļÉśņŚłļŗż. ļśÉĒĢ£ ļ░£ņĀäļÉ£ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ ļ░Å ņĀäļ¼ĖĻ░Ć ņØśĻ▓¼ ļō▒ņØä ļ░śņśüĒĢśĻĖ░ ņ£äĒĢ┤ ļ»ĖĻĄŁĻ│╝ ņ£Āļ¤Įļźśļ¦łĒŗ░ņŖżĒĢÖĒÜī Ļ│ĄļÅÖņ£╝ļĪ£ ļīĆĻĘ£ļ¬©ņØś ĻĄŁņĀ£ ļŗżĒĢÖņĀ£ ņ£äņøÉĒÜīļź╝ ĻĄ¼ņä▒ĒĢśņśĆņ£╝ļ®░, ņŚ¼ļ¤¼ ĒĢ®ņØś ļŗ©Ļ│äļź╝ Ļ▒░ņ│É ņāłļĪ£ņÜ┤ ļČäļźś ĻĖ░ņżĆņØä ļÅäņČ£ĒĢśņśĆļŗż[7]. 2019 EULAR/ACR ļČäļźś ĻĖ░ņżĆņØĆ ļŗżņØīņØś ļæÉ Ļ░Ćņ¦Ć ĻĖ░ļ│Ė Ļ░£ļģÉņŚÉņä£ ņČ£ļ░£ĒĢśņśĆļŗż. ņ▓½ņ¦Ė, ANAļź╝ ļČäļźś ĻĖ░ņżĆņØś ĒĢśļéśļĪ£ ņ£Āņ¦ĆĒĢśĻĖ░ļ│┤ļŗżļŖö ņ¦äņ×ģ ĻĖ░ņżĆ(entry criterion)ņ£╝ļĪ£ ņ▒äĒāØĒĢśļŖö Ļ▓āņØ┤ ļŹö ļéśņØĆ ņ¦äļŗ© ņä▒ļŖźņØä ļ│┤ņØĖļŗż. ņØ┤ļŖö Ļ░äņĀæļ®┤ņŚŁĒśĢĻ┤æļ▓Ģ(indirect immunofluorescence assay, IFA)ņŚÉņä£ 1:80 ņØ┤ņāüņØś ANA ņ¢æņä▒ņØä ņ¦äņ×ģ ĻĖ░ņżĆņ£╝ļĪ£ ĒĢśļ®┤ ņ¦äļŗ©ņŚÉ ļ¦żņÜ░ ļåÆņØĆ ļ»╝Ļ░ÉļÅäļź╝ ļ│┤ņØĖļŗżļŖö ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļź╝ ĻĘ╝Ļ▒░ļĪ£ ĒĢ£ļŗż[17]. ļö░ļØ╝ņä£ ņāłļĪ£ņÜ┤ ļČäļźś ĻĖ░ņżĆņŚÉņä£ļŖö ANAĻ░Ć ĒĢ£ļ▓łņØ┤ļØ╝ļÅä ņ¢æņä▒ņØ┤ņ¢┤ņĢ╝ ļČäļźś ĻĖ░ņżĆņØś ļŗżņØī ļŗ©Ļ│äļĪ£ ņ¦äĒ¢ēĒĢĀ ņłś ņ׳ļŗż(Fig. 1, Table 3). ļæśņ¦Ė, ņØ┤ņĀäņŚÉ ļÅģļ”ĮņĀüņ£╝ļĪ£ ņ£Āņ¦ĆļÉśņ¢┤ ņś© Ļ░ü ĻĖ░ņżĆņØś ņ¦äļŗ©ņĀü Ļ░Ćņ╣śļŖö ļÅÖņØ╝ĒĢśņ¦Ć ņĢŖļŗż. ņśłļź╝ ļōżņ¢┤ ĻĄ¼Ļ░ĢĻČżņ¢æņØä ļŻ©ĒæĖņŖżņŗĀņŚ╝Ļ│╝ ļÅÖļō▒ĒĢśĻ▓ī ņāØĻ░üĒĢĀ ņłś ņŚåļŗżļŖö Ļ▓āņØ┤ļŗż. ņāłļĪ£ņÜ┤ ļČäļźś ĻĖ░ņżĆņØĆ ĒĢŁļ¬®ņŚÉ ļö░ļØ╝ 2-10ņĀÉņØś Ļ░Ćņżæņ╣śļź╝ ļČĆņŚ¼ĒĢśļ®░, 7Ļ░£ņØś ņ×äņāü ĻĖ░ņżĆ(ņĀäņŗĀ ņ”Øņāü, ĒśłņĢĪĒĢÖņĀü ņ¦łĒÖś, ņŗĀĻ▓ĮņĀĢņŗĀ ņ¦łĒÖś, Ēö╝ļČĆņĀÉļ¦ē ņ¦łĒÖś, ņןļ¦ēņŚ╝, ĻĘ╝Ļ│©Ļ▓®Ļ│ä ņ¦łĒÖś, ņŗĀņן ņ¦łĒÖś)Ļ│╝ 3Ļ░£ņØś ļ®┤ņŚŁ ĻĖ░ņżĆ(ĒĢŁņØĖņ¦Ćņ¦łĒĢŁņ▓┤, ļ│┤ņ▓┤, ļŻ©ĒæĖņŖż ĒŖ╣ņØ┤ĒĢŁņ▓┤)ņ£╝ļĪ£ ĻĄ¼ņä▒ļÉśņ¢┤ ņ׳ļŗż. ļÅÖņØ╝ ņśüņŚŁ ļé┤ ĒĢŁļ¬®ļōż ņżæ Ļ░Ćņן ļåÆņØĆ ņĀÉņłśļ¦īņØä ĒĢ®ņé░ĒĢśņŚ¼ ĒÖśņ×É ņĀÉņłśņØś ņ┤ØĒĢ®ņØ┤ 10ņĀÉ ņØ┤ņāüņØ╝ ļĢī SLEļĪ£ ļČäļźśĒĢ£ļŗż(Fig. 1). ņāłļĪ£ņÜ┤ EULAR/ACR ļČäļźś ĻĖ░ņżĆņØä Ļ▓Ćņ”Ø ņĮöĒśĖĒŖĖņŚÉ ņĀüņÜ®ĒĢśņśĆņØä ļĢī ļ»╝Ļ░ÉļÅäļŖö 96%, ĒŖ╣ņØ┤ļÅäļŖö 93%ļź╝ ļ│┤ņśĆņ£╝ļ®░, 1997 ACR ļČäļźś ĻĖ░ņżĆņØĆ Ļ░üĻ░ü 83%, 93%, 2012 SLICC ļČäļźś ĻĖ░ņżĆņØĆ Ļ░üĻ░ü 97%, 84%ņØĖ Ļ▓āĻ│╝ ļ╣äĻĄÉĒĢśļ®┤ Ļ│╝Ļ▒░ ĻĖ░ņżĆļōżņŚÉ ļ╣äĒĢ┤ ņ¦äļŗ© ļŖźļĀźņØ┤ ļŹö ņÜ░ņłśĒĢ£ Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż(Table 4).
ņāłļĪ£ņÜ┤ ļČäļźś ĻĖ░ņżĆņŚÉņä£ ANA Ļ▓Ćņé¼ņØś ņ£äņāü
2019 ACR/EULAR ļČäļźś ĻĖ░ņżĆņŚÉņä£ļŖö ANA ņżæņÜöņä▒ņØä ņ×¼ņĀĢļ”ĮĒĢśņśĆļŗż[7]. ANA ņ¢æņä▒ņØĆ ĒÅēĻ░ĆņØś ņ▓½ ļŗ©Ļ│äļĪ£ņä£ ļ░śļō£ņŗ£ ĒĢ£ ļ▓łņØ┤ļØ╝ļÅä 1:80 ņØ┤ņāüņØś ņŚŁĻ░Ćļź╝ ļ│┤ņŚ¼ņĢ╝ ĒĢ£ļŗż. ANA ņĖĪņĀĢņØĆ HEp2ņäĖĒżļź╝ ņØ┤ņÜ®ĒĢ£ Ļ░äņĀæļ®┤ņŚŁĒśĢĻ┤æļ▓Ģ(HEp2-IFA)ņØ┤ ņśżļ×£ ĻĖ░Ļ░ä Ēæ£ņżĆ Ļ▓Ćņé¼ļ▓Ģņ£╝ļĪ£ ļäÉļ”¼ ņé¼ņÜ®ļÉśņ¢┤ ņÖöļŗż. ĻĘĖļ¤¼ļéś ļ¬©ļōĀ Ļ▓Ćņé¼ņŗżņŚÉņä£ ņØ┤ Ļ▓Ćņé¼Ļ░Ć Ļ░ĆļŖźĒĢśņ¦ĆļŖö ņĢŖĻĖ░ ļĢīļ¼ĖņŚÉ ņØ┤ņÖĆ ņ£Āņé¼ĒĢ£ ņä▒ļŖźņØä ļ│┤ņØ┤ļŖö Ļ│Āņ▓┤ņāü(solid phase) Ļ▓Ćņé¼ļ▓Ģņ£╝ļĪ£ņä£ ĒÜ©ņåīĻ▓░ĒĢ®ļ®┤ņŚŁĒØĪņ░®ļ▓Ģ(enzyme-linked immunosorbent assay, ELISA), ĒśĢĻ┤æĒÜ©ņåīļ®┤ņŚŁņĖĪņĀĢļ▓Ģ(fluoroenzyme immunoassays, FEIA), ĒÖöĒĢÖļ░£Ļ┤æļ®┤ņŚŁļČäņäØļ▓Ģ(chemiluminescence assays, CLIA) ļō▒ņØä ņØ┤ņÜ®ĒĢ£ ANA Ļ▓ĆņČ£ļÅä ņØ┤ļŻ©ņ¢┤ņ¦ĆĻ│Ā ņ׳ļŗż[18]. ANAļź╝ ņ¦äņ×ģ ĻĖ░ņżĆņ£╝ļĪ£ ņé¼ņÜ®ĒĢ£ļŗżļŖö Ļ▓āņØĆ ņ¦ĆņåŹņĀüņ£╝ļĪ£ ANA ņØīņä▒ņØĖ ĒÖśņ×ÉļŖö ņāł ļČäļźś ĻĖ░ņżĆņŚÉņä£ļŖö SLEļĪ£ ņ¦äļŗ©ĒĢĀ ņłś ņŚåļŗżļŖö Ļ▓āņØä ņØśļ»ĖĒĢ£ļŗż. ĻĘĖļ¤¼ļéś ANA ņØīņä▒ņØĖ SLE ĒÖśņ×ÉĻĄ░ņØ┤ ņØ╝ļČĆ ņĪ┤ņ×¼ĒĢśļŖö Ļ▓āņØĆ ņé¼ņŗżņØ┤ļ®░, ņØ┤ļōżņØä ņ£äĒĢ£ ļīĆņ▓┤ ĻĖ░ņżĆņŚÉ ļīĆĒĢ£ ņČöĻ░ĆņĀü ņŚ░ĻĄ¼Ļ░Ć ĒĢäņÜöĒĢśļŗż. ļśÉĒĢ£, ANA ņØīņä▒ ņåīĻ▓¼ņØ┤ ņØ┤ļ»Ė SLEļź╝ ņĪ░ņ¦üĒĢÖņĀüņ£╝ļĪ£ ņ¦äļŗ©ļ░øņĢśĻ▒░ļéś Ļ░ĢļĀźĒ׳ ņØśņŗ¼ļÉśļŖö ĒÖśņ×ÉņŚÉĻ▓ī ĒĢäņÜöĒĢ£ ņ╣śļŻī ņĀ£Ļ│ĄņØä ņ¦ĆņŚ░ņŗ£ĒéżļŖö ĻĘ╝Ļ▒░Ļ░Ć ļÉśņ¢┤ņä£ļŖö ņĢł ļÉ£ļŗż. ļŗżļ¦ī ļČäļźś ĻĖ░ņżĆņØĆ ĒÜ©ņ£©ņĀüņØĖ ņ×äņāü ņŚ░ĻĄ¼ņÖĆ ņ×äņāüņŗ£ĒŚśņØä ļ¬®ņĀüņ£╝ļĪ£ ļ¦īļōżņ¢┤ņĪīļŗżļŖö ņĘ©ņ¦ĆņŚÉ ļ╣äņČöņ¢┤ļ│╝ ļĢī ANA ņØīņä▒ņØĖ ĒÖśņ×ÉļŖö ņ×äņāüņŗ£ĒŚśņŚÉņä£ ņĀ£ņÖĖĒĢ┤ļÅä ļ¼┤ļ░®ĒĢśļŗżļŖö Ļ▓āņØ┤ ņĀĆņ×ÉļōżņØś ņāØĻ░üņØ┤ļŗż[7].
ņ×äņāü ļ░Å ļ®┤ņŚŁ ĻĖ░ņżĆņØś ļ│ĆĒÖö
ņĪ░ĻĖ░ ļŻ©ĒæĖņŖż ņĮöĒśĖĒŖĖņŚÉņä£ ļŗżļźĖ ņ×ÉĻ░Ćļ®┤ņŚŁ ņ¦łĒÖśņŚÉ ļ╣äĒĢ┤ ļ░£ņŚ┤ņØ┤ ņ┤łĻĖ░ ņ”Øņāüņ£╝ļĪ£ ņ×ÉņŻ╝ ļéśĒāĆļé¼ĻĖ░ ļĢīļ¼ĖņŚÉ ņ×äņāü ĻĖ░ņżĆņŚÉ ļ░£ņŚ┤ņØä ĒżĒĢ©ĒĢśņŚ¼ ņĪ░ĻĖ░ ņ¦äļŗ©ņŚÉ ļÅäņøĆņØä ņŻ╝Ļ│Āņ×É ĒĢśņśĆļŗż. ļśÉĒĢ£ Ļ░ü ĻĖ░ņżĆļōżņØä ļÅÖņØ╝ ņśüņŚŁļ│äļĪ£ ĻĄ¼ņĪ░ĒÖöĒĢśņśĆņ£╝ļ®░, ņ¦äļŗ©ņĀü Ļ░Ćņ╣śņŚÉ ļö░ļØ╝ Ļ░Ćņżæņ╣śļź╝ ļČĆņŚ¼ĒĢśņśĆļŗż. ĻĖēņä▒ ņŗ¼ļ¦ēņŚ╝ņØä ĒØēļ¦ē Ēś╣ņØĆ ņŗ¼ļ¦ēņé╝ņČ£Ļ│╝ ĻĄ¼ļČäĒĢśņśĆĻ│Ā 2012 SLICC ĻĖ░ņżĆņØś ņŗĀĻ▓ĮņĀĢņŗĀ ņ¦łĒÖś ĻĖ░ņżĆņŚÉ ĒżĒĢ©ļÉśņŚłļŹś ļŗżļ░£ņä▒ ļŗ©ņŗĀĻ▓ĮņŚ╝, ņ▓ÖņłśņŚ╝, ļ¦Éņ┤ł Ēś╣ņØĆ ļæÉĻ░£ ņŗĀĻ▓Įļ│æņ”Ø ĒĢŁļ¬®ņØĆ ļŗżņŗ£ ņĀ£ņÖĖļÉśņŚłļŗż. ņŗĀņן ņ¦łĒÖśņŚÉņä£ļÅä ļŻ©ĒæĖņŖżņŗĀņŚ╝ņØś ņĪ░ņ¦üĒĢÖņĀü ļČäļźśņŚÉ ļö░ļØ╝ Ļ░Ćņżæņ╣śļź╝ ļŗżļź┤Ļ▓ī ļČĆņŚ¼ĒĢśņśĆļŖöļŹ░, International Society of Nephrology/Renal Pathology Society ļČäļźś 3ĒśĢ Ēś╣ņØĆ 4ĒśĢņØ┤ 2ĒśĢ Ēś╣ņØĆ 5ĒśĢļ│┤ļŗż ļåÆņØĆ ņĀÉņłśļź╝ ļ░øļŖöļŗż. Ļ▓Ćņé¼ļÅä C3ņÖĆ C4 ļ¬©ļæÉ Ļ░ÉņåīĒĢ£ Ļ▓ĮņÜ░Ļ░Ć ĒĢśļéśļ¦ī Ļ░ÉņåīĒĢ£ Ļ▓ĮņÜ░ļ│┤ļŗż ļåÆņØĆ ņĀÉņłśļź╝ ļ░øļÅäļĪØ ĒĢśņśĆļŗż. Ļ░ü ĒĢŁļ¬®ņØĆ SLE ņÖĖņŚÉ ņØ┤ļź╝ ņäżļ¬ģĒĢĀ ņłś ņ׳ļŖö ņøÉņØĖņØ┤ ņĪ┤ņ×¼ĒĢśņ¦Ć ņĢŖņØä ļĢīļ¦ī ņĀÉņłśļź╝ ļČĆņŚ¼ĒĢ┤ņĢ╝ ĒĢśļ®░, ļÅÖņØ╝ ņśüņŚŁ ļé┤ņŚÉņä£ Ļ░Ćņן ļåÆņØĆ ņĀÉņłśļź╝ ĒĢ®ņé░ĒĢ£ļŗż.
ANAļź╝ ņ¦äņ×ģ ĻĖ░ņżĆ(entry criteria)ņ£╝ļĪ£ ņé¼ņÜ®ĒĢśļŖö Ļ▓āņŚÉ ļīĆĒĢ£ ļģ╝ļ×Ćļōż
ANAļź╝ ņ¦äņ×ģ ĻĖ░ņżĆņ£╝ļĪ£ ļæÉļŖö Ļ▓āņØĆ ļŗżņØī ņäĖ Ļ░Ćņ¦Ć Ļ░ĆņĀĢņØ┤ ļ¦īņĪ▒ļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż. ņ▓½ņ¦Ė, SLEņŚÉņä£ ANA ņ¢æņä▒ņØĆ ņśłņÖĖ ņŚåņØ┤ ĒĢäņłśņĀüņØ┤ļ®░, ANA ņØīņä▒ ļŻ©ĒæĖņŖżļŖö ļ¦żņÜ░ ļō£ļ¼╝ļŗż[19]. ļæśņ¦Ė, SLEņŚÉņä£ ANA ņ¢æņä▒ņØĆ ņŗ£Ļ░äņØ┤ Ļ▓ĮĻ│╝ĒĢ┤ļÅä ņ¦ĆņåŹļÉ£ļŗż. ĻĘĖļ¤¼ļ»ĆļĪ£ ņ¦łļ│æ Ļ▓ĮĻ│╝ ņżæ ņ¢┤ļŖÉ ņŗ£ņĀÉņŚÉ Ļ▓Ćņé¼ĒĢśļŹöļØ╝ļÅä ANA ņ¢æņä▒ņØä ļČäļźś ĻĖ░ņżĆņØś ņČ£ļ░£ņĀÉņ£╝ļĪ£ ņé¼ņÜ®ĒĢĀ ņłś ņ׳ļŗż. ņģŗņ¦Ė, ANAļź╝ Ļ▓ĆņČ£ĒĢśļŖö Ēæ£ņżĆ Ļ▓Ćņé¼ļŖö HEp2-IFA Ēś╣ņØĆ Ļ│Āņ▓┤ņāü(solid phase) Ļ▓Ćņé¼ļ▓ĢņØ┤ļŗż. SLEņŚÉņä£ ANA ņ¢æņä▒ņ£©ņØĆ 95-99%ļĪ£ ņĢīļĀżņĀĖ ņ׳ņ£╝ļ®░, 100%ļĪ£ ļ│┤Ļ│ĀĒĢ£ Ļ▓ĮņÜ░ļŖö ņåīņłśņŚÉ ļČłĻ│╝ĒĢśļŗż[19,20]. ļŗ©ļ®┤ņĀü ņŚ░ĻĄ¼ļōżņŚÉņä£ļŖö ļŹö ļé«Ļ▓ī ļ│┤Ļ│ĀļÉśļŖö Ļ▓ĮņÜ░ļÅä ļ╣łļ▓łĒĢśļ®░, SLEņŚÉņä£ ANAņØś ņŗżņĀ£ ņ¢æņä▒ņ£©ņØĆ ņĢīļĀżņĀĖ ņ׳ņ¦Ć ņĢŖļŗż. ĻĘĖ ņØ┤ņ£ĀļŖö ļīĆņāü ĒÖśņ×É, ņ£Āļ│æ ĻĖ░Ļ░ä, ņØ┤ņĀäņØś ņ╣śļŻī, ņé¼ņÜ®ļÉ£ ANA Ļ▓Ćņé¼ļ▓ĢļōżņØ┤ ļ¬©ļæÉ ļÅÖņØ╝ĒĢśņ¦Ć ņĢŖĻĖ░ ļĢīļ¼ĖņØ┤ļŗż. ĒĢŁ IL-6ļź╝ ņØ┤ņÜ®ĒĢ£ 2ņāü ņ×äņāü ņŚ░ĻĄ¼ņŚÉņä£ļŖö ļō▒ļĪØļÉ£ SLE ĒÖśņ×ÉņØś ņäĀļ│ä Ļ▓Ćņé¼ Ļ▓░Ļ│╝ 23.8%Ļ░Ć ANA ņØīņä▒ņ£╝ļĪ£ ļéśĒāĆļé¼ņ£╝ļ®░, ļ▓©ļ”¼ļ¼┤ļ▒ü 2ņāü ņ×äņāü ņŚ░ĻĄ¼ļÅä ANA ņØīņä▒ņ£©ņØä 30%Ļ╣īņ¦Ć ļåÆĻ▓ī ļ│┤Ļ│ĀĒĢ£ ļ░ö ņ׳ļŗż[21]. SLE ĒÖśņ×ÉļŖö ņ¢┤ļŖÉ ņŗ£ĻĖ░ņŚÉ ANAļź╝ Ļ▓Ćņé¼ĒĢ┤ļÅä 100% ņ¢æņä▒ņØ┤ļØ╝ļŖö Ļ▓¼ĒĢ┤ļŖö ņāüļŗ╣ ļČĆļČä Ļ░ĆņĀĢņŚÉ ņØśņĪ┤ĒĢśĻ│Ā ņ׳ļŖö Ļ▓āņØ┤ļŗż. ņØ┤ņŚÉ ANA ņ¢æņä▒ņØä ĒĢäņłś ņ¦äņ×ģņĪ░Ļ▒┤ņ£╝ļĪ£ ņ▒äĒāØĒĢ£ Ļ▓āņŚÉ ļīĆĒĢ┤ ļģ╝ļ×ĆņØ┤ ļÉśĻ│Ā ņ׳ļŗż. ņØ┤ļ»Ė ņ¦äļŗ©ņØ┤ ĒÖĢņĀĢļÉ£ SLE ĒÖśņ×ÉņŚÉņä£ ANA ņØīņä▒ņØ┤ ņ×ÉņŻ╝ ļéśĒāĆļéśļŖö ņØ┤ņ£ĀļŖö ļŗżņØīņØś ļæÉ Ļ░Ćņ¦Ć ņØ┤ņ£ĀĻ░Ć Ļ░ĆļŖźĒĢśļŗż. ĒĢśļéśļŖö ņŗ£Ļ░ä Ļ▓ĮĻ│╝ņŚÉ ļö░ļØ╝ Ēś╣ņØĆ ņ╣śļŻīņŚÉ ļö░ļØ╝ Ēśłņ▓ŁĒĢÖņĀü ņåīĻ▓¼ņØ┤ ļŗ¼ļØ╝ņ¦ł ņłś ņ׳ļŗżļŖö Ļ▓āņØ┤Ļ│Ā, ļŗżļźĖ ĒĢśļéśļŖö Ēśäņ×¼ ņé¼ņÜ®ĒĢśĻ│Ā ņ׳ļŖö Ļ▓Ćņé¼ ļ░®ļ▓ĢņØś ņä▒ļŖźĻ│╝ Ļ┤ĆļĀ©ļÉ£ ĻĖ░ņłĀņĀüņØĖ ļ¼ĖņĀ£ņØ┤ļŗż[22]. 2019 EULAR/ACR ļČäļźś ĻĖ░ņżĆņŚÉņä£ ANA ņ¢æņä▒ņØ┤ ĒĢäņłś ĻĖ░ņżĆņ£╝ļĪ£ ļō▒ņןĒĢ©ņŚÉ ļö░ļØ╝ ļŹö ļéśņØĆ ANA Ļ▓Ćņé¼ļ▓ĢņŚÉ ļīĆĒĢ£ Ļ┤Ćņŗ¼ņØ┤ ņ”ØĻ░ĆĒĢśĻ│Ā ņ׳ļŗż. ANA ņ¢æņä▒ņ£©ņØĆ ņé¼ņÜ®ĒĢ£ Ļ▓Ćņé¼ļ▓ĢĻ│╝ Ļ▓Ćņé¼ ĒéżĒŖĖņŚÉ ļö░ļØ╝ ļŗ¼ļØ╝ņ¦ł ņłś ņ׳ļŗż. ĒĢ£ ņŚ░ĻĄ¼[22]ņŚÉņä£ ņŗĀņן ņ╣©ļ▓öņØ┤ ņŚåĻ│Ā ņ£Āļ│æ ĻĖ░Ļ░äņØ┤ ļŗżņ¢æĒĢ£ 103ļ¬ģņØś SLE ĒÖśņ×É Ēśłņ▓ŁņØä ņäĖ Ļ░Ćņ¦Ć ļŗżļźĖ HEp2-IFA kitļĪ£ Ļ▓Ćņé¼ĒĢśņśĆņØä ļĢī ANA ņØīņä▒ņ£©ņØĆ 4.9-22.3%ļĪ£ ļŗżņ¢æĒĢśĻ▓ī ļéśĒāĆļé¼ļŗż. ELISA Ļ▓Ćņé¼ļ▓ĢņØś ņØīņä▒ņ£©ņØĆ 13.6%ņśĆņ£╝ļ®░, ļŗżņżæļČäņäØļ▓Ģ(multiplex)ņØś ņØīņä▒ņ£©ļÅä 13.6%ņśĆļŗż. ļö░ļØ╝ņä£ ņ¢┤ļ¢ĀĒĢ£ Ļ▓Ćņé¼ļÅä 100%ņØś ņ¢æņä▒ņ£©ņŚÉ ļÅäļŗ¼ĒĢśņ¦Ć ļ¬╗ĒĢśņśĆņ£╝ļ®░, ņØ┤ļōż Ļ▓Ćņé¼ļ▓ĢņØä ņĪ░ĒĢ®ĒĢśņŚ¼ ņé¼ņÜ®ĒĢśņśĆņØä ļĢī ņ¢æņä▒ņ£©ņØ┤ 100%ņŚÉ ĻĘ╝ņĀæĒĢśĻ▓ī ļÉśņŚłļŗż. HEp2-IFA ņŚŁĻ░ĆĻ░Ć 1:80ņØ╝ ļĢī SLE ĒÖĢņ¦äņŚÉ ļīĆĒĢ£ ņÜ░ļÅäļ╣ä(likelihood ratio)ļŖö 1.1ņØ┤ļ®░, ņŚŁĻ░Ćļź╝ 1:160, 1:320, 1:640ņ£╝ļĪ£ ņ”ØĻ░Ćņŗ£Ēéżļ®┤ ņÜ░ļÅäļ╣äļŖö Ļ░üĻ░ü 4.1ļ░░, 7.0ļ░░, 14.7ļ░░ļĪ£ ņ”ØĻ░ĆĒĢśņśĆļŗż[23]. ņĄ£ĻĘ╝ņØś ļ®öĒāĆ ļČäņäØ ņŚ░ĻĄ¼ņŚÉņä£ļŖö HEp2-IFAņÖĆ Ļ│Āņ▓┤ņāü ļČäņäØļ▓Ģ(solid phase assay)ņØĖ FEIA Ļ▓Ćņé¼ļź╝ ļ│æĒ¢ēĒĢśņśĆņØä ļĢī ļŗ©ļÅģ Ļ▓Ćņé¼ļ│┤ļŗż ņ¦äļŗ© ņĀĢĒÖĢļÅäļź╝ ļåÆņØ╝ ņłś ņ׳ļŗżļŖö ņé¼ņŗżņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż[24]. ļŗżņ¢æĒĢ£ ANA Ļ▓Ćņé¼ļ▓ĢņØś ņ¢æņä▒ņ£©ņØ┤ ņØ╝ņĀĢĒĢśņ¦Ć ņĢŖļŗżļŖö ņĀÉĻ│╝ ļŻ©ĒæĖņŖż ĒÖśņ×ÉņØś ņŗżņĀ£ ANA ņ¢æņä▒ņ£©ņØä ņĀĢĒÖĢĒ׳ ļ¬©ļźĖļŗżļŖö ņĀÉņØĆ ņāłļĪ£ņÜ┤ ļČäļźś ĻĖ░ņżĆņØś ļģ╝ļ×ĆņØ┤ ļÉśĻ│Ā ņ׳ļŗż. ņĢ×ņ£╝ļĪ£ ņØ┤ ļ¼ĖņĀ£ņĀÉņØä ĒĢ┤Ļ▓░ĒĢśĻĖ░ ņ£äĒĢ£ ņŚ░ĻĄ¼Ļ░Ć ļŹö ļ¦ÄņØ┤ ņŗ£Ē¢ēļÉśņ¢┤ņĢ╝ ĒĢśļéś Ēśäņ×¼ļĪ£ņä£ļŖö IFAņÖĆ Ļ│Āņ▓┤ņāü ļČäņäØļ▓ĢņØä ļ│æņÜ®ĒĢśļŖö Ļ▓āņØ┤ ņĄ£ņäĀņØś ļ░®ļ▓ĢņØ╝ Ļ▓āņØ┤ļŗż.
2019 EULAR/ACR ĻĖ░ņżĆņØś ņĀüņÜ®
2019 EULAR/ACR ĻĖ░ņżĆņØ┤ ļ░£Ēæ£ļÉ£ ņØ┤Ēøä ņØ┤ļź╝ ņŗżņĀ£ ņ¦äļŻī ņżæņØĖ Ēś╣ņØĆ Ļ│╝Ļ▒░ņØś ĒÖśņ×ÉļōżņŚÉĻ▓ī ņĀüņÜ®ĒĢśņŚ¼ ĻĘĖ ņ£ĀņÜ®ņä▒ņØä ņĢīņĢäļ│┤Ļ│Āņ×ÉĒĢśļŖö ņŚ░ĻĄ¼Ļ░Ć ĒÖ£ļ░£Ē׳ ņ¦äĒ¢ēļÉśĻ│Ā ņ׳ļŗż. Sacre ļō▒[25]ņØĆ ņŗ¼ļ¦ēņé╝ņČ£ļĪ£ ņ×ģņøÉĒ¢łļŹś 129ļ¬ģņØś ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ņØ┤ ĻĖ░ņżĆņØä ņĀüņÜ®ĒĢśņśĆņØäļĢī 17ļ¬ģņØ┤ SLEļĪ£ ņ¦äļŗ©ļÉśņŚłņ£╝ļ®░, ļ»╝Ļ░ÉļÅäļŖö 100%ņśĆņ£╝ļéś ĒŖ╣ņØ┤ļÅäļŖö 84%ļĪ£ ļŗżņåī ļé«ņĢśļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż. ņØ┤ņŚÉ Aringer ļō▒[26]ņØĆ Sacre ņŚ░ĻĄ¼ņØś ļ»╝Ļ░ÉļÅäĻ░Ć ļé«ņØĆ Ļ▓āņØĆ ļČäļźś ĻĖ░ņżĆņØä ļČĆņĀüņĀłĒĢśĻ▓ī ņĀüņÜ®ĒĢśņśĆĻĖ░ ļĢīļ¼ĖņØ┤ļØ╝ļŖö ļ░śļĪĀņØä ņĀ£ĻĖ░ĒĢ£ ļ░ö ņ׳ļŗż. ņ”ē, ĒĢ┤ļŗ╣ ņ”ØņāüņØ┤ļéś ņåīĻ▓¼ņØä ņäżļ¬ģĒĢĀ ņłś ņ׳ļŖö ņøÉņØĖņØ┤ SLEņØ╝ ļĢīļ¦ī ņĀÉņłśļź╝ ņé░ņĀĢĒĢ┤ņĢ╝ ĒĢśļŖöļŹ░ ĻĘĖļĀćņ¦Ć ņĢŖņĢśļŗżļŖö Ļ▓āņØ┤ļŗż. Adamichou ļō▒[27]ņØ┤ 1997 ACR, 2012 SLICC, 2019 EULAR/ACR ĻĖ░ņżĆņØä ņĪ░ĻĖ░ ļŻ©ĒæĖņŖż ņĮöĒśĖĒŖĖņŚÉ ņĀüņÜ®ĒĢśņśĆņØä ļĢī ļ»╝Ļ░ÉļÅäļŖö Ļ░üĻ░ü 82.7%, 91.3%, 88.6%ļĪ£ ļéśĒāĆļéś 2012 SLICCĻ│╝ 2019 EULAR/ACR ĻĖ░ņżĆņØ┤ ņĪ░ĻĖ░ ņ¦äļŗ©ņŚÉļŖö ņóĆ ļŹö ņĀüĒĢ®ĒĢ£ Ļ▓āņ£╝ļĪ£ ļ│┤ņśĆļŗż. ņäĖ Ļ░Ćņ¦Ć ĻĖ░ņżĆ ļ¬©ļæÉļź╝ ļ¦īņĪ▒ĒĢśļŖö ĒÖśņ×ÉļŖö 76.7%ņŚÉ ļČłĻ│╝ĒĢśņśĆņ£╝ļ®░, Ļ░ü ĻĖ░ņżĆļ¦łļŗż 25.6-30%ņØś ĒÖśņ×Éļź╝ ņ¦äļŗ©ĒĢśņ¦Ć ļ¬╗ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż. ņŻ╝ļ¬®ĒĢĀ ņĀÉņØĆ ņ¦äļŗ©ļÉśņ¦Ć ļ¬╗ĒĢ£ ĒÖśņ×ÉņØś ņāüļŗ╣ņłśļŖö ņżæļō▒ļÅä ņØ┤ņāüņØś ņ”ØņāüņØ┤ļéś ņןĻĖ░ ņåÉņāüņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ņŚłļŗżļŖö ņĀÉņØ┤ļŗż. ļö░ļØ╝ņä£ SLE ņ¦äļŗ©ņ£©ņØä ĻĘ╣ļīĆĒÖöĒĢśĻĖ░ ņ£äĒĢ┤ņä£ļŖö ņäĖ Ļ░Ćņ¦Ć ĻĖ░ņżĆ ļ¬©ļæÉļź╝ ņāüĒśĖļ│┤ņÖäņĀüņ£╝ļĪ£ ņé¼ņÜ®ĒĢ┤ņĢ╝ ĒĢ£ļŗżĻ│Ā ņĀ£ņĢłĒĢśņśĆļŗż. ņØ┤ņÖĖ ņ×äņāüņĀü ņ£Āņé¼ņä▒ņØä Ļ│Ąņ£ĀĒĢśļŖö ņć╝ĻĘĖļĀī ņ”ØĒøäĻĄ░Ļ│╝ SLE, ļæÉ ņ¦łĒÖśņØ┤ ĒĢ©Ļ╗ś ļéśĒāĆļéśļŖö ņżæļ│Ą ņ”ØĒøäĻĄ░ņØä Ļ░Éļ│äĒĢśļŖö ļŹ░ņŚÉļÅä ņāłļĪ£ņÜ┤ ļČäļźś ĻĖ░ņżĆņØ┤ ņ£ĀņÜ®ĒĢśņśĆļŗżļŖö ļ│┤Ļ│ĀĻ░Ć ņ׳ņŚłļŗż[28]. ņĄ£ĻĘ╝ 100ļ¬ģņØś SLE ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ņŗ£Ē¢ēĒĢ£ ņØ╝ļ│ĖņØś ĒĢ£ ĒøäĒ¢źņĀü ņŚ░ĻĄ¼ņŚÉņä£ļŖö 2019 EULAR/ACR ĻĖ░ņżĆņØś ļ»╝Ļ░ÉļÅäļŖö 92%ļĪ£ 1997 ACR ĻĖ░ņżĆ(97%)ņØ┤ļéś 2012 SLICC ĻĖ░ņżĆ(99%)ņŚÉ ļ╣äĒĢ┤ ļŗżņåī ļé«Ļ▓ī ļéśĒāĆļé¼ļŗż[29]. ļśÉĒĢ£ SLEļĪ£ ņ¦äļŗ©ļÉśņ¦Ć ļ¬╗ĒĢ£ ĒÖśņ×ÉņØś ļīĆļČĆļČäņØĆ ANA ņŚŁĻ░ĆĻ░Ć 1:80 ņØ┤ĒĢśņśĆļŹś ĒÖśņ×ÉļōżļĪ£ ņØ┤ļōżņØś ņ¦äļŗ©ņØä ļåōņ╣śņ¦Ć ņĢŖĻĖ░ ņ£äĒĢ┤ņä£ļŖö ņ¦äņ×ģ ĻĖ░ņżĆņØś ļ│┤ņÖäņØ┤ ĒĢäņÜöĒĢ┤ ļ│┤ņØĖļŗż.
Ļ▓░ ļĪĀ
SLEņØś ļ░£ļ│æ ņ¢æņāüņØĆ ĒÖśņ×Éļ¦łļŗż Ēü░ ņ░©ņØ┤ļź╝ ļ│┤ņØ╝ ļ┐Éļ¦ī ņĢäļŗłļØ╝ ļŗżļźĖ ņĀäņŗĀņĀü ņ×ÉĻ░Ćļ®┤ņŚŁ ņ¦łĒÖśĻ│╝ ņżæļ│ĄļÉśļŖö ņåīĻ▓¼ļōżļĪ£ ņØĖĒĢ┤ ņ¦äļŗ©ņŚÉ ņ¢┤ļĀżņøĆņØ┤ ļ¦Äļŗż. SLE ļČäļźś ĻĖ░ņżĆņØĆ ņ×äņāü ņ”Øņāü ļ░Å ņ¦ĢĒøä, Ļ▓Ćņé¼ņŗż ņåīĻ▓¼ņØä ņóģĒĢ®ĒĢśņŚ¼ ĻĄ¼ņä▒ļÉśņ¢┤ ņ׳ņ£╝ļ®░, ņ¦äļŗ©ņØś ļ»╝Ļ░ÉļÅäņÖĆ ĒŖ╣ņØ┤ļÅäļź╝ ļåÆņØ┤Ļ│Ā, ņĪ░ĻĖ░ ņ¦äļŗ©ņØä Ē¢źņāüņŗ£ĒéżĻĖ░ ņ£äĒĢ┤ ļ░£ņĀäļÉśņ¢┤ ņÖöļŗż. ņ¦ĆĻĖłĻ╣īņ¦Ć 1997ļģä Ļ░£ņĀĢļÉ£ ACR ĻĖ░ņżĆĻ│╝ 2012ļģä SLICC ĻĖ░ņżĆņØä ņ×äņāü ņŚ░ĻĄ¼ ļ░Å ņ¦äļŻī ĒśäņןņŚÉņä£ ļäÉļ”¼ ņé¼ņÜ®ĒĢ┤ ņÖöņ£╝ļéś ņØ┤ņĀä ļČäļźś ĻĖ░ņżĆļōżņØś ļ¼ĖņĀ£ņĀÉņØä ļ│┤Ļ░ĢĒĢśĻ│Ā ņČĢņĀüļÉ£ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ņÖĆ ņĀäļ¼ĖĻ░Ć ņØśĻ▓¼ņØä ļ░śņśüĒĢśņŚ¼ 2019ļģä ļ»ĖĻĄŁĻ│╝ ņ£Āļ¤Įļźśļ¦łĒŗ░ņŖżĒĢÖĒÜī Ļ│ĄļÅÖņ£╝ļĪ£ ņāłļĪ£ņÜ┤ ļČäļźś ĻĖ░ņżĆņØä ļ░£Ēæ£ĒĢśņśĆļŗż. 2019ļģä EULAR/ACR ļČäļźś ĻĖ░ņżĆņØĆ ANAļź╝ ņ¦äņ×ģ ĻĖ░ņżĆņ£╝ļĪ£ ņé¼ņÜ®ĒĢśĻ│Ā, Ļ░ü ĒĢŁļ¬®ņŚÉ Ļ░Ćņżæņ╣śļź╝ ļČĆņŚ¼ĒĢśļ®░, Ļ│äņĖĄ ĻĄ¼ņĪ░ņĀüņ£╝ļĪ£ ņśüņŚŁņØä ļéśļłäņŚłļŗżļŖö ĒŖ╣ņ¦ĢņØ┤ ņ׳ļŗż. ņāłļĪ£ņÜ┤ ļČäļźś ĻĖ░ņżĆņØĆ ņØ┤ņĀä ĻĖ░ņżĆņŚÉ ļ╣äĒĢ┤ ļ»╝Ļ░ÉļÅäņÖĆ ĒŖ╣ņØ┤ļÅä ļ¬©ļæÉ ņÜ░ņłśĒĢ£ ņ¦äļŗ© ņä▒ļŖźņØä ļéśĒāĆļéĖļŗż. ļśÉĒĢ£ ņ×äņāü ĻĖ░ņżĆņŚÉ ļ░£ņŚ┤ņØä ĒżĒĢ©ĒĢśņŚ¼ ņ┤łĻĖ░ ĒÖśņ×ÉņØś ņ¦äļŗ©ņŚÉ ļÅäņøĆņØä ņŻ╝Ļ│Āņ×É ĒĢśņśĆņ£╝ļ®░, ņŗĀņן ņĪ░ņ¦ü Ļ▓Ćņé¼ ņåīĻ▓¼ņØä ļČäļ”¼ĒĢśņŚ¼ Ļ░ü ņåīĻ▓¼ļ¦łļŗż ņ¦äļŗ©ņŚÉ ļ»Ėņ╣śļŖö ņśüĒ¢źņØ┤ ļŗżļ”äņØä ļ░śņśüĒĢśĻ│Āņ×É ĒĢśņśĆļŗż. ĻĘĖļ¤¼ļéś ņ£Āļ│æ ĻĖ░Ļ░äņØ┤ļéś Ļ▓Ćņé¼ ņŗ£ņĀÉņŚÉ ļö░ļØ╝ ņŚäņŚ░Ē׳ ANA ņØīņä▒ņØĖ SLE ĒÖśņ×ÉļōżņØ┤ ņĪ┤ņ×¼ĒĢśļ®░ ņĀĢĒÖĢĒĢ£ ANA ņ¢æņä▒ņ£©ņØä ļ¬©ļźĖļŗżļŖö ņĀÉņØ┤ ļģ╝ļ×ĆņØ┤ ļÉśĻ│Ā ņ׳Ļ│Ā, Ļ░Ćņżæņ╣ś ļČĆņŚ¼ ņ▓┤Ļ│äļź╝ ļÅäņ×ģĒĢśņŚ¼ ņŗżņĀ£ ņ¦äļŻī ĒśäņןņŚÉņä£ ņēĮĻ▓ī ņĀüņÜ®ĒĢśĻĖ░ ņ¢┤ļĀĄļŗżļŖö ļ¼ĖņĀ£ņĀÉņØ┤ ņ׳ļŗż. ņŚ¼ļ¤¼ ņØĖņóģ ļ░Å ņ¦ĆņŚŁņŚÉņä£ ņŚŁĒĢÖņĪ░ņé¼ņÖĆ ņ×äņāü ņŚ░ĻĄ¼ļź╝ ĒåĄĒĢ┤ ļČäļźś ĻĖ░ņżĆņØś ņ£ĀņÜ®ņä▒ ļ░Å ĒāĆļŗ╣ņä▒ņŚÉ ļīĆĒĢ£ Ļ▓Ćņ”ØņØ┤ ņ¦ĆņåŹļÉśņ¢┤ņĢ╝ ĒĢĀ Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






