


ņä£ ļĪĀ
ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉņŚÉņä£ ļ╣ä-ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁ ĒĢŁņØæĻ│ĀņĀ£(non-vitamin K antagonist oral anticoagulant, NOAC)ļŖö ĒÖ£ļ░£ĒĢśĻ▓ī ņé¼ņÜ®ļÉśĻ│Ā ņ׳Ļ│Ā, ĻĘĖ ņ▓śļ░®ņØ┤ ļŹö ļŖśņ¢┤ļéĀ Ļ▓āņ£╝ļĪ£ ņśłņāüļÉ£ļŗż. ņØ┤ņŚÉ ļ¦×ņČöņ¢┤ ļīĆĒĢ£ļČĆņĀĢļ¦źĒĢÖĒÜīņŚÉņä£ļŖö NOAC ņ▓śļ░®ņØś ņŗ£ņ×æĻ│╝ ņ£Āņ¦Ćņŗ£ ņŻ╝ņØśĒĢĀ ņĀÉņŚÉ ļīĆĒĢśņŚ¼ ņäżļ¬ģĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ļ│Ė ļĪĀ
NOAC ņé¼ņÜ®ņØ┤ ļÅäņøĆņØ┤ ļÉśļŖö ĒÖśņ×É
Ēśäņ×¼ ĻĄŁļé┤ ļ░Å ņÖĖĻĄŁņŚÉņä£ ļŗżļ╣äĻ░ĆĒŖĖļ×Ć, ņĢäĒöĮņé¼ļ░ś, ļ”¼ļ░öļĪØņé¼ļ░ś, ņŚÉļÅģņé¼ļ░ś ļō▒ņØś NOACĻ░Ć ļ╣äĒīÉļ¦ēņä▒ ņŗ¼ļ░®ņäĖļÅÖņŚÉņä£ ļćīņĪĖņżæ ņśłļ░®ņØä ņ£äĒĢśņŚ¼ ĒŚłĻ░ĆļÉśņ¢┤ ņé¼ņÜ®ļÉśĻ│Ā ņ׳ļŗż. NOACļŖö ņØĖĻ│Ą ĻĖ░Ļ│ä ĒīÉļ¦ē ļśÉļŖö ņżæļō▒ļÅä ņØ┤ņāüņØś ņŖ╣ļ¬©ĒīÉ Ēśæņ░®ņ”ØņØä Ļ░Ćņ¦ä ĒÖśņ×ÉņŚÉņä£ļ¦ī ĒÜ©Ļ│╝Ļ░Ć ņ×ģņ”ØļÉśņ¦Ć ņĢŖņĢśļŗż. ļö░ļØ╝ņä£ NOACļŖö ĻĘĖ ņÖĖ ļ¬©ļōĀ ĒīÉļ¦ē ņ¦łĒÖśņŚÉņä£ļŖö ĒÜ©Ļ│╝ņĀüņ£╝ļĪ£ ņé¼ņÜ®ņØ┤ Ļ░ĆļŖźĒĢśļŗż(Table 1) [1-3]. ņĄ£ĻĘ╝ ļ░£Ēæ£ļÉ£ 2016 European Society of Cardiology ņ¦äļŻī ņ¦Ćņ╣©ņŚÉņä£ļŖö ŌĆśļ╣äĒīÉļ¦ēņä▒ŌĆÖņØ┤ļØ╝ļŖö ņÜ®ņ¢┤Ļ░Ć ņéŁņĀ£ļÉśņŚłņ£╝ļ®░, ļīĆĒĢ£ļČĆņĀĢļ¦źĒĢÖĒÜī ņŗżņÜ® ņ¦Ćņ╣©ņŚÉņä£ļÅä Ēś╝ļÅÖņØä Ēö╝ĒĢśĻĖ░ ņ£äĒĢśņŚ¼ ŌĆ£ļ╣äĒīÉļ¦ēņä▒ŌĆØņØ┤ļ×Ć ņÜ®ņ¢┤ļź╝ ņéŁņĀ£ĒĢśņśĆļŗż[1,3]. ĒĢśņ¦Ćļ¦ī ņØ┤ ņÜ®ņ¢┤ļŖö ņ×äņāü ņŚ░ĻĄ¼ņØś ņĀ£ņÖĖ ĻĖ░ņżĆņŚÉ ĒżĒĢ©ļÉ£ ņĄ£ņ┤łņØś ļŗ©ņ¢┤ņØ┤ĻĖ░ ļĢīļ¼ĖņŚÉ Ļ░ü NOACņØś ņĀ£ĒÆł ĒŖ╣ņä▒ ņÜöņĢĮņŚÉ ĻĖ░ņłĀļÉśņ¢┤ ņ׳ļŗż.
ņĄ£ĻĘ╝ņŚÉļŖö ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£(vitamin K antagonist; ļīĆĒĢ£ļ»╝ĻĄŁņŚÉņä£ļŖö ņÖĆĒīīļ”░ļ¦īņØ┤ ņé¼ņÜ® Ļ░ĆļŖźĒĢśļ»ĆļĪ£, ņÖĆĒīīļ”░ņ£╝ļĪ£ ĻĖ░ņłĀĒĢ©)ņØś ņé¼ņÜ®ņØ┤ ĒĢäņÜöĒĢ£ ĒīÉļ¦ē ņ¦łĒÖś ĒÖśņ×Éļź╝ evaluated heat valves, rheumatic or artificial (EHRA) 1ĒśĢ, ĻĘĖļ”¼Ļ│Ā NOAC ļ░Å ņÖĆĒīīļ”░ ņāüņÜ®ņØ┤ ļ¬©ļæÉ Ļ░ĆļŖźĒĢ£ ĒÖśņ×Éļź╝ EHRA 2ĒśĢņ£╝ļĪ£ ļČäļźśĒĢśĻĖ░ļÅä ĒĢ£ļŗż[3]. EHRA 2ĒśĢņØĆ ņÖĆĒīīļ”░ ļśÉļŖö NOACļĪ£ ĒśłņĀäņāēņĀäņ”Ø ņśłļ░®ņØ┤ ĒĢäņÜöĒĢ£ ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉļōżņØ┤ļ®░, ņżæļō▒ļÅä ņØ┤ņāüņØś ņŖ╣ļ¬©ĒīÉ Ēśæņ░®ņØä ņĀ£ņÖĖĒĢ£ ļ¬©ļōĀ ĒīÉļ¦ē ņ¦łĒÖś, ņŖ╣ļ¬©ĒīÉ ņä▒ĒśĢņłĀ, ņĪ░ņ¦ü ĒīÉļ¦ē ņ╣śĒÖś ļśÉļŖö Ļ▓ĮĒö╝ņĀü ļīĆļÅÖļ¦ź ĒīÉļ¦ē ņżæņ×¼ņłĀ(trans-catheter aortic valve implantation)ņØä ĒżĒĢ©ĒĢ£ļŗż[3]. EHRA 2ĒśĢ ĒÖśņ×ÉĻĄ░ņØĆ NOAC ļ¼┤ņ×æņ£ä ņŚ░ĻĄ¼ļōżņŚÉ ĒżĒĢ©ļÉśņ¢┤ ņ׳Ļ│Ā, ņÖĆĒīīļ”░Ļ│╝ ļ╣äņŖĘĒĢ£ ĒÜ©ļŖź ļ░Å ņĢłņĀĢņä▒ņØä ļ│┤ņśĆĻĖ░ ļĢīļ¼ĖņŚÉ[3-9], ņØ┤ļōż ĒÖśņ×ÉņŚÉņä£ļŖö NOACĻ░Ć ņé¼ņÜ®ļÉĀ ņłś ņ׳ļŗż(Table 1) [1,3,10]. ĒĢśņ¦Ćļ¦ī, ņĪ░ņ¦üĒīÉļ¦ē ņ╣śĒÖśņłĀ ļśÉļŖö ĒīÉļ¦ē ņä▒ĒśĢņłĀņØä ņŗ£Ē¢ēļ░øņØĆ ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉņØś ņ╣śļŻīņŚÉ ļīĆĒĢ┤ņä£ļŖö ļģ╝ļ×ĆņØ┤ ņ׳ļŗż[3,6,7,11]. ĒīÉļ¦ē ņ╣śĒÖśņłĀ ņ×Éņ▓┤ļĪ£ ņןĻĖ░Ļ░äņØś Ļ▓ĮĻĄ¼ ĒĢŁņØæĻ│ĀņĀ£ ņ╣śļŻīĻ░Ć ļīĆļČĆļČäņØś ĒÖśņ×ÉņŚÉņä£ ĒĢäņÜöĒĢśņ¦Ć ņĢŖņ¦Ćļ¦ī, ļÅÖļ░śļÉ£ ņŗ¼ļ░®ņäĖļÅÖņØś ņ╣śļŻīļź╝ ņ£äĒĢ£ NOACņØś ņé¼ņÜ®ņØĆ ĒāĆļŗ╣ĒĢ£ ņ╣śļŻī ņśĄņģśņØ┤ļŗż. ļźśļ¦łĒŗ░ņŖżņä▒ ņŖ╣ļ¬©ĒīÉ Ēśæņ░®ņ”ØņŚÉ ņĪ░ņ¦üĒīÉļ¦ē ņ╣śĒÖśņłĀņØä ņŗ£Ē¢ēĒĢ£ Ļ▓ĮņÜ░ļŖö ņśłņÖĖņŚÉ ĒĢ┤ļŗ╣ĒĢ£ļŗż. ņØ┤ ĒÖśņ×ÉļōżņŚÉņä£ ņŖ╣ļ¬©ĒīÉ ņ╣śĒÖśņłĀ Ēøä ņŖ╣ļ¬©ĒīÉ ĒśłļźśļŖö ņĀĢņāüĒÖöļÉśņ¦Ćļ¦ī ņŗ¼ļ░®ņØĆ ņŚ¼ņĀäĒ׳ ĒÖĢņןļÉśņ¢┤ ņ׳Ļ│Ā ļ╣äņĀĢņāüņĀüņØ┤ļŗż. ļö░ļØ╝ņä£, ņÖĆĒīīļ”░ņØ┤ ņäĀĒśĖļÉśļŖö ņśĄņģśņØ┤ņ¦Ćļ¦ī ņČöĻ░Ć ņŚ░ĻĄ¼Ļ░Ć ĒĢäņÜöĒĢśļŗż.
Ļ▓ĮĒö╝ņĀü ļīĆļÅÖļ¦ź ĒīÉļ¦ē ņŗ£ņłĀ ņØ┤Ēøä NOAC ņé¼ņÜ®ņŚÉ ļīĆĒĢ£ ņĀäĒ¢źņĀüņØĖ ņŚ░ĻĄ¼ļŖö ņŚåĻ│Ā, ņØ┤ļōż ĒÖśņ×ÉņŚÉņä£ļŖö ĒĢŁĒśłņåīĒīÉņĀ£ ļŗ©ļÅģ ļśÉļŖö ļ│ĄĒĢ® ņÜöļ▓ĢņØ┤ ĒĢäņÜöĒĢśļŗż[2]. Ļ▓ĮĻĄ¼ ĒĢŁņØæĻ│ĀņĀ£ņØś ņČöĻ░ĆļŖö ņČ£Ēśł ņ£äĒŚśņØä ņāüņŖ╣ņŗ£ĒéżĻ│Ā ņĀüņĀłĒĢ£ ņĪ░ĒĢ® ļ░Å ĻĖ░Ļ░äņŚÉ ļīĆĒĢ┤ņä£ļŖö ņ¦äĒ¢ē ņżæņØĖ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļź╝ ĻĖ░ļŗżļĀż ļ│┤ņĢäņĢ╝ ĒĢ£ļŗż.
ļ╣äĒøäņä▒ ņŗ¼ĻĘ╝ņ”Ø ĒÖśņ×ÉņŚÉņä£ ņŗ¼ļ░®ņäĖļÅÖņØĆ ĒśłņĀäņāēņĀäņ”ØņØś ņ£äĒŚśņØĖņ×ÉņØ┤ļŗż[12,13]. ĻĖ░Ļ│ä ĒīÉļ¦ē ļśÉļŖö ļźśļ¦łĒŗ░ņŖżņä▒ ņŖ╣ļ¬©ĒīÉ Ēśæņ░®ņ”ØĻ│╝ ļŗ¼ļ”¼ NOACĻ░Ć ņÖĆĒīīļ”░Ļ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ņŚ┤ļō▒ĒĢśļŗżĻ│Ā ņČöļĪĀĒĢĀ ļ¦īĒĢ£ ĒĢ®ļ”¼ņĀüņØĆ ĻĘ╝Ļ▒░Ļ░Ć ņŚåļŗż. ļ░śļīĆļĪ£ ļ╣äĒøäņä▒ ņŗ¼ĻĘ╝ļ│æņ”ØņŚÉ ļÅÖļ░śļÉ£ ņŗ¼ļ░®ņäĖļÅÖņØĆ ņóīņŗ¼ņŗż ĻĄ¼ĒśłļźĀņØ┤ ņ£Āņ¦ĆļÉ£ ņŗ¼ļČĆņĀä ĒÖśņ×ÉņŚÉņä£ņØś ņŗ¼ļ░®ņäĖļÅÖĻ│╝ ļ¦ÄņØĆ ņ£Āņé¼ņä▒ņØ┤ ņ׳Ļ│Ā, ļåÆņØĆ CHA2DS2-VASC ņĀÉņłś ĒÖśņ×ÉņŚÉņä£ NOACņØś ĒÜ©Ļ│╝Ļ░Ć ņ”Øļ¬ģļÉśņŚłņ£╝ļ»ĆļĪ£, NOAC ņ╣śļŻīļŖö ņĀüņĀłĒĢśļŗżĻ│Ā ĒĢĀ ņłś ņ׳ļŗż[14-16].
NOACļź╝ ņé¼ņÜ®ĒĢśļŖö ĒÖśņ×ÉņØś ņĢĮņĀ£ ņŗ£ņ×æ ļ░Å ņČöņĀü Ļ┤Ćņ░░ Ļ│äĒÜŹ
ĒĢŁņØæĻ│Ā ņ╣śļŻīņØś ņĀüņØæņ”Ø ļ░Å ņÖĆĒīīļ”░Ļ│╝ NOACņØś ņäĀĒāØ
ĒĢŁņØæĻ│Ā ņ╣śļŻī ņĀüņØæņØ┤ ļÉśļŖö ĒÖśņ×É ņäĀņĀĢ ļ░Å ņÖĆĒīīļ”░Ļ│╝ NOACņØś ņäĀĒāØņØĆ ņŻ╝ņØśĻ░Ć ĒĢäņÜöĒĢśļ®░ ņ¦äļŻī ņ¦Ćņ╣©ņØ┤ ļÅäņøĆņØ┤ ļÉĀ ņłś ņ׳ļŗż. ļ¬©ļōĀ NOACļŖö ņŗĀĻĖ░ļŖźņŚÉ ļö░ļźĖ ņÜ®ļ¤ē ņĪ░ņĀłņØ┤ ĒĢäņÜöĒĢśĻ│Ā ņŗ¼ĒĢ£ ņŗĀĻĖ░ļŖź ņĀĆĒĢśņŚÉņä£ļŖö ņé¼ņÜ®ņØ┤ ĻĖłņ¦ĆļÉśņ¢┤ ņ׳ĻĖ░ ļĢīļ¼ĖņŚÉ, ņŗĀĻĖ░ļŖźņŚÉ ļīĆĒĢ£ ņĀĢļ│┤Ļ░Ć ĒĢäņÜöĒĢśļŗż. ļśÉĒĢ£ Ļ░ü ņĢĮņĀ£ļ¦łļŗż ļ│┤ņ£ĀĒĢśĻ│Ā ņ׳ļŖö Ļ│Āņ£ĀņØś ĒŖ╣ņä▒, ĒÖśņ×É Ļ░£Ļ░£ņØĖņØś ņ×äņāü ņÜöņØĖ, ĒÖśņ×ÉņØś ņäĀĒśĖļÅä ļ¬©ļæÉĻ░Ć Ļ│ĀļĀżļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż[17-19].
ļīĆĒĢ£ļČĆņĀĢļ¦źĒĢÖĒÜī ņŗ¼ļ░®ņäĖļÅÖ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņØĆ ĒŖ╣Ē׳ ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉņŚÉņä£ ļćīņĪĖņżæ ņśłļ░®ņØä ņ£äĒĢśņŚ¼ ĒĢŁņØæĻ│Ā ņ╣śļŻīļź╝ ņŗ£ņ×æĒĢśļŖö ĒÖśņ×ÉņØś Ļ▓ĮņÜ░, NOACņØś ņóģĒĢ®ņĀüņØĖ ņ×äņāüņĀü ņØ┤ļōØņŚÉ ļ░öĒāĢĒĢśņŚ¼, NOACņØś ĒŖ╣ļ│äĒĢ£ ĻĖłĻĖ░ņ”ØņØ┤ ņŚåļŖö ĒĢ£ ņÖĆĒīīļ”░ļ│┤ļŗż NOACļź╝ ņäĀĒśĖĒĢśĻ│Ā ņ׳ļŗż(class I, level of evidence A) [20].
NOAC ņóģļźś ļ░Å ņÜ®ļ¤ēņØś ņäĀĒāØ
ĻĄŁļé┤ņŚÉņä£ļŖö ļŗżļ╣äĻ░ĆĒŖĖļ×Ć, ļ”¼ļ░öļĪØņé¼ļ░ś, ņĢäĒöĮņé¼ļ░ś, ņŚÉļÅģņé¼ļ░ś ļō▒ ņĀä ņäĖĻ│äņĀüņ£╝ļĪ£ ņŗ£ĒīÉļÉśĻ│Ā ņ׳ļŖö ļäż Ļ░Ćņ¦Ć ļ¬©ļōĀ NOACĻ░Ć ņ▓śļ░® Ļ░ĆļŖźĒĢśĻ│Ā, Ļ░üĻ░üņØś ņÜ®ļ¤ē Ļ░Éļ¤ē ĻĖ░ņżĆņŚÉ ļö░ļØ╝ ņĀüņĀłĒĢ£ ņÜ®ļ¤ēņ£╝ļĪ£ ņ▓śļ░® Ļ░ĆļŖźĒĢśļŗż. ĻĄŁļé┤ ļ│┤ĒŚś ĻĖ░ņżĆņ£╝ļĪ£ļŖö CHA2DS2-VASc ņĀÉņłśĻ░Ć 2ņĀÉ ņØ┤ņāüņØĖ Ļ▓ĮņÜ░ ĻĖēņŚ¼ ņØĖņĀĢņØ┤ ļÉ£ļŗż. ļäż Ļ░Ćņ¦Ć NOAC ļ¬©ļæÉ ļīĆĻĘ£ļ¬© ļ¼┤ņ×æņ£ä ņ×äņāü ņŗ£ĒŚśņŚÉņä£ ĒÜ©ļŖźĻ│╝ ņĢłņĀäņä▒ņØ┤ ņ×ģņ”ØļÉśņŚłļŗż. Apixaban for reduction in stroke and other thromboembolic events in atrial fibrillation (ARISTOTLE, ņĢäĒöĮņé¼ļ░ś)Ļ│╝ ROCKET-AF (ļ”¼ļ░öļĪØņé¼ļ░ś) ņŚ░ĻĄ¼ņŚÉņä£ļŖö ĻĖ░ļ│ĖņĀüņ£╝ļĪ£ ĒĢ£ Ļ░Ćņ¦Ć ņÜ®ļ¤ēņØ┤ ņŻ╝ ņÜ®ļ¤ēņ£╝ļĪ£ ņŚ░ĻĄ¼ļÉśĻ│Ā ĒÖśņ×É ĒŖ╣ņä▒ņŚÉ ļö░ļØ╝ ņÜ®ļ¤ēņØä Ļ░Éļ¤ēĒĢśļÅäļĪØ ņäżĻ│äļÉśņŚłļŗż[21,22]. ņØ┤ņŚÉ ļ░śĒĢśņŚ¼ randomized evaluation of long-term anticoagulation therapy (RE-LY, ļŗżļ╣äĻ░ĆĒŖĖļ×Ć)ņÖĆ Effective Anticoagulation with Factor Xa Next Generation in Atrial Fibrillation (ENGAGE-AF, ņŚÉļÅģņé¼ļ░ś) ņŚ░ĻĄ¼ļŖö Ļ│ĀņÜ®ļ¤ē, ņĀĆņÜ®ļ¤ē ĻĄ░ņŚÉ ļ¬©ļæÉ ņČ®ļČäĒĢ£ ĒÖśņ×É ņłśļź╝ ļ░░ņĀĢĒĢśņŚ¼ ņŚ░ĻĄ¼Ļ░Ć ņäżĻ│äļÉśņŚłĻ│Ā ņŚÉļÅģņé¼ļ░śņØś Ļ▓ĮņÜ░ņŚÉļŖö Ļ│ĀņÜ®ļ¤ē, ņĀĆņÜ®ļ¤ē ĻĄ░ ļé┤ņŚÉņä£ ĒŖ╣ņĀĢ ĒŖ╣ņä▒ņØä Ļ░Ćņ¦ä ĒÖśņ×ÉņŚÉņä£ ņÜ®ļ¤ēņØä Ļ░Éļ¤ēĒĢśļÅäļĪØ ņäżĻ│äļÉśņŚłļŗż[23,24]. Ļ░ĆļŖźĒĢ£ Ēæ£ņżĆ ņÜ®ļ¤ēņØś NOACļź╝ ņé¼ņÜ®ĒĢ┤ņĢ╝ ĒĢśļ®░, ņÜ®ļ¤ē ņĪ░ņĀłņØĆ ŌĆś2018 ļīĆĒĢ£ļČĆņĀĢļ¦źĒĢÖĒÜī ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉņŚÉņä£ ĒĢŁņØæĻ│ĀņĀ£ņØś ņĀüĒĢ®ĒĢ£ ņäĀĒāØ ļ░Å ņÜ®ļ¤ē ĻČīĻ│ĀņĢłŌĆÖņŚÉ ļö░ļØ╝ ņŗ£Ē¢ēĒĢ£ļŗż[25]. ĒÖśņ×ÉĻ░Ć ĒĢ©Ļ╗ś ļ│ĄņÜ®ĒĢśĻ│Ā ņ׳ļŖö ņĢĮņĀ£ņŚÉ ļīĆĒĢ£ Ļ▓ĆĒåĀĻ░Ć ĒĢäņÜöĒĢśļ®░ ņĢĮņĀ£ Ļ░ä ņāüĒśĖņ×æņÜ®ļÅä Ļ│ĀļĀżĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż. ļśÉĒĢ£ ĒÖśņ×ÉņØś ļéśņØ┤, ņ▓┤ņżæ, ņŗĀĻĖ░ļŖź, ļŗżļźĖ ļÅÖļ░ś ņ¦łĒÖśļÅä Ļ│ĀļĀżļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż. Ļ│╝Ļ▒░ ņ£äņןĻ┤Ć ņČ£ĒśłņØ┤ļéś ĻČżņ¢æņØ┤ ņ׳ņŚłļŹś ĒÖśņ×Éļéś ĒĢŁĒśłņåīĒīÉ ņĢĮņĀ£ņØś ļ│ĄņĢĮņØ┤ ĒĢ©Ļ╗ś ĒĢäņÜöĒĢ£ Ļ▓ĮņÜ░ņŚÉļŖö ņ£äņןĻ┤Ć ņČ£ĒśłņØś ņ£äĒŚśļÅä Ļ░Éņåīļź╝ ņ£äĒĢśņŚ¼ ĒöäļĪ£Ēåż ĒÄīĒöä ņ¢ĄņĀ£ņĀ£(proton pump inhibitor, PPI) ļ│ĄņÜ®ņØä Ļ│ĀļĀżĒĢ£ļŗż[26,27]. PPIņØś ņé¼ņÜ®ņØĆ ņÖĆĒīīļ”░ņØ┤ļéś ĒĢŁĒśłņåīĒīÉ ņĢĮņĀ£ ņé¼ņÜ®ņŚÉņä£ ņ£äņן ļ│┤ĒśĖ ĒÜ©Ļ│╝Ļ░Ć ņ”Øļ¬ģļÉśņŚłņ£╝ļéś, NOACņŚÉņä£ņØś ļŹ░ņØ┤Ēä░ļŖö ņĀ£ĒĢ£ņĀüņØ┤ļŗż[28-31]. ĒÖśņ×Éļ│ä ĒŖ╣ņä▒ņŚÉ ļö░ļØ╝ NOAC ņóģļźś ņäĀĒāØņŚÉ ļÅäņøĆņØä ņŻ╝ļŖö ņ¦äļŻī ņ¦Ćņ╣©ņØä ņ░ĖĻ│ĀĒĢśĻĖ░ ļ░öļ×Ćļŗż[32-35].
NOAC ļ│ĄņÜ®ņØä ņ£äĒĢ£ ĒĢŁņØæĻ│Ā ņ╣śļŻī ņ╣┤ļō£ ļ░Å ĻĄÉņ£ĪņØś ņżæņÜöņä▒
ņÖĆĒīīļ”░ņØä ļ│ĄņÜ®ĒĢśļŖö ĒÖśņ×ÉļōżĻ│╝ ļ¦łņ░¼Ļ░Ćņ¦ĆļĪ£ NOACļź╝ ļ│ĄņÜ®ĒĢśļŖö ĒÖśņ×ÉļōżļÅä ņ╣śļŻīņŚÉ ļīĆĒĢ£ ņāüņäĖĒĢ£ ĻĄÉņ£ĪņØĆ ņżæņÜöĒĢśļŗż. ņØ┤ņŚÉ ļö░ļØ╝ ļīĆĒĢ£ļČĆņĀĢļ¦źĒĢÖĒÜīņŚÉņä£ ņĀ£ņŗ£ĒĢśļŖö ĒåĄņØ╝ļÉ£ NOAC ĒÖśņ×É Ļ┤Ćļ”¼ ņ╣┤ļō£ ņé¼ņÜ®ņØä ņČöņ▓£ĒĢ£ļŗż(Figs. 1 and 2).
ļ¦ż ņ¦äļŻīļ¦łļŗż ĒÖśņ×ÉņŚÉĻ▓ī ļ│ĄņÜ®ļ▓ĢņØä ĻĄÉņ£ĪĒĢśĻ│Ā, ļ│ĄņĢĮ ņł£ņØæļÅäļź╝ ĒÖĢņØĖņØ┤ ņżæņÜöĒĢśļŗż. ļśÉĒĢ£ ņĢĮņØä Ļ╣£ļ░ĢĒĢśĻ│Ā ļ│ĄņÜ®ĒĢśņ¦Ć ļ¬╗ĒĢśņśĆņØä ļĢī ņ¢┤ļ¢╗Ļ▓ī ĒĢ┤ņĢ╝ ĒĢśļŖöņ¦Ć ĻĄÉņ£ĪĒĢ┤ņĢ╝ ĒĢśļ®░, ņŚ¼Ē¢ēņŗ£ņŚÉ ņĢĮņØä ĒĢŁņāü ņ¦Ćņ░ĖĒĢśļŖö Ļ▓āņØä Ļ░ĢņĪ░ĒĢśļŖö Ļ▓āņØ┤ ņżæņÜöĒĢśļŗż. NOAC ĒÖśņ×É Ļ┤Ćļ”¼ ņ╣┤ļō£ņŚÉ ņØ┤ļ¤¼ĒĢ£ ņŻ╝ņÜö ņé¼ĒĢŁļōżņØ┤ ĒżĒĢ©ļÉśņ¢┤ ņ׳ļŗż. ņ×ÉņäĖĒĢ£ ĒÖśņ×É ĻĄÉņ£ĪņØä ņ£äĒĢśņŚ¼ ļŗżņØīņØś ņ░ĖĻ│Āļ¼ĖĒŚīņØä ņØ┤ņÜ®ĒĢĀ ņłś ņ׳Ļ▓Āļŗż[17,19,36,37].
ņČöņĀü Ļ┤Ćņ░░
ĒĢŁņØæĻ│Ā ņ╣śļŻīļź╝ ļ░øļŖö ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉļŖö ņäĖņŗ¼ĒĢ£ ņĀĢĻĖ░ņĀü ņČöņĀü Ļ┤Ćņ░░ņØ┤ ĒĢäņÜöĒĢśļŗż. ņĢĮļ¼╝ ņāüĒśĖņ×æņÜ®ņ£╝ļĪ£ ņČ£ĒśłņØ┤ ņĪ░ņןļÉĀ ņłśļÅä Ēś╣ņØĆ ļćīņĪĖņżæņØä ņśłļ░®ĒĢśļŖö ĒÜ©Ļ│╝Ļ░Ć Ļ░ÉņåīļÉĀ ņłśļÅä ņ׳ļŗż. ĒŖ╣Ē׳ ĒÖśņ×ÉĻ░Ć Ļ│ĀļĀ╣ņØ┤Ļ▒░ļéś ĒŚłņĢĮĒĢĀ Ļ▓ĮņÜ░ ļ░£ņāØ Ļ░ĆļŖźĒĢ£ ĒĢ®ļ│æņ”ØņŚÉ ļīĆĒĢśņŚ¼ ĒĢŁņāü ņŻ╝ņØśĒĢ┤ņĢ╝ ĒĢ£ļŗż. ņĢĮņĀ£ļź╝ ņŗ£ņ×æĒĢ£ ņØ┤Ēøä ĒĢ£ ļŗ¼ ļÆż ņĀĢĻĖ░ ļ░®ļ¼ĖņØä ņČöņ▓£ĒĢśĻ│Ā ņØ┤ĒøäļČĆĒä░ļŖö ņĀüņ¢┤ļÅä 3Ļ░£ņøöņŚÉ ĒĢ£ ļ▓ł ņĀĢĻĖ░ņĀüņ£╝ļĪ£ ņ¦äļŻīĒĢśļŖö Ļ▓āņØä ņČöņ▓£ĒĢ£ļŗż. NOAC ņ▓śļ░® Ļ▓ĮĒŚśņØ┤ ņīōņØ┤ļ®┤ ĒÖśņ×É ĒŖ╣ņä▒ņØ┤ļéś ņ¦äļŻī ĻĖ░Ļ┤ĆņØś ĒŖ╣ņä▒ņØä Ļ│ĀļĀżĒĢśņŚ¼ ņĀĢĻĖ░ņĀü ņČöņĀü Ļ┤Ćņ░░ ĻĖ░Ļ░äņØä ļŹö ĻĖĖĻ▓ī ņäżņĀĢĒĢĀ ņłśļÅä ņ׳Ļ▓Āļŗż(Fig. 3) [38,39].
Ēæ£ 2ņÖĆ ĻĘĖļ”╝ 3ņŚÉ ņāüĒÖ®ņŚÉ ļö░ļźĖ ņĀüņĀłĒĢ£ ņČöņĀü Ļ┤Ćņ░░ ņŗ£ņĀÉņŚÉ ļīĆĒĢśņŚ¼ ĻĖ░ņłĀĒĢśņśĆļŗż. Ļ░Ćņן ņżæņÜöĒĢ£ ņĀÉņØĆ ĒÖśņ×É ĒŖ╣ņä▒ņŚÉ ļīĆĒĢ£ Ļ│ĀļĀżņØ┤ļŗż. ņśłļź╝ ļōżņ¢┤, Ļ│ĀļĀ╣ņØ┤Ļ▒░ļéś(75ņäĖ ņØ┤ņāü), ĒŚłņĢĮĒĢ£ ĒÖśņ×É, Ļ░äĻĖ░ļŖźņØ┤ļéś ņŗĀĻĖ░ļŖźņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣Ā ņłś ņ׳ļŖö ļÅÖļ░śļÉ£ Ļ░ÉņŚ╝ņØ┤ļéś ņĢöņØ┤ ņ׳ļŖö ĒÖśņ×ÉņŚÉņä£ļŖö ņŗĀĻĖ░ļŖźņØä ņóĆ ļŹö ņ×ÉņŻ╝ ĒÅēĻ░ĆĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż[40,41]. ļśÉĒĢ£ ļćīņĪĖņżæ ņ£äĒŚśļÅäļŖö ņŗ£Ļ░äņØ┤ ņ¦Ćļé©ņŚÉ ļö░ļØ╝ ļ│ĆĒĢĀ ņłś ņ׳ĻĖ░ ļĢīļ¼ĖņŚÉ ĒÖśņ×É ļ░®ļ¼Ėņŗ£ ļ¦łļŗż ņ×¼ĒÅēĻ░ĆĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż[42]. ņČ£Ēśł ņ£äĒŚśļÅäļÅä ļ¦łņ░¼Ļ░Ćņ¦ĆļĪ£ ņóģĒĢ®ņĀüņ£╝ļĪ£ ĒÅēĻ░ĆļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż[43-47]. ĒĢśņ¦Ćļ¦ī ļåÆņØĆ ņČ£Ēśł ņ£äĒŚśļÅä ņ×Éņ▓┤Ļ░Ć ĒĢŁņØæĻ│Ā ņ╣śļŻīņØś ĻĖłĻĖ░ņ”ØņØĆ ņĢäļŗłļŗż. ĻĘĖ ņØ┤ņ£ĀļŖö ņČ£Ēśł ņ£äĒŚśņŚÉ ļ╣äļĪĆĒĢśņŚ¼ ļćīņĪĖņżæ ņ£äĒŚśļÅäļÅä ņ”ØĻ░ĆĒĢśĻĖ░ ļĢīļ¼ĖņØ┤ļŗż[17,48]. ņØ╝ļŗ© ĻĄÉņĀĢ Ļ░ĆļŖźĒĢ£ ņ£äĒŚśņØĖņ×Éļź╝ ņĄ£ļīĆĒĢ£ ĻĄÉņĀĢĒĢśļŖö Ļ▓āņØ┤ ņČöņ▓£ļÉ£ļŗż. ļśÉĒĢ£ ļģĖņćĀĒĢ©ņØ┤ļéś ļéÖņāü ņ£äĒŚśņØĆ ĒĢŁņØæĻ│ĀņĀ£ ņé¼ņÜ®ņØś ĻĖłĻĖ░ņ”ØņØ┤ ņĢäļŗłļ®░, ĒÖśņ×ÉņŚÉĻ▓ī ņĀüĒĢ®ĒĢ£ ņĄ£ņāüņØś ĒĢŁņØæĻ│ĀņĀ£ ņóģļźś ļ░Å ņÜ®ļ¤ēņØä ņäĀĒāØĒĢśņŚ¼ ņČ®ļČäĒĢ£ ĒÖśņ×É ĻĄÉņ£Ī ļ░Å ņĀüņĀłĒĢ£ ņČöņĀü Ļ┤Ćņ░░ņØä ĒĢśļŖö Ļ▓āņØ┤ ņČöņ▓£ļÉ£ļŗż.
ĒĢŁņØæĻ│ĀņĀ£ņØś ļ│ĄņĢĮ ņł£ņØæļÅä
ņ¦¦ņØĆ ņĢĮņĀ£ ļ░śĻ░ÉĻĖ░ļź╝ Ļ│ĀļĀżĒĢśņśĆņØä ļĢī NOACņØś ļ│ĄņÜ® ņł£ņØæļÅäļŖö ĒĢŁņØæĻ│Ā ĒÜ©Ļ│╝ļź╝ ņ£Āņ¦ĆĒĢśļŖöļŹ░ ĒĢäņłśņĀüņØ┤ļŗż[49]. ņÖ£ļāÉĒĢśļ®┤, ļ│ĄņĢĮ 12-24ņŗ£Ļ░ä ļé┤ņŚÉ ņĀÉņ░©ņĀüņ£╝ļĪ£ ĒĢŁņØæĻ│Ā ĒÜ©Ļ│╝Ļ░Ć Ļ░ÉņåīĒĢśĻĖ░ ļĢīļ¼ĖņØ┤ļŗż. NOAC ļ│ĄņĢĮ ņł£ņØæļÅä ĒÅēĻ░Ćļź╝ ņĢĮņĀ£ Ēśłņżæ ļåŹļÅäļéś ņØ╝ļ░śņĀüņØĖ ņØæĻ│Ā Ļ▓Ćņé¼ļĪ£ ņŗ£Ē¢ēĒĢ©ņØĆ ļ¬©ļæÉ ņĀüĒĢ®ĒĢśņ¦Ć ņĢŖļŗż. ĒŖ╣Ē׳ ļÅÖļ░ś ņ¦łĒÖśņØ┤ ļ¦ÄĻ▒░ļéś Ļ│ĀļĀ╣ņØ┤Ļ▒░ļéś ņŗĀĻĖ░ļŖź ņĀĆĒĢśĻ░Ć ņ׳Ļ▒░ļéś ļģĖņćĀĒĢ£ ĒÖśņ×ÉņØś Ļ▓ĮņÜ░ NOACļź╝ ļ│ĄņÜ®ĒĢśļŹöļØ╝ļÅä ņĀĢĻĖ░ņĀü ņČöņĀü Ļ┤Ćņ░░ņØ┤ ĒĢäņłśņĀüņØ┤ļŗż.
ņŗżņĀ£ ņ¦äļŻī ĒÖśĻ▓ĮņŚÉņä£ NOAC ļ│ĄņĢĮ ņł£ņØæļÅäļŖö 38%ņŚÉņä£ 99%ļĪ£ ļ│┤Ļ│ĀļÉ£ļŗż[50-61]. NOAC ļ│ĄņÜ®ņØś ļé«ņØĆ ņł£ņØæļÅäļŖö ņ╣śļŻīļĪ£ ņ¢╗ņØä ņłś ņ׳ļŖö ņØ┤ļōØņØä ņŗ¼ĒĢśĻ▓ī Ļ░Éņåīņŗ£Ēé©ļŗż. ņĄ£ĻĘ╝ ŌĆśņŗżņĀ£ ņ¦äļŻī ĒÖśĻ▓ĮŌĆÖ ļŹ░ņØ┤Ēä░ ļČäņäØ Ļ▓░Ļ│╝ņŚÉņä£ ņÖĆĒīīļ”░ņŚÉ ļ╣äĒĢśņŚ¼ NOACņØś ņØ┤ļōØņØ┤ ņ×äņāü ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ņÖĆ Ļ░ÖņØ┤ ņØ╝Ļ┤ĆļÉśĻ▓ī ļ│┤Ļ│ĀļÉśņŚłļŗżļŖö ņĀÉņ£╝ļĪ£ ļ»ĖļŻ©ņ¢┤, ņŗżņĀ£ ņ¦äļŻī ĒÖśĻ▓ĮņŚÉņä£ņØś ļ│ĄņĢĮ ņł£ņØæļÅäĻ░Ć ņÜ░ļĀżĒĢśņśĆļŹś ļ¦īĒü╝ ļ¦żņÜ░ ļé«ņ¦Ć ņĢŖĻ│Ā, ļīĆļץ ņĀüņĀłĒĢśņśĆņØīņØä ņČöņĀĢĒĢĀ ņłś ņ׳ļŗż[56,62-81]. ĻĘĖļ¤╝ņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā, ļ│ĄņĢĮ ņżæļŗ©ņ£©ņØĆ NOAC ĒÖśņ×É Ļ┤Ćļ”¼ņŚÉ ņ׳ņ¢┤ņä£ ņŚ¼ņĀäĒ׳ ļ¼ĖņĀ£ņØ┤ļŗż[51,59,60,67,78,82-89]. ļö░ļØ╝ņä£, NOAC ļ│ĄņĢĮ ņł£ņØæļÅäļź╝ ņ”Øņ¦äņŗ£ĒéżĻĖ░ ņ£äĒĢ┤ņä£ļŖö ļ¬©ļōĀ Ļ░ĆļŖźĒĢ£ ļ░®ļ▓ĢņØä ļ¬©ļæÉ Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢśļ®░, ņĢäļלņÖĆ Ļ░ÖņØĆ ņ¦Ćņ╣©ņØä ņĀ£ņŗ£ĒĢ£ļŗż.
ļ│ĄņĢĮ ņł£ņØæļÅä Ē¢źņāüņØä ņ£äĒĢ£ ņŗżņÜ®ņĀü ņ¦Ćņ╣©(Fig. 3)
1) ĒĢŁņØæĻ│Āņ╣śļŻīļź╝ ļ░øļŖö ĒÖśņ×ÉņŚÉ ļīĆĒĢ£ ņØ╝ļ░śņĀüņØĖ ĻĄÉņ£ĪĻ│╝ ņĢĮņĀ£ ļ│ĄņĢĮ ņł£ņØæļÅäņØś ņżæņÜöņä▒ņŚÉ ļīĆĒĢ£ ĻĄÉņ£ĪņØ┤ Ļ░Ćņן ņżæņÜöĒĢśļŗż[18,19,36,37,90,91]. 2) ĒÖśņ×ÉņØś Ļ░ĆņĪ▒ļōżļÅä ļ│ĄņĢĮ ņł£ņØæļÅäņØś ņżæņÜöņä▒ņØä ņØ┤ĒĢ┤ĒĢĀ ņłś ņ׳ļÅäļĪØ ĒĢśĻ│Ā ĒÖśņ×Éļź╝ ļÅäņÜĖ ņłś ņ׳ļÅäļĪØ ĻĄÉņ£ĪĒĢ£ļŗż. 3) NOACļź╝ ļ│ĄņÜ®ĒĢśļŖö ĒÖśņ×ÉņØś ņČöņĀü Ļ┤Ćņ░░ ņŖżņ╝ĆņżäņØä Ļ│äĒÜŹĒĢśĻ│Ā, ņØ┤ļź╝ ĒÖśņ×É Ļ┤Ćļ”¼ņŚÉ Ļ┤ĆņŚ¼ĒĢśļŖö ļŗżļźĖ ņĀäļ¼ĖĻ░Ćļōż(ĒÖśņ×Éļź╝ ļŗ┤ļŗ╣ĒĢśļŖö ņŗ¼ņןļé┤Ļ│╝ ņØśņé¼, ņØ╝ļ░śņØś, ņĢĮņé¼, Ļ░äĒśĖņé¼, ĒĢŁņØæĻ│Ā Ēü┤ļ”¼ļŗē, ĒÖśņ×Éļź╝ ņ¦äļŻīĒĢśļŖö ĒāĆĻ│╝ ņØśļŻīņ¦ä ļō▒)Ļ│╝ļÅä Ļ│Ąņ£ĀĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż. ĒÖśņ×É Ļ┤Ćļ”¼ņŚÉ ņŚ░Ļ┤ĆļÉ£ ļ¬©ļōĀ ņØśļŻīņ¦äņØ┤ ĒÖśņ×ÉņØś ļ│ĄņĢĮ ņł£ņØæļÅäņŚÉ ņ▒ģņ×äņØ┤ ņ׳ļŗż. 4) ņØ╝ļČĆ ĻĄŁĻ░ĆņØś Ļ▓ĮņÜ░ ņĢĮĻĄŁņØś ņĪ░ņĀ£ ņĀĢļ│┤ņØś ļäżĒŖĖņøīĒü¼Ļ░Ć ņל ņØ┤ļŻ©ņ¢┤ņĀĖ ņ׳ņ¢┤ Ļ░£Ļ░£ņØĖņØś ĒÖśņ×ÉņŚÉĻ▓ī ņ▓śļ░®ļÉśļŖö NOACņØś ņłśļź╝ ļ¬©ļæÉ ņČöņĀüĒĢĀ ņłś ņ׳ļŗż. ņØ┤ļ¤░ Ļ▓ĮņÜ░ ņĢĮņé¼Ļ░Ć ļ│ĄņĢĮ ņł£ņØæļÅä ļ¬©ļŗłĒä░ļ¦üņŚÉ ņĀüĻĘ╣ņĀüņ£╝ļĪ£ Ļ░£ņ×ģļÉĀ ņłś ņ׳ņ£╝ļ®░ ņØ┤ļ¤¼ĒĢ£ ņĀĢļ│┤ļŖö ņĀüņĀłĒĢ£ ņ▓śļ░® ļ░Å ņÜ®ļ¤ē ņĪ░ņĀłņØś ļīĆņĪ░ Ļ▓ĆĒåĀņŚÉ ņØ┤ņÜ®ļÉĀ ņłś ņ׳ļŗż. ņØ╝ļČĆ ĻĄŁĻ░ĆņŚÉņä£ļŖö ņĢĮņé¼ņŚÉ ņØśĒĢ£ ņČöņĀü Ļ┤Ćņ░░Ļ│╝ ļ│ĄņĢĮ ņł£ņØæļÅä ļ¬©ļŗłĒä░ļ¦üņØś ņ”ØĻ░ĆĻ░Ć ļ│ĄņĢĮ ņł£ņØæļÅäļź╝ Ē¢źņāüņŗ£ņ╝░ļŗż[92]. 5) ļ│ĄņĢĮ ņł£ņØæļÅäļź╝ Ē¢źņāüņŗ£ĒéżĻĖ░ ņ£äĒĢ£ ņŚ¼ļ¤¼ Ļ░Ćņ¦Ć ĒśĢĒā£ņØś ļ¦ÄņØĆ ĻĖ░ņłĀņĀüņØĖ ļÅäņøĆ ņןņ╣śļōżņØ┤ Ļ░£ļ░£ļÉśĻ│Ā ņĀüņÜ®ļÉśĻ│Ā ņ׳ļŗż. ĒŖ╣ņłśĒĢ£ ņĢĮņĀ£ ĒżņןņÜ®ĻĖ░ Ēś╣ņØĆ ņĢĮņĀ£ ļ│┤Ļ┤Ć ņāüņ×É(ĻĖ░ņĪ┤ ļ░®ņŗØ ļśÉļŖö ļ│ĄņĢĮņØ┤ ĻĖ░ļĪØļÉśļŖö ņĀäņ×É ņןņ╣śņÖĆ ņŚ░Ļ│äļÉ£ ļ░®ņŗØ) ĒśĢĒā£Ļ░Ć ņ׳ņ¢┤ņÖöĻ│Ā, ņĄ£ĻĘ╝ņŚÉļŖö ņŖżļ¦łĒŖĖĒÅ░ ņ¢┤Ēöīļ”¼ņ╝ĆņØ┤ņģśņØä ņØ┤ņÜ®ĒĢśņŚ¼ ĒÖśņ×ÉņŚÉĻ▓ī ļ│ĄņĢĮ ņŗ£Ļ░äņØä ņĢīļĀżņŻ╝ļŖö ĒśĢĒā£ņØś ļÅäņøĆ ņןņ╣śļōżļÅä ņ׳ļŗż[93]. 6) ņŗ¼ĒśłĻ┤Ć ĒÖśņ×ÉņŚÉņä£ ņØ╝ļ░śņĀüņ£╝ļĪ£ 1ņØ╝ 1ĒÜī ņÜ®ļ▓ĢņØ┤ 1ņØ╝ 2ĒÜī ņÜ®ļ▓Ģļ│┤ļŗż ļ│ĄņĢĮ ņł£ņØæļÅäĻ░Ć ļåÆļŗż[94-97]. ļīĆļČĆļČäņØś NOAC ļ│ĄņĢĮ ņł£ņØæļÅäļź╝ ĒÅēĻ░ĆĒĢ£ ņŚ░ĻĄ¼ļōżņŚÉ ņØśĒĢśļ®┤, 1ņØ╝ 1ĒÜī ņÜ®ļ▓ĢņØ┤ ļé©ņØĆ ņĢīņĢĮ ņłś ņĖĪļ®┤ņŚÉņä£ ļŹö ņÜ░ņłśĒĢśņśĆļŗż[51,54-57,78,97-100]. ĒśłņĀä ņāēņĀäņ”Ø ņśłļ░® ĒÜ©Ļ│╝ņÖĆ ņĢłņĀäņä▒ ļ│┤ņןņŚÉ ļīĆĒĢśņŚ¼ ņ¢┤ļ¢ż ņÜ®ļ▓ĢņØ┤ ļŹö ņÜ░ņłśĒĢ£ņ¦ĆļŖö ļČłļČäļ¬ģĒĢśņ¦Ćļ¦ī, ļé«ņØĆ ļ│ĄņĢĮ ņł£ņØæļÅäļŖö ļéśņü£ ņ×äņāüņĀü Ļ▓░Ļ│╝ņÖĆ ņŚ░Ļ┤ĆļÉ£ļŗż[66-69,73-78,101-104]. 1ņØ╝ 1ĒÜī ņÜ®ļ▓ĢņŚÉņä£ ĒĢ£ļ▓ł ļ│ĄņĢĮņØä ļåōņ╣śļŖö Ļ▓āņØ┤ 1ņØ╝ 2ĒÜī ņÜ®ļ▓ĢņŚÉņä£ ļæÉ ļ▓ł ļ│ĄņĢĮņØä ļåōņ╣śļŖö Ļ▓āļ│┤ļŗż ĒĢŁņØæĻ│Ā ņ×æņÜ®ņØś ļ│ĆļÅÖņä▒ņØ┤ ļŹö Ēü┤ ņłś ņ׳ļŗżļŖö ļŹ░ņØ┤Ēä░Ļ░Ć ņ׳ņ¦Ćļ¦ī[105], ņØ┤ļ¤¼ĒĢ£ ļ│ĆļÅÖņä▒ņØ┤ Ļ░¢ļŖö ņ×äņāüņĀü ņØśļ»ĖļŖö ĒÖĢņØĖļÉśņ¦Ć ņĢŖņĢśļŗż[106]. 7) ļé«ņØĆ ļ│ĄņĢĮ ņł£ņØæļÅäĻ░Ć ņØśņŗ¼ļÉĀ Ļ▓ĮņÜ░ ņĀäņ×É ļ¬©ļŗłĒä░ļ¦üņØä ņØ┤ņÜ®ĒĢśņŚ¼ ĒÖśņ×ÉņØś ņĢĮņĀ£ ļ│ĄņÜ® Ēī©Ēä┤ņŚÉ Ļ┤ĆĒĢ£ ņĀĢļ│┤ļź╝ ņ¢╗Ļ│Ā, ĒÖśņ×Éļź╝ ĻĄÉņ£ĪĒĢśļŖöļŹ░ ļÅäņøĆņØä ņ¢╗ņØä ņłś ņ׳ļŗż. ņĀäņ×ÉņĢĮņĀ£ ļ│ĄņÜ® ļ¬©ļŗłĒä░ļ¦üņØĆ ņøÉĻ▓® ļ¬©ļŗłĒä░ļ¦ü ņä£ļ╣äņŖżņÖĆ ņŚ░Ļ│äļÉĀ ņłśļÅä ņ׳Ļ│Ā ĒÖśņ×ÉņŚÉĻ▓ī ņóĆ ļŹö ļ╣ĀļźĖ Ēö╝ļō£ļ░▒ņØä ņĀ£Ļ│ĄĒĢĀ ņłś ņ׳ļŗż[107]. 8) ļ¬©ļŗłĒä░ļ¦ü ĒĢśņ¦Ć ņĢŖļŖö NOACļ│┤ļŗżļŖö INR ļ¬©ļŗłĒä░ļ¦üņØ┤ Ļ░ĆļŖźĒĢ£ ņÖĆĒīīļ”░ņØä ņäĀĒśĖĒĢśļŖö ĒÖśņ×ÉļōżļÅä ņ׳ļŗż. ņØ┤ļ¤░ ĒÖśņ×ÉĻĄ░ņŚÉĻ▓īļÅä NOAC ņé¼ņÜ®ņØ┤ ĒĢŁņØæĻ│Ā ĒÜ©Ļ│╝Ļ░Ć ņĀüņĀłĒĢśĻ▓ī ņ£Āņ¦ĆļÉśļŖö ņÖĆĒīīļ”░ĻĄ░Ļ│╝ ļ╣äĻĄÉĒĢśņŚ¼ļÅä ļæÉĻ░£ļé┤ ņČ£ĒśłņØś ņ£äĒŚśņØä ĒśäņĀĆĒ׳ ņżäņØ┤ļŖö ļō▒ņØś ņĄ£ĻĘ╝ņØś ņ×äņāüņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļź╝ ĻĄÉņ£ĪĒĢśļŖö Ļ▓āņØ┤ ĒĢäņÜöĒĢśļŗż[18,36]. 9) ņĀüņĀłĒĢ£ ĻĄÉņ£ĪĻ│╝ ņČöĻ░ĆņĀüņØĖ ļÅäĻĄ¼ ņé¼ņÜ®ņŚÉļÅä ļ│ĄņĢĮ ņł£ņØæļÅäĻ░Ć ļé«ņØĆ NOAC ĒÖśņ×ÉļōżņØĆ ļŗżņŗ£ ņÖĆĒīīļ”░ņ£╝ļĪ£ ņĀäĒÖśņØä Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢ£ļŗż. ĒĢśņ¦Ćļ¦ī ļé«ņØĆ ļ│ĄņĢĮ ņł£ņØæļÅäļź╝ ļ│┤ņØ┤ļŖö ĒÖśņ×ÉļōżņØĆ ņÖĆĒīīļ”░ ņé¼ņÜ®ņŚÉļÅä ņŚŁņŗ£ Ēü░ INR ļ│ĆļÅÖĒÅŁņØä ļ│┤ņØ┤ļ®░ ņØ┤ļŖö ļéśņü£ ņ×äņāü Ļ▓ĮĻ│╝ņÖĆ ņŚ░Ļ┤ĆļÉ£ļŗż.
ļŗżļźĖ ĒĢŁņØæĻ│ĀņĀ£ļĪ£ ĻĄÉņ▓┤ĒĢśļŖö ļ░®ļ▓Ģ
ļŗżļźĖ ĒĢŁņØæĻ│ĀņĀ£ļĪ£ ĻĄÉņ▓┤ĒĢĀ ļĢīļŖö ļ░śļō£ņŗ£ ĒĢŁņØæĻ│ĀņĀ£ņØś ĒÜ©Ļ│╝ļź╝ ņ¦ĆņåŹņŗ£Ēéżļ®┤ņä£ ņČ£Ēśł ļČĆņ×æņÜ®ņØä ņżäņŚ¼ņĢ╝ ĒĢ£ļŗż. ņØ┤ļź╝ ņ£äĒĢśņŚ¼ Ļ░£ļ│ä ņĢĮņĀ£ņØś ņĢĮņŚŁļÅÖĒĢÖņØä Ļ░£Ļ░£ņØĖņØś ĒÖśņ×ÉņŚÉĻ▓ī ņĀüņĀłĒĢśĻ▓ī ņĀüņÜ®ĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż.
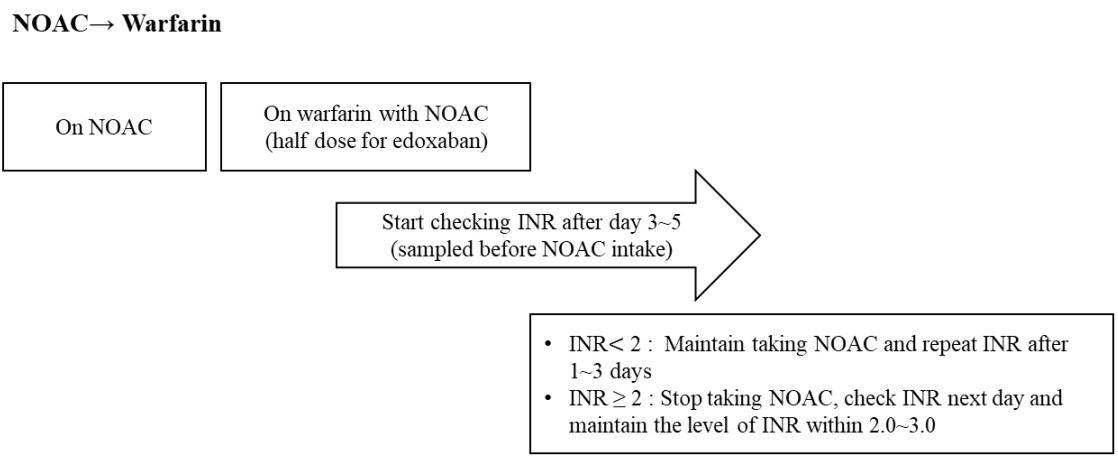
ņÖĆĒīīļ”░ņŚÉņä£ NOACļĪ£ņØś ņĀäĒÖś
INR ņłśņ╣śĻ░Ć ņ╣śļŻī ļ¬®Ēæ£ņ╣śņØĖ ĒÖśņ×ÉņŚÉņä£ NOACļĪ£ ņĢĮņĀ£ļź╝ ņĀäĒÖśĒĢśļŖö Ļ▓ĮņÜ░, NOACņØś Ēł¼ņĢĮ ņŗ£ņĀÉņØĆ ņÖĆĒīīļ”░ņØä ņżæļŗ©ĒĢ£ Ēøä INR ņłśņ╣śņŚÉ ļö░ļźĖ ļŗżņØīņØś ĻČīĻ│ĀņĢłņØä ļö░ļźĖļŗż(Fig. 4). ņÖĆĒīīļ”░ņØś ļ░śĻ░ÉĻĖ░ļŖö 36-48ņŗ£Ļ░äņØ┤ļ»ĆļĪ£, ņØ┤ļ¤¼ĒĢ£ ņĢĮņŚŁļÅÖĒĢÖņĀü ņ¦ĆņŗØņØä ĻĘ╝Ļ▒░ļĪ£ ĒĢśņŚ¼ ņĢĮņĀ£ ņżæļŗ© Ēøä INRņØä ļŗżņŗ£ ĒÖĢņØĖĒĢĀ ņŗ£ņĀÉņØä Ļ▓░ņĀĢĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż.
NOACņŚÉņä£ ņÖĆĒīīļ”░ņ£╝ļĪ£ņØś ņĀäĒÖś
ņÖĆĒīīļ”░ņØĆ ņ×æņÜ® ņŗ£Ļ░äņØ┤ ļŖ”ĻĖ░ ļĢīļ¼ĖņŚÉ, ņ╣śļŻī ļ¬®Ēæ£ņØś INRņŚÉ ļÅäļŗ¼ĒĢśĻĖ░ ņ£äĒĢ┤ņä£ļŖö 5-10ņØ╝ ņĀĢļÅäņØś ĻĖ░Ļ░äņØ┤ ņåīņÜöļÉ£ļŗż. ļö░ļØ╝ņä£ NOACņŚÉņä£ ņÖĆĒīīļ”░ņ£╝ļĪ£ ļ│ĆĻ▓ĮĒĢśĻĖ░ ņ£äĒĢ┤ņä£ļŖö ņāüļŗ╣ĒĢ£ ņŗ£Ļ░äņØ┤ ĒĢäņÜöĒĢśļ®░, NOAC ņżæļŗ© ņŗ£ņĀÉņØä ņĀüņĀłĒĢśĻ▓ī Ļ▓░ņĀĢĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż. ņÖĆĒīīļ”░ņŚÉņä£ NOACļĪ£ņØś ņĢĮņĀ£ ņĀäĒÖśņØä ņ£äĒĢ£ ĒØÉļ”äļÅäļź╝ ĻĘĖļ”╝ 5ņŚÉ ņĀ£ņŗ£ĒĢśņśĆļŗż. ņØ╝ļ░śņĀüņ£╝ļĪ£ ļČĆĒĢś ņÜ®ļ¤ē(loading dose)ņØĆ ņÖĆĒīīļ”░ņØä ņé¼ņÜ®ĒĢĀ Ļ▓ĮņÜ░ņŚÉļŖö ĒĢäņÜöĻ░Ć ņŚåļŗż.
NOACļŖö INRņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣Ā ņłś ņ׳ņ£╝ļ»ĆļĪ£, NOAC ļ│ĄņÜ® ņ¦üņĀäņŚÉ INRņØä ņĖĪņĀĢĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗżļŖö ņĀÉņØä ņ£ĀļģÉĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż. ļśÉĒĢ£ NOACņŚÉņä£ ņÖĆĒīīļ”░ņ£╝ļĪ£ ļ│ĆĻ▓ĮņØä ņŗ£ņ×æĒĢ£ņ¦Ć 1Ļ░£ņøö ņØ┤ļé┤ņŚÉļŖö ņ▓ĀņĀĆĒĢśĻ▓ī INRņØä ņĖĪņĀĢĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż. ENGAGE-AF ņŚ░ĻĄ¼ņŚÉņä£ NOACņŚÉņä£ ņÖĆĒīīļ”░ņ£╝ļĪ£ ņĀäĒÖśņØ┤ ņÖäļŻīļÉśļŖö ļŹ░ņŚÉļŖö ļīĆļץ 14ņØ╝ Ļ░Ćļ¤ēņØś ĻĖ░Ļ░äņØ┤ ņÜöĻĄ¼ļÉśņŚłļŗż[108]. ņĢĮņĀ£ ņĀäĒÖśņØä ņ£äĒĢ£ ĒØÉļ”äļÅäļź╝ ņżĆņłśĒĢśņśĆņØä ļĢīļŖö ļćīĻ▓ĮņāēņØ┤ļéś ļćīņČ£ĒśłĻ│╝ Ļ░ÖņØĆ ļČĆņ×æņÜ®ņØ┤ ņĀüņŚłļŹś ļ░śļ®┤[108], ņżĆņłśĒĢśņ¦Ć ņĢŖņĢśņØä Ļ▓ĮņÜ░ņŚÉļŖö ļČĆņ×æņÜ®ņØ┤ ĒÖĢņŚ░ĒĢśĻ▓ī ņ”ØĻ░ĆĒĢśņśĆļŗż[109,110].
NOACņŚÉņä£ ļ╣äĻ▓ĮĻĄ¼ņÜ® ĒĢŁņØæĻ│ĀņĀ£ļĪ£ņØś ņĀäĒÖś
NOAC ņżæļŗ© Ēøä ļÅÖņØ╝ ņĢĮņĀ£ļź╝ ļŗżņØīņŚÉ ļ│ĄņÜ®ĒĢĀ ņŗ£ņĀÉņŚÉ ļ╣äĻ▓ĮĻĄ¼ ĒĢŁņØæĻ│ĀņĀ£ņØĖ ĒŚżĒīīļ”░ņØä Ēł¼ņŚ¼ĒĢ£ļŗż.
ļ╣äĻ▓ĮĻĄ¼ ĒĢŁņØæĻ│ĀņĀ£ņŚÉņä£ NOACļĪ£ņØś ņĀäĒÖś
ļ╣äļČäĒÜŹ ĒŚżĒīīļ”░ ņżæļŗ© Ēøä 2-4ņŗ£Ļ░äņØ┤ Ļ▓ĮĻ│╝ĒĢ£ ļÆż NOACļź╝ Ēł¼ņŚ¼ĒĢ£ļŗż. ņĀĆ ļČäņ×Éļ¤ē ĒŚżĒīīļ”░ņØĆ ņżæļŗ© Ēøä ļŗżņØī Ēł¼ņŚ¼ ņŗ£ņĀÉņŚÉ NOACļź╝ Ēł¼ņŚ¼ĒĢ£ļŗż.
NOACņØś ņĢĮļÅÖĒĢÖĻ│╝ ņĢĮņĀ£Ļ░ä ņāüĒśĖņ×æņÜ®
ņÖĆĒīīļ”░ņØä ņé¼ņÜ®ĒĢśļŖö Ļ▓ĮņÜ░ļŖö ņŚ¼ļ¤¼ ņØīņŗØĻ│╝ ņĢĮņĀ£ Ļ░ä ņāüĒśĖņ×æņÜ®ņØä ņŗĀņżæĒ׳ Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢ£ļŗż. NOACļŖö ņØ┤ļ¤░ ņāüĒśĖņ×æņÜ®ņØ┤ ņāüļīĆņĀüņ£╝ļĪ£ ņĀüņ¦Ćļ¦ī, ļ░śļō£ņŗ£ ļÅÖļ░ś ņĢĮņĀ£ ļ░Å ĻĖ░ņĀĆ ņ¦łĒÖśņŚÉ ļīĆĒĢśņŚ¼ Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢ£ļŗż. Ļ░üĻ░ü ĒÖśņ×ÉļōżņØś ĒŖ╣ņä▒ņŚÉ ļ¦×ļŖö ņ▓śļ░®ņØä ĒĢ┤ņĢ╝ ĒĢśĻ│Ā, ĒŖ╣Ē׳ ĒÖśņ×ÉĻ░Ć Ļ░Ćņ¦ä ņŚ¼ļ¤¼ ņØĖņ×Éļōż Ļ░äņØś ņāüĒśĖņ×æņÜ®ņŚÉ ļīĆĒĢ┤ņä£ļÅä Ļ│ĀļĀżĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż. ņāüĒśĖņ×æņÜ®ņŚÉ ļīĆĒĢ£ ņĀĢļ│┤Ļ░Ć ņĀÉņ░© ļ¦ÄņĢä ņ¦ÉņŚÉ ļö░ļØ╝ Ē¢źĒøäņŚÉļŖö ņāłļĪ£ņÜ┤ ņĀĢļ│┤ļōżņØ┤ Ēśäņ×¼ņØś ĻČīĻ│ĀņĢłņØä ļ│ĆĻ▓Įņŗ£Ēé¼ ņłśļÅä ņ׳ļŗż.
ļīĆļČĆļČä NOACņÖĆņØś ņāüĒśĖņ×æņÜ®ņŚÉļŖö ņ£äņןĻ┤ĆņØä ĒåĄĒĢśņŚ¼ ĒØĪņłśļÉ£ ļÆż P-glycoprotein (P-gp)ņØä ĒåĄĒĢ£ ņ×¼ļČäļ╣ä Ļ│╝ņĀĢņØ┤ Ļ┤ĆņŚ¼ĒĢ£ļŗż. ņØ┤ Ļ│╝ņĀĢņŚÉņä£ ņĢĮņĀ£ļōż Ļ░äņØś Ļ▓Įņ¤üņĀüņØĖ ņ¢ĄņĀ£Ļ░Ć ņĢĮļ¼╝ņØś Ēśłņżæ ļåŹļÅä ņ”ØĻ░Ćļź╝ ņØ╝ņ£╝Ēé©ļŗż. P-gpļŖö ņŗĀņן ļ░░ņäżĻ│╝ļÅä ņŚ░Ļ┤ĆļÉ£ļŗż[111]. ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉņŚÉņä£ ņé¼ņÜ®ĒĢśļŖö ņĢĮņĀ£ļōż ņżæ ņāüļŗ╣ņłśĻ░Ć P-gp ņ¢ĄņĀ£ņĀ£ņØ┤ļŗż(ļ▓ĀļØ╝Ēīīļ░Ć, ļō£ļĪ£ļäżļŗżļĪĀ, ņĢäļ»ĖņśżļŗżļĪĀ, ĒĆ┤ļŗłļöś ļō▒). ļ”¼ļ░öļĪØņé¼ļ░śĻ│╝ ņĢäĒöĮņé¼ļ░śņØś ņĢĮļ¼╝ ļīĆņé¼ļŖö CYP3A4 typeņØś Cytochrome P450ņØä ņØ┤ņÜ®ĒĢśņŚ¼ ņØ┤ļŻ©ņ¢┤ņ¦äļŗż[112]. Ļ░ĢļĀźĒĢ£ CYP3A4 ņ¢ĄņĀ£ļéś ņ£ĀļÅäĻ░Ć ņØ┤ļōż ņĢĮņĀ£ņØś Ēśłņżæ ļåŹļÅäņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣Ā ņłś ņ׳ļŗż. ņĢäĒöĮņé¼ļ░śņØś ļ╣äļīĆņé¼ņĀü ņĀ£Ļ▒░ļŖö ļŗżņ¢æĒĢśņŚ¼ ņ×Āņ×¼ņĀüņØĖ ņĢĮļ¼╝ Ļ░ä ņāüĒśĖņ×æņÜ®ņØ┤ ņāüļīĆņĀüņ£╝ļĪ£ ņĀüļŗż[113]. ņØ╝ļ░śņĀüņ£╝ļĪ£, Ļ░ĢļĀźĒĢ£ P-gp Ēś╣ņØĆ CYP3A4 ņ¢ĄņĀ£ ņĢĮļ¼╝ņØä NOACņÖĆ ļ│æņÜ®ņØĆ ĻČīĻ│ĀļÉśņ¦Ć ņĢŖļŖöļŗż. ļ░śļīĆļĪ£ Ļ░ĢļĀźĒĢ£ P-gp Ēś╣ņØĆ CYP3A4 ņ£ĀļÅä ņĢĮņĀ£ļź╝ ņé¼ņÜ®ĒĢśļŖö Ļ▓ĮņÜ░, NOAC ņĢĮņĀ£ņØś Ēśłņżæ ļåŹļÅäļź╝ ĒśäņĀĆĒ׳ ņĀĆĒĢśņŗ£Ēé¼ ņłś ņ׳ņ¢┤ ņØ┤ļ¤░ ņĢĮņĀ£ņÖĆņØś ļ│æņÜ®ņØĆ ĻĖłĒĢśĻ▒░ļéś ņŻ╝ņØś Ļ╣ŖĻ▓ī ņé¼ņÜ®ĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż.
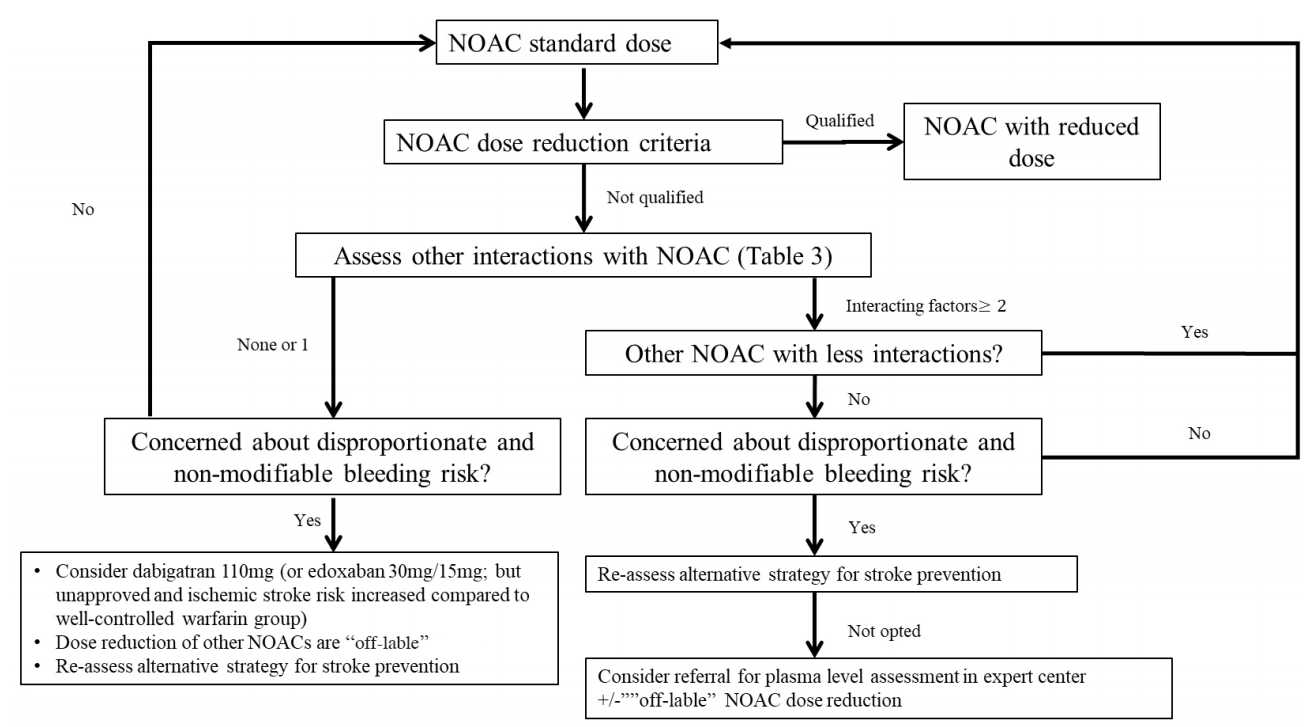
ļŗżņ¢æĒĢ£ NOACņØś ņÜ®ļ¤ē ņĪ░ņĀłņŚÉ ļīĆĒĢ£ ņĢīĻ│Āļ”¼ņ”śņØ┤ ļīĆĻĘ£ļ¬© 3ņāü ņŚ░ĻĄ¼ņŚÉņä£ ĒÅēĻ░ĆļÉśņŚłĻ│Ā, ĻĘĖ ĒÜ©Ļ│╝ņÖĆ ņĢłņĀäņä▒ņØ┤ ņ”Øļ¬ģļÉśņŚłļŗż. ENGAGE-AF ņŚ░ĻĄ¼ņŚÉņä£ļ¦ī ņÜ®ļ¤ē Ļ░Éņåī ĻĖ░ņżĆņŚÉ ĒżĒĢ©ļÉ£ ņĢĮņĀ£ļź╝ ĒżĒĢ©ĒĢśņŚ¼ ļČäņäØĒĢśņśĆļŗż. ĻĖ░ņĪ┤ņŚÉ ļ░£Ēæ£ļÉ£ ņÜ®ļ¤ē Ļ░Éņåī ĻĖ░ņżĆņŚÉ ĻĘ╝Ļ▒░ĒĢśņŚ¼ ņÜ®ļ¤ēņØä Ļ░ÉņåīĒĢśĻ│Ā, ļÉśļÅäļĪØ ņĀĢĒĢ┤ņ¦ä ĻČīĻ│Ā ņÜ®ļ¤ēņŚÉ ļ¦×Ļ▓ī ņé¼ņÜ®ĒĢśļŖö Ļ▓āņØ┤ ĻČīņןļÉ£ļŗż. ĻĘĖļ¤¼ļéś ņČ£Ēśł ņä▒Ē¢źņØ┤ ļåÆĻ▒░ļéś ņŚ¼ļ¤¼ ņØĖņ×ÉļĪ£ ņØĖĒĢśņŚ¼ Ēśłņżæ ņĢĮļ¼╝ ļåŹļÅäĻ░Ć ļåÆņØä Ļ▓āņ£╝ļĪ£ ņśłņāüļÉśļŖö ĒÖśņ×ÉļōżņŚÉņä£ļŖö NOAC ņÜ®ļ¤ē Ļ░Éļ¤ēņØ┤ ņśżĒ׳ļĀż ĒĢ®ļ”¼ņĀüņØ╝ ņłś ņ׳ļŗż[17,114-117]. ņĀĆ ņÜ®ļ¤ēņØś NOACņŚÉ ļīĆĒĢ£ ņĀäĒ¢źņĀü ņŚ░ĻĄ¼ļŖö ļŗżļ╣äĻ░ĆĒŖĖļ×Ć 110 mg ĒĢśļŻ© 2ĒÜīņÖĆ ņŚÉļÅģņé¼ļ░ś 30/15 mg ĒĢśļŻ© 1ĒÜī ņé¼ņÜ®ņŚÉ ļīĆĒĢ┤ņä£ļ¦ī ņ¦äĒ¢ēļÉśņŚłļŗż. ļŗżļ╣äĻ░ĆĒŖĖļ×Ć 110 mg ĒĢśļŻ© 2ĒÜī ņé¼ņÜ®ņØĆ ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ņÖĆ ļ╣äĻĄÉĒĢśņŚ¼ ļćīņĪĖņżæ ļ░£ņāØļźĀņØĆ ļ╣äņŖĘĒĢśņśĆĻ│Ā ņŻ╝ņÜö ņČ£Ēśł ņé¼Ļ▒┤ņØĆ Ļ░ÉņåīĒĢśņśĆļŗż[23]. ĒĢśņ¦Ćļ¦ī ņØ┤ļŖö ļČłĒŖ╣ņĀĢĒĢ£ ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉļōżņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ ņŚ░ĻĄ¼ņØ┤ĻĖ░ ļĢīļ¼ĖņŚÉ, ņĢĮļ¼╝ņØś Ēśłņżæ ļåŹļÅäĻ░Ć ņ”ØĻ░ĆļÉ£ ĒÖśņ×ÉņŚÉņä£ņØś ņŻ╝ņÜö ņČ£Ēśł ņé¼Ļ▒┤ņØś Ļ░Éņåī ĒÜ©Ļ│╝ļŖö ņŚåņØä ņłśļÅä ņ׳ļŗż[115,118]. ņŚÉļÅģņé¼ļ░ś 30/15 mg ĒĢśļŻ© 1ĒÜī ņé¼ņÜ®ņØĆ ļ╣äĻĄÉņĀü ņל ņĪ░ņĀłļÉśļŖö ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ ņé¼ņÜ®ĻĄ░ņŚÉ ļ╣äĒĢśņŚ¼ ĒŚłĒśłņä▒ ļćīņĪĖņżæņØ┤ 41% ņ”ØĻ░ĆļÉśņŚłĻĖ░ ļĢīļ¼ĖņŚÉ, ņŚÉļÅģņé¼ļ░ś ņĀĆņÜ®ļ¤ē ņé¼ņÜ®ņØĆ ņŖ╣ņØĖļ░øņ¦Ć ļ¬╗ĒĢśņśĆļŗż[24,116]. ĒĢśņ¦Ćļ¦ī ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ ņé¼ņÜ®ĻĄ░Ļ│╝ ļīĆļ╣äĒĢśņŚ¼ ņŻ╝ņÜö ņČ£Ēśł, ņŗ¼ĒśłĻ┤ĆĻ│ä ĻĘĖļ”¼Ļ│Ā ļ¬©ļōĀ ņøÉņØĖņØś ņé¼ļ¦ØļźĀņØĆ ņŚÉļÅģņé¼ļ░ś ņé¼ņÜ®ĻĄ░ņŚÉņä£ Ļ░ÉņåīļÉśņŚłļŗż. ļö░ļØ╝ņä£, ņØ┤ļ¤░ ņĀĆņÜ®ļ¤ē NOAC ņŚ░ĻĄ¼ļŖö ļćīņĪĖņżæ ņśłļ░® ĒÜ©Ļ│╝ņŚÉ ļīĆĒĢ┤ņä£ļ¦ī ĒĢ┤ņäØņØ┤ Ļ░ĆļŖźĒĢśļŗż[23,34]. ļ░śļ®┤, ROCKET-AFļéś ARISTOTLE ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņĀĆņÜ®ļ¤ēĻĄ░ņØ┤ ĒżĒĢ©ļÉśņ¢┤ ņ׳ņ¦Ć ņĢŖņĢä Ļ░Éļ¤ēļÉ£ ņÜ®ļ¤ēņŚÉ ļīĆĒĢ┤ņä£ļŖö ņĀĢļ│┤Ļ░Ć ņĀ£ĒĢ£ņĀüņØ┤ļŗż[119]. ļīĆļŗżņłśņØś ĒÖśņ×ÉņŚÉņä£ ŌĆ£off-lableŌĆØļĪ£ ņĀĆņÜ®ļ¤ē ņ▓śļ░®ņØĆ ņØ┤ļ¤░ ņØ┤ņ£ĀņŚÉņä£ ņ¦Ćņ¢æļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż. ņŗżņĀ£ļĪ£, ņČ£Ēśł Ļ▓ĮĒ¢źņØä ļåÆņØ┤ļŖö ņØĖņ×ÉļōżņØ┤ ļćīņĪĖņżæņØś ņ£äĒŚśņØĖņ×ÉņØĖ Ļ▓ĮņÜ░Ļ░Ć ļ¦ÄņĢä(Ļ│ĀļĀ╣, ļģĖņćĀĒĢ© ļō▒) ļČĆņĀüņĀłĒĢśĻ▓ī Ļ░Éļ¤ēļÉ£ ņÜ®ļ¤ēņ£╝ļĪ£ļŖö ļćīņĪĖņżæņØś ņśłļ░® ĒÜ©Ļ│╝Ļ░Ć ņČ®ļČäņ╣ś ļ¬╗ĒĢĀ ņłś ņ׳ļŗż[120]. ĒĢśņ¦Ćļ¦ī, ĒŖ╣ņĀĢĒĢ£ ņĢĮļ¼╝ Ļ░ä ņāüĒśĖņ×æņÜ® Ēś╣ņØĆ ĒŖ╣ņłśĒĢ£ ĻĖ░ņĀĆ ņ¦łĒÖśņØ┤ ņ׳ļŖö ĒÖśņ×É(ņןĻĖ░ ņØ┤ņŗØ ĒÖśņ×É, HIV ņĢĮļ¼╝ ļ│ĄņÜ®ņżæņØĖ ĒÖśņ×É)ņŚÉņä£ļŖö ļō£ļ¼╝Ļ▓ī NOACņØś Ļ░Éļ¤ē Ēś╣ņØĆ ņżæļŗ© ļō▒ņØ┤ ĒĢäņÜöĒĢĀ ņłś ņ׳ļŗż(Fig. 6). ņØ┤ļ¤░ Ļ▓ĮņÜ░ņŚÉļŖö ņØ┤ļ¤¼ĒĢ£ ĒŖ╣ņłśĒĢ£ ņĢĮņĀ£ļéś NOACņØś Ļ▓ĮĒŚśņØ┤ ĒÆŹļČĆĒĢ£ ņØśļŻī ĻĖ░Ļ┤ĆņŚÉņä£ Ļ┤Ćļ”¼ļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż. ņÜöņĢĮĒĢśņ×Éļ®┤, NOACņØś Ēśłņżæ ļåŹļÅäņŚÉ ņśüĒ¢źņØä ņżä ņłś ņ׳ļŖö ņĢĮļ¼╝ Ļ░äņØś ņāüĒśĖņ×æņÜ®ņØ┤ļéś ĒŖ╣Ē׳ ĒŖ╣ņłśĒĢ£ ņ×äņāü ņāüĒÖ®Ļ│╝ ļÅÖļ░śļÉ£ Ļ▓ĮņÜ░, ĒÖśņ×ÉņŚÉļ¦×ņČ░ņä£ NOACļź╝ ņĀüņĀłĒ׳ ņ▓śļ░®ĒĢśļŖö Ļ▓āņØ┤ ņżæņÜöĒĢśļŗż. ļŗżņØīņØś Ēæ£ 3ņØĆ NOACņØś Ēśłņżæ ļåŹļÅäņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣Ā ņłś ņ׳ļŖö ņŚ¼ļ¤¼ ņĢĮņĀ£ļōżņŚÉ ļīĆĒĢśņŚ¼ ņĀĢļ”¼ĒĢśņśĆļŗż. ņØ┤ļ¤░ ņØĖņ×ÉļōżĻ│╝ ļīĆĻĘ£ļ¬© ļ¼┤ņ×æņ£ä ņŚ░ĻĄ¼ņØś Ļ▓░Ļ│╝ļōżņØä ļ░öĒāĢņ£╝ļĪ£ NOACņØś ņäĀĒāØ ļ░Å ĻĘĖ ņÜ®ļ¤ēņØä Ļ▓░ņĀĢĒĢĀ ņłś ņ׳ļŗż. ĻĘĖļ¤╝ņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā ņŗżņĀ£ļĪ£ ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉņŚÉņä£ ņé¼ņÜ®ļÉśļŖö ņāüĒśĖņ×æņÜ®ņØ┤ Ļ░ĆļŖźĒĢ£ ņāüļŗ╣ņłśņØś ņĢĮņĀ£ļōżņŚÉ ļīĆĒĢ┤ņä£ļŖö ņĀĢļ│┤Ļ░Ć ļ»Ėļ»ĖĒĢśļŗżļŖö ņĀÉņØä ņŚ╝ļæÉĒĢ┤ņĢ╝ ĒĢ£ļŗż.
ņØīņŗØ ņäŁņĘ©, ņĀ£ņé░ņĀ£, ļ╣äņ£äĻ┤ĆņØä ĒåĄĒĢ£ ņĢĮļ¼╝ Ēł¼ņŚ¼
ļ”¼ļ░öļĪØņé¼ļ░ś 15 mg/20 mgņØĆ ļŗżļźĖ NOACņÖĆ ļŗ¼ļ”¼ ņØīņŗØļ¼╝Ļ│╝ ĒĢ©Ļ╗ś ņäŁņĘ©ĒĢśļÅäļĪØ ĒĢ£ļŗż. ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØś Ļ▓ĮņÜ░, PPIļéś H2 blockerņÖĆ ĒĢ©Ļ╗ś ļ│ĄņÜ®ĒĢśļ®┤ ņāØņ▓┤ ņØ┤ņÜ®ļźĀņØ┤ ņĢĮĻ░ä Ļ░ÉņåīļÉśņ¦Ćļ¦ī, ņ×äņāüņĀü ĒÜ©Ļ│╝ņŚÉļŖö ņ░©ņØ┤Ļ░Ć ņŚåļŗż[121,122]. ļŗżļźĖ NOACņŚÉņä£ļÅä ņĀ£ņé░ņĀ£ņÖĆņØś ņāüĒśĖņ×æņÜ®ņØĆ ņŚåļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[123-125]. Fish oilĻ│╝ņØś ņĢĮļÅÖĒĢÖņĀü ņ×ÉļŻīļŖö ņŚåņ£╝ļéś ņāüĒśĖņ×æņÜ®ņØĆ ņŚåņØä Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż. ļ╣äņ£äĻ┤ĆņØä ĒåĄĒĢ£ ļČäļ¦É ĒśĢĒā£ Ēł¼ņĢĮņØĆ ņĢäĒöĮņé¼ļ░ś, ļ”¼ļ░öļĪØņé¼ļ░ś, ņŚÉļÅģņé¼ļ░śņŚÉņä£ ņāØņ▓┤ ņØ┤ņÜ®ļźĀņŚÉ ņ░©ņØ┤Ļ░Ć ņŚåļŗż[126-128]. ĒĢśņ¦Ćļ¦ī ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØĆ ņ║ĪņŖÉņØä ņĀ£Ļ▒░ĒĢśĻ│Ā Ļ░ĆļŻ©ļź╝ Ēł¼ņŚ¼ĒĢśļŖö Ļ▓āņØĆ ņāØņ▓┤ ņØ┤ņÜ®ļźĀņØä ņ”ØĻ░Ćņŗ£Ēé¼ ņłś ņ׳ļŗż.
ĒĢŁļČĆņĀĢļ¦źņĀ£(rate control/rhythm control agents)
Ļ░ĆļŖźĒĢ£ ņāüĒśĖņ×æņÜ®ņØĆ Ēæ£ 3ņŚÉ ļ¬ģņŗ£ļÉśņ¢┤ ņ׳ļŗż. ļ▓ĀļØ╝Ēīīļ░ĆņŚÉ ņØśĒĢ£ ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØś P-gp ņ¢ĄņĀ£ ĒÜ©Ļ│╝ļŖö ļ▓ĀļØ╝Ēīīļ░ĆņØś ņä▒ņāüņŚÉ ļö░ļØ╝ ļŗżņ¢æĒĢśļŗż. ņ”ēĒÜ©ĒśĢņØś Ļ▓ĮņÜ░, ļŗżļ╣äĻ░ĆĒŖĖļ×Ćļ│┤ļŗż ĒĢ£ ņŗ£Ļ░ä ņĀäņŚÉ ļ│ĄņÜ®ĒĢśļ®┤ ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØś Ēśłņżæ ļåŹļÅäļź╝ 180%ļĪ£ ņ”ØĻ░Ćņŗ£Ēé¼ ņłś ņ׳ļŗż. ņØ┤ļ¤░ Ļ▓ĮņÜ░ ņĢĮ Ēł¼ņĢĮ Ļ░äĻ▓®ņØä ļæÉ ņŗ£Ļ░ä ņØ┤ņāüņ£╝ļĪ£ ĒĢśļ®┤ ņāüĒśĖņ×æņÜ®ņØĆ ņŚåņ¢┤ņ¦äļŗż. ņä£ļ░®ĒśĢ ņĀ£ņĀ£ņØś Ļ▓ĮņÜ░, ļŗżļ╣äĻ░ĆĒŖĖļ×Ć ļåŹļÅäņØś 60%ļź╝ ņ”ØĻ░Ćņŗ£Ēé¼ ņłś ņ׳ļŗż.
RE-LY ņŚ░ĻĄ¼ņŚÉņä£ ļ▓ĀļØ╝Ēīīļ░ĆņØä ļ│ĄņÜ®ĒĢśļŖö Ļ▓ĮņÜ░ ļŗżļ╣äĻ░ĆĒŖĖļ×Ć ļåŹļÅäĻ░Ć ĒÅēĻĘĀ 23% ņ”ØĻ░ĆĒĢ£ļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆĻ│Ā[129], ņØ┤ņŚÉ ļö░ļØ╝ ļ▓ĀļØ╝Ēīīļ░Ć ļ│ĄņÜ®ņØ┤ ĒĢäņÜöĒĢ£ ĒÖśņ×ÉļŖö ņĀĆņÜ®ļ¤ē ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØä ņé¼ņÜ®ĒĢśļÅäļĪØ ĻČīĒĢ£ļŗż. ņŚÉļÅģņé¼ļ░śļÅä ņ┤łĻĖ░ņŚÉļŖö ņāüĒśĖņ×æņÜ®ņØ┤ ņ׳ļŖö Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉśņŚłņ£╝ļéś[130], 3ņāü ņŚ░ĻĄ¼ ļČäņäØ ĒøäņŚÉļŖö ņØ┤ļ¤░ ņāüĒśĖņ×æņÜ®ņØ┤ ņ×äņāüņĀüņ£╝ļĪ£ ņØśļ»ĖĻ░Ć ņŚåņØīņØ┤ ĒÖĢņØĖļÉśņ¢┤, ņØ┤ņŚÉ ļö░ļźĖ ņÜ®ļ¤ē Ļ░ÉņåīļŖö ĻČīņןļÉśņ¦Ć ņĢŖļŖöļŗż. ĻĘĖļ¤¼ļéś ļŗżļźĖ ņÜöņØĖļōżĻ│╝ņØś ņāüĻ┤Ć Ļ┤ĆĻ│äĻ░Ć ņ׳ļŖöņ¦Ć ņŻ╝ņØśļź╝ ĒĢ┤ņĢ╝ ĒĢ£ļŗż. ņĢäĒöĮņé¼ļ░śņØ┤ļéś ļ”¼ļ░öļĪØņé¼ļ░śņŚÉ ļīĆĒĢśņŚ¼ ļ▓ĀļØ╝Ēīīļ░ĆņØś ņĢĮļÅÖĒĢÖņĀüņØĖ ņāüĒśĖņ×æņÜ®ņØĆ ņĢīļĀżņ¦ä ļ░öĻ░Ć ņŚåļŗż.
ļö£Ēŗ░ņĢäņĀ¼ņØĆ P-gp ņ¢ĄņĀ£ ĒÜ©Ļ│╝Ļ░Ć ļé«ņĢä ņāüĒśĖņ×æņÜ®ņØ┤ ņĀüļŗżĻ│Ā ņĢīļĀżņĪīņØīņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā[129], ņĢäĒöĮņé¼ļ░śņØś Ēśłņżæ ļåŹļÅäļź╝ 40% ņ”ØĻ░Ćņŗ£Ēé©ļŗż[131]. ņĀĢņāü ņŗĀĻĖ░ļŖźņØä Ļ░Ćņ¦ä ĒÖśņ×ÉņŚÉņä£ ņĢäļ»ĖņśżļŗżļĪĀņØĆ ņŚÉļÅģņé¼ļ░śņØś AUCļź╝ 40% ņ”ØĻ░Ćņŗ£Ēé©ļŗż[132]. 3ņāü ņŚ░ĻĄ¼ņŚÉņä£ ņĀĆņÜ®ļ¤ē ņŚÉļÅģņé¼ļ░śĻ│╝ ņĢäļ»ĖņśżļŗżļĪĀ Ļ░äņŚÉļŖö ņāüļŗ╣ĒĢ£ ņāüĒśĖņ×æņÜ®ņØ┤ ņ׳ņ¢┤ Ēśłņżæ ļåŹļÅä ļ│ĆĒÖöņŚÉļÅä ņśüĒ¢źņØ┤ ņ׳ņØä ņłś ņ׳ņØä Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż[133]. ĻĘĖļ¤╝ņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā, ĒĢ©Ļ╗ś ņ▓śļ░®ĒĢśļŖö Ļ▓ĮņÜ░ņŚÉļÅä ņÜ®ļ¤ēņØś Ļ░ÉņåīļŖö ĻČīņןļÉśņ¦Ć ņĢŖļŖöļŗż.
ļō£ļĪ£ļäżļŗżļĪĀņØĆ ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØś Ēśłņżæ ļåŹļÅäņŚÉ Ēü░ ņśüĒ¢źņØä ļ»Ėņ╣śļ»ĆļĪ£, ĒĢ©Ļ╗ś ņé¼ņÜ®ĒĢśļŖö Ļ▓āņØĆ ĻĖłĻĖ░ņØ┤ļŗż. ņŚÉļÅģņé¼ļ░śņŚÉ ļīĆĒĢ┤ņä£ļÅä ņżæļō▒ļÅäņØś ņāüĒśĖņ×æņÜ®ņØ┤ ņ׳ņ¢┤ ļō£ļĪ£ļäżļŗżļĪĀņØä ņé¼ņÜ®ĒĢśļŖö Ļ▓ĮņÜ░ ENGAGE-AFņŚÉņä£ļÅä ņŚÉļÅģņé¼ļ░ś ņÜ®ļ¤ēņØä ņżäņØ┤ļŖö ĻĖ░ņżĆņØ┤ ļÉ£ļŗż[24]. ļ”¼ļ░öļĪØņé¼ļ░śĻ│╝ ņĢäĒöĮņé¼ļ░śņŚÉ ļīĆĒĢ┤ņä£ļŖö ņĢĮļÅÖĒĢÖņĀüņ£╝ļĪ£ ņĢīļĀżņ¦ä ņāüĒśĖņ×æņÜ®ņØ┤ ņŚåņ£╝ļéś, P-gpņÖĆ CYP3A4 ņāüĒśĖņ×æņÜ®ņØä ĻĘ╝Ļ▒░ļĪ£ ņŻ╝ņØśļź╝ ņÜöĒĢ£ļŗż[134]. ĒØźļ»ĖļĪŁĻ▓īļÅä ņĄ£ĻĘ╝ ņŚ░ĻĄ¼ņŚÉņä£ NOAC ļ│ĄņÜ® ĒÖśņ×ÉņŚÉņä£ ņłśņłĀņĀü ņ╣śļŻī ņĀä, ļ▓ĀļØ╝Ēīīļ░Ć, ļō£ļĪ£ļäżļŗżļĪĀ ļśÉļŖö ņĢäļ»ĖņśżļŗżļĪĀņØä ĒĢ©Ļ╗ś ļ│ĄņÜ®ĒĢ£ Ļ▓ĮņÜ░, NOACņØś Ēśłņżæ ļåŹļÅäĻ░Ć ņ£ĀņØśĒĢśĻ▓ī ļåÆņĢśļŗż[135].
ĻĖ░ĒāĆ ņĢĮņĀ£
ņØ╝ļ░śņĀüņ£╝ļĪ£ NOACļŖö CYPļéś P-gp/breast cancer resistance protein (BCRP)ņØä ņ£ĀļÅäĒĢśĻ▒░ļéś ņ¢ĄņĀ£ĒĢśņ¦Ć ņĢŖļŖöļŗż. ņØ┤ļōż ļīĆņé¼ļź╝ ņØ┤ņÜ®ĒĢśļŖö ļ»ĖļŗżņĪĖļ×ī(CYP3A4), ļööĻ│ĪņŗĀ(P-gp), ņĢäĒåĀļ░öņŖżĒāĆĒŗ┤(P-gp, CYP3A4)Ļ│╝ņØś ļ│æņÜ® Ēł¼ņĢĮņØ┤ ņØ┤ļōż ņĢĮņĀ£ņØś Ēśłņżæ ļåŹļÅäļź╝ ņ£ĀņØśĒĢśĻ▓ī ļ│ĆĒÖöņŗ£Ēéżņ¦ĆļŖö ņĢŖļŖöļŗż.
ĒĢŁĒśłņåīĒīÉņĀ£ņØĖ Ēŗ░ņ╣┤ĻĘĖļĀÉļ¤¼(ticagrelor)ļŖö P-gp ņ¢ĄņĀ£ņĀ£ņØ┤ļŗż. ļŗżļ╣äĻ░ĆĒŖĖļ×Ć 110 mgĻ│╝ Ēŗ░ņ╣┤ĻĘĖļĀÉļ¤¼ņØś ļ│æņÜ® Ēł¼ņĢĮņØĆ ļŗżļ╣äĻ░ĆĒŖĖļ×Ć ļŗ©ļÅģ Ēł¼ņĢĮņŚÉ ļ╣äĒĢśņŚ¼ ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØś Cmaxļź╝ 65%Ļ╣īņ¦Ć ņ”ØĻ░Ćņŗ£Ēé©ļŗż. ļŗżļ╣äĻ░ĆĒŖĖļ×Ć Ēł¼ņŚ¼ Ēøä ļæÉ ņŗ£Ļ░äņØś Ēł¼ņĢĮ Ļ░äĻ▓®ņØä ļæÉĻ│Ā Ēŗ░ņ╣┤ĻĘĖļĀÉļ¤¼ 180 mgņØä Ēł¼ņĢĮĒĢśņśĆņØä ļĢīņŚÉļŖö ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØś CmaxņÖĆ AUC ņ”ØĻ░ĆĻ░Ć Ļ░üĻ░ü 23%ņÖĆ 27%ļĪ£ ĒÖĢņØĖļÉśņŚłļŗż[136]. Ēŗ░ņ╣┤ĻĘĖļĀÉļ¤¼ņØś ļČĆĒĢś ņÜ®ļ¤ē ļ│ĄņÜ®ņØ┤ ĒĢäņÜöĒĢĀ ļĢīļŖö ņØ┤ņÖĆ Ļ░ÖņØ┤ Ēł¼ņĢĮ Ļ░äĻ▓®ņØä ĻĖĖĻ▓ī ĒĢśņŚ¼ ļ│ĄņÜ®ĒĢśļŖö Ļ▓āņØä ĻČīĒĢ£ļŗż. Ēŗ░ņ╣┤ĻĘĖļĀÉļ¤¼ņÖĆ ļŗżļ╣äĻ░ĆĒŖĖļ×Ć 110 mgņØä ĒĢ©Ļ╗ś ļ│ĄņÜ®ĒĢśļŖö Ļ▓ĮņÜ░, ļŗżļ╣äĻ░ĆĒŖĖļ×Ć ļŗ©ļÅģ ļ│ĄņÜ®ņŚÉ ļ╣äĒĢśņŚ¼ ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØś AUCņÖĆ CmaxĻ░Ć Ļ░üĻ░ü 26%, 29% ņ”ØĻ░ĆĒĢśņśĆĻ│Ā, ņØ┤ļŖö RE-DUAL PCIņŚÉņä£ ĒÖĢņØĖļÉśņŚłļŗż. ĻĘĖ ņÖĖ ņĢĮņ┤łņŚÉ ļīĆĒĢ┤ņä£ļŖö ņāüĒśĖņ×æņÜ®ņØ┤ Ļ│╝ņåī ĒÅēĻ░ĆļÉśļŖö Ļ▓ĮĒ¢źņØ┤ ņ׳ļŗż. St. JohnŌĆÖs wortļŖö Ļ░ĢļĀźĒĢ£ CYP3A4Ļ│╝ P-gp ņ£ĀļÅäņĀ£ņØ┤ļ®░, NOAC ļåŹļÅäļź╝ Ļ░Éņåīņŗ£Ēé¼ Ļ░ĆļŖźņä▒ņ£╝ļĪ£ ņØĖĒĢśņŚ¼[137] NOACņÖĆņØś ļ│æņÜ® ņé¼ņÜ®ņØ┤ ĻČīņןļÉśņ¦Ć ņĢŖļŖöļŗż.
ņĢĮļÅÖĒĢÖņĀü ņāüĒśĖņ×æņÜ®
ņĢĮļÅÖĒĢÖņĀü ņāüĒśĖņ×æņÜ®Ļ│╝ ņāüĻ┤Ć ņŚåņØ┤ ļŗżļźĖ ĒĢŁņØæĻ│ĀņĀ£, ĒĢŁĒśłņåīĒīÉņĀ£, NSAIDsņØś ļ│æņÜ®ņØĆ ņČ£ĒśłņØś ņ£äĒŚśņØä ņ”ØĻ░Ćņŗ£Ēé©ļŗż[138-140]. ļö░ļØ╝ņä£, ņØ┤ļ¤░ ņĢĮņĀ£ņØś ļ│æņÜ®ņØĆ ņØ┤ļōØņØ┤ ņČ£Ēśłļ│┤ļŗż ļåÆļŗżĻ│Ā ĒīÉļŗ©ļÉśļŖö Ļ▓ĮņÜ░ ņŻ╝ņØśĒĢśņŚ¼ ņØ┤ļŻ©ņ¢┤ņĀĖņĢ╝ ĒĢ£ļŗż. NOACņÖĆ ļæÉ Ļ░Ćņ¦ĆņØś ĒĢŁĒśłņåīĒīÉņĀ£ļź╝ ļ│æņÜ®ĒĢśļŖö 3ņĀ£ ņÜöļ▓Ģ ĻĖ░Ļ░äņØĆ ņĄ£ļīĆĒĢ£ ĻĖ░Ļ░äņØä ņżäņØ┤ļŖö ļō▒ņØś ņĪ░ņ£©ņØ┤ ĒĢäņÜöĒĢśļŗż.
ļŗżņĀ£ ņĢĮņĀ£ ļ│ĄņÜ®
ņŚ¼ļ¤¼ ņĢĮņĀ£ ļ│ĄņÜ®ņØĆ ņĢĮļ¼╝ ņāüĒśĖņ×æņÜ®ņ£╝ļĪ£ ņØĖĒĢ£ ļČĆņ×æņÜ®ņØ┤ ņל ņāØĻĖ░ļŖö ņ£äĒŚśņØĖņ×ÉņØ┤ļŗż[141-143]. ĒĢśņ¦Ćļ¦ī, ROCKET-AFņÖĆ ARISTOTLEņŚÉņä£, 5Ļ░Ćņ¦Ć Ēś╣ņØĆ 9Ļ░Ćņ¦Ć ņØ┤ņāüņØś ļŗżņĢĮņĀ£ļź╝ ļ│ĄņÜ®ĒĢśļŖö ĒÖśņ×Éļōż ņŚŁņŗ£ NOACļŖö ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ņÖĆ ņ£Āņé¼ĒĢ£ ņ×äņāü Ļ▓░Ļ│╝ļź╝ ļ│┤ņśĆļŗż[142,143]. ņØ┤ļ¤░ Ļ▓░Ļ│╝ļŖö ĒĢ┤ņäØņŚÉ ņĀ£ĒĢ£ņĀÉņØ┤ ņ׳ņ¦Ćļ¦ī, ņŚ¼ļ¤¼ ņŚ░ĻĄ¼ņØś ņé¼Ēøä ļČäņäØņŚÉņä£ ĒÖĢņØĖļÉśņŚłĻ│Ā, ļŗżņĢĮņĀ£ ņżæņŚÉņä£ļÅä Ļ░ĢļĀźĒĢ£ CYP3A4 ņ¢ĄņĀ£ņĀ£(ketoconazole, ritonavir) ļśÉļŖö ņ£ĀļÅäņĀ£(phenytoin, rifampicin)ņÖĆņØś ļ│æņÜ®ņØĆ ĻĖłĒĢśņśĆļŗż. ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ĻĄ░ņŚÉņä£ļÅä ļŗżņĢĮņĀ£ ļ│ĄņÜ® ĒÖśņ×ÉņŚÉņä£ļŖö ņ×äņāü ņé¼Ļ▒┤ņØ┤ ņ”ØĻ░ĆĒĢśņśĆļŖöļŹ░ ņØ┤ļŖö ņĢĮļ¼╝ ņāüĒśĖņ×æņÜ®ļ┐Éļ¦ī ņĢäļŗłļØ╝, ņØ┤ļ¤░ ĒÖśņ×ÉļōżņØ┤ ĻĖ░ļ│ĖņĀüņ£╝ļĪ£ Ļ│Āņ£äĒŚśĻĄ░ņØ┤ĻĖ░ ļĢīļ¼ĖņØ┤ĻĖ░ļÅä ĒĢśļŗż. ļŗżņĢĮņĀ£ ļ│ĄņÜ®ļĀźņØ┤ NOAC ņé¼ņÜ®ņØś ĻĖłĻĖ░ļŖö ņĢäļŗłņ¦Ćļ¦ī, ņØ┤ļ¤░ Ļ│Āņ£äĒŚśĻĄ░ ĒÖśņ×ÉņŚÉņä£ļŖö ĒŖ╣ļ│äĒ׳ ņŻ╝ņØśĻ░Ć ĒĢäņÜöĒĢśļŗż.
ļ¦īņä▒ ņŗĀņ¦łĒÖś ļ░Å ņ¦äĒ¢ēļÉ£ Ļ░äņ¦łĒÖśņŚÉņä£ņØś NOAC
ņŗĀņן ļ░Å Ļ░ä ĻĖ░ļŖźņØĆ NOACņØś ļīĆņé¼ ļ░Å ļ░░ņäżņŚÉ ņżæņÜöĒĢ£ ņŚŁĒĢĀņØä ĒĢśļ»ĆļĪ£ NOAC ņé¼ņÜ® ļ░Å ņÜ®ļ¤ē Ļ▓░ņĀĢņŚÉ ļ░śļō£ņŗ£ Ļ│ĀļĀżļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż.
ļ¦īņä▒ ņŗĀņ¦łĒÖśņŚÉņä£ņØś Ļ▓ĮĻĄ¼ ĒĢŁņØæĻ│Ā ņÜöļ▓Ģ
ņŗ¼ļ░®ņäĖļÅÖņØĆ ļ¦īņä▒ ņŗĀņ¦łĒÖśņØś ļ░£ņāØĻ│╝ ņ¦äĒ¢ēņØä ņ£Āļ░£ĒĢśļ®░, ļ¦īņä▒ ņŗĀņ¦łĒÖś ĒÖśņ×ÉņŚÉņä£ ņŗĀĻĖ░ļŖźņØ┤ ņĀĆĒĢśļÉĀņłśļĪØ ņŗ¼ļ░®ņäĖļÅÖņØś ņ£Āļ│æļźĀ ļ░Å ļ░£ņāØļźĀņØ┤ ņāüņŖ╣ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[144-147]. ņŗĀņ¦łĒÖśņØä ļÅÖļ░śĒĢ£ ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉļŖö ņāēņĀäņ”Ø ļ░Å ņŗ¼Ļ░üĒĢ£ ņČ£Ēśł ņ£äĒŚśļÅä ļ¬©ļæÉĻ░Ć ņ”ØĻ░ĆĒĢśņŚ¼ ņØ┤ĒÖśņ£© ļ░Å ņé¼ļ¦ØļźĀņØä ņ”ØĻ░Ćņŗ£ĒéżĻĖ░ ļĢīļ¼ĖņŚÉ ņ£äĒŚśļÅä ņśłņĖĪ ļ░Å ņ╣śļŻīĻ░Ć ņēĮņ¦Ć ņĢŖļŗż[148,149]. ĒśäņĪ┤ĒĢśļŖö 4Ļ░£ņØś NOAC ļ¬©ļæÉ ņØ╝ņĀĢ ļČĆļČä ņŗĀņןņØä ĒåĄĒĢśņŚ¼ ļ░░ņäżļÉśļŖöļŹ░, ĻĘĖ ļ╣äņ£©ņØĆ ļŗżļ╣äĻ░ĆĒŖĖļ×Ć(80%), ņŚÉļÅģņé¼ļ░ś(50%), ļ”¼ļ░öļĪØņé¼ļ░ś(35%), ņĢäĒöĮņé¼ļ░ś(27%) ņł£ņØ┤ļŗż(Table 4).
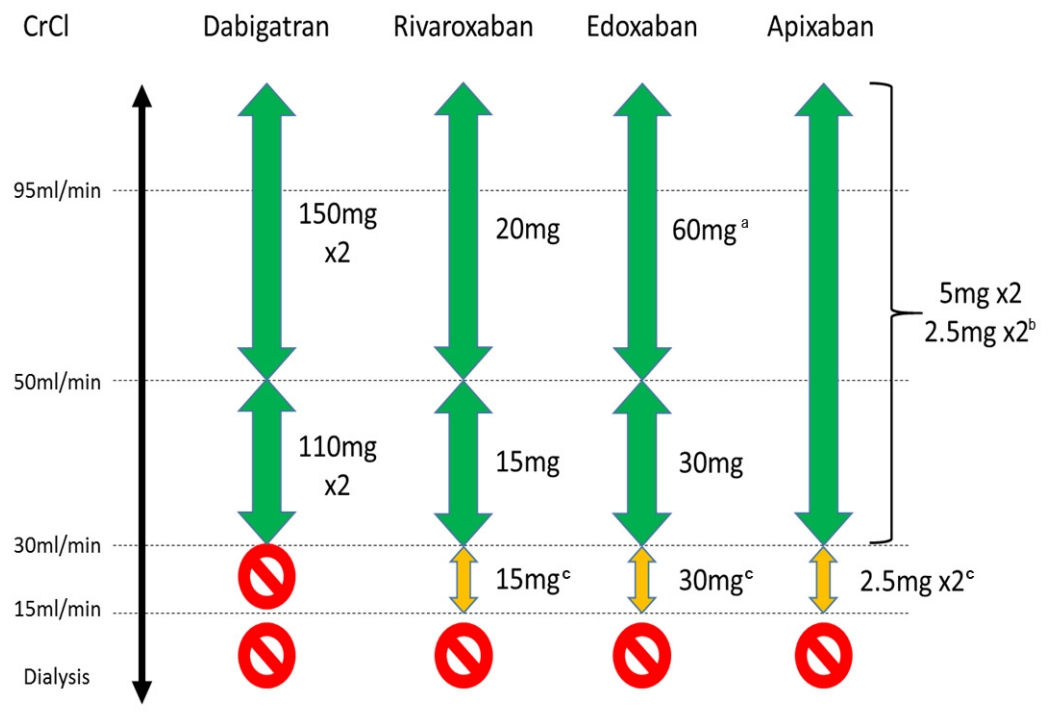
ļ¦īņä▒ ņŗĀņ¦łĒÖśņØä Ļ░Ćņ¦ä ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉņŚÉĻ▓ī Ļ▓ĮĻĄ¼ ĒĢŁņØæĻ│ĀņĀ£ļź╝ ņ▓śļ░®ĒĢśĻĖ░ ņĀä ņŗĀĻĖ░ļŖźņØś ĒÅēĻ░ĆņŚÉļŖö ņŚ¼ļ¤¼ Ļ│ĄņŗØņØ┤ ņé¼ņÜ®ļÉśĻ│Ā ņ׳ļŖöļŹ░, Ļ░üĻ░üņØś Ļ│ĄņŗØļ¦łļŗż ņןņĀÉĻ│╝ ļŗ©ņĀÉļōżņØ┤ ņ׳ļŗż. CKD-EPI Ļ│ĄņŗØņØĆ National Kidney FoundationņŚÉņä£ ĻČīņןĒĢśļŖö Ļ│ĄņŗØņ£╝ļĪ£, ļ¬©ļōĀ ļ▓öņ£äņØś ļ¦īņä▒ ņŗĀņ¦łĒÖś ļŗ©Ļ│äņŚÉņä£ ņŗĀļó░ļÅäĻ░Ć ļåÆņØĆ Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[150]. ĻĘĖļ¤¼ļéś NOAC ņé¼ņÜ®ņŚÉ ņ׳ņ¢┤ņä£ļŖö Cockcroft-Gault ļ░®ņŗØņØä ņØ┤ņÜ®ĒĢ£ ņŗĀĻĖ░ļŖź Ļ│äņé░(creatinine clearance, CrCl)ņØä ņŻ╝ļĪ£ ņé¼ņÜ®ĒĢśĻ▓ī ļÉśļŖöļŹ░, ņØ┤ļŖö ļīĆļČĆļČäņØś NOAC 3ņāü ļīĆĒæ£ ņŚ░ĻĄ¼ļōżņŚÉņä£ ņØ┤ ļ░®ņŗØņØ┤ ņé¼ņÜ®ļÉśņŚłĻĖ░ ļĢīļ¼ĖņØ┤ļŗż. ĒĢśņ¦Ćļ¦ī ļ¼┤ņŚćļ│┤ļŗż ņżæņÜöĒĢ£ ņĀÉņØĆ ņŗĀĻĖ░ļŖźņØś Ļ│äņé░ņØ┤ ņ¢┤ļ¢ż Ļ│ĄņŗØņ£╝ļĪ£ ņØ┤ļŻ©ņ¢┤ņ¦ĆļŖöņ¦Ć ļ│┤ļŗż ĻĖēņä▒ ņŗĀĻĖ░ļŖź ņĀĆĒĢśĻ░Ć ņ׳ļŖö ņāüĒā£Ļ░Ć ņĢäļŗī ņĢłņĀĢņĀüņØĖ ņāüĒā£ņŚÉņä£ ņŗĀĻĖ░ļŖźņØś ĒÅēĻ░ĆĻ░Ć ņØ┤ļŻ©ņ¢┤ņĀĖņĢ╝ ĒĢ£ļŗżļŖö ņĀÉņØ┤ļŗż.
ļśÉĒĢ£ NOACļź╝ ļ│ĄņÜ®ĒĢśļŖö ĒÖśņ×ÉļōżņØĆ ņŗĀĻĖ░ļŖź ņĀĆĒĢśņŚÉ ļīĆĒĢ£ ņĪ░ĻĖ░ Ļ░Éņ¦Ćļź╝ ņ£äĒĢśņŚ¼ ņĄ£ņåīĒĢ£ 1ļģä Ļ░äĻ▓®ņ£╝ļĪ£ ņŗĀĻĖ░ļŖźņŚÉ ļīĆĒĢ£ ĒÅēĻ░ĆĻ░Ć ņØ┤ļŻ©ņ¢┤ņĀĖņĢ╝ ĒĢ£ļŗż. ļ¦īņĢĮ ņŗĀĻĖ░ļŖź ņĀĆĒĢśĻ░Ć ņØ┤ļ»Ė ņĪ┤ņ×¼ĒĢśļŖö Ļ▓ĮņÜ░(CrCl < 60 mL/min)ņŚÉļŖö ļŹö ņ¦¦ņØĆ Ļ░äĻ▓®ņØś ņŗĀĻĖ░ļŖź ĒÅēĻ░ĆĻ░Ć ĒĢäņÜöĒĢ£ļŹ░, ņØ╝ļ░śņĀüņ£╝ļĪ£ ĒÖśņ×ÉņØś CrClļź╝ 10ņ£╝ļĪ£ ļéśļłł Ļ░ÆņØ┤ ņŗĀĻĖ░ļŖź Ļ▓Ćņé¼ņØś Ļ░äĻ▓®(Ļ░£ņøö)ņ£╝ļĪ£ ĻČīņןļÉ£ļŗż(ņśł: CrCl 30 mL/minņØś Ļ▓ĮņÜ░ 3Ļ░£ņøöņŚÉ ĒĢ£ ļ▓łņö® Ļ▓Ćņé¼ ĻČīņן). ļśÉĒĢ£ ĒÖśņ×ÉĻ░Ć Ļ│ĀļĀ╣, ļģĖņćĀ, ļŗżņ¢æĒĢ£ ļÅÖļ░ś ņ¦łĒÖś ļō▒ ņČöĻ░ĆņĀüņØĖ ņ£äĒŚśņØĖņ×ÉļōżņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ņØä Ļ▓ĮņÜ░ņŚÉļŖö ņČöĻ░ĆņĀüņØĖ ņŻ╝ņØś ļ░Å ņ¦¦ņØĆ Ļ░äĻ▓®ņØś ņŗĀĻĖ░ļŖź Ļ▓Ćņé¼Ļ░Ć ĒĢäņÜöĒĢĀ ņłś ņ׳ņ£╝ļ®░, ĒŖ╣Ē׳ ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØś Ļ▓ĮņÜ░ ņŗĀņן ļ░░ņäż ļ╣äņ£©ņØ┤ ļåÆĻĖ░ ļĢīļ¼ĖņŚÉ Ļ░üļ│äĒĢ£ ņŻ╝ņØśĻ░Ć ņÜöĻĄ¼ļÉ£ļŗż.
ĻĘĖ ņÖĆļŖö ļ░śļīĆļĪ£, ņŗĀĻĖ░ļŖźņØ┤ ĒÅēĻĘĀ ņØ┤ņāüņ£╝ļĪ£ ļåÆņØĆ ĒÖśņ×É(CrCl > 95 mL/min)ņŚÉņä£ ņŚÉļÅģņé¼ļ░ś(60 mg 1ņØ╝ 1ĒÜī)ņØś Ļ▓ĮņÜ░ ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ ļīĆļ╣ä ĻĘĖ ĒÜ©ļŖźņØ┤ Ļ░ÉņåīĒĢ£ļŗżļŖö Ļ┤Ćņ░░ Ļ▓░Ļ│╝Ļ░Ć ļ░£Ēæ£ļÉ£ ļ░ö ņ׳ņ¢┤ ņŻ╝ņØśĻ░Ć ņÜöĻĄ¼ļÉśļ®░, ļ»ĖĻĄŁ Food and Drug Administration (FDA)ņŚÉņä£ļŖö 2015ļģä ņŚÉļÅģņé¼ļ░śņØä CrClņØ┤ ļåÆņØĆ(> 95 mL/min) ĒÖśņ×ÉĻĄ░ņŚÉ ņé¼ņÜ®ĒĢśļŖö Ļ▓āņŚÉ ļīĆĒĢśņŚ¼ ļŗżļźĖ NOACļĪ£ ļ│ĆĻ▓ĮĒĢśņŚ¼ ņé¼ņÜ®ĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢ£ ļ░ö ņ׳ļŗż[24]. ĒĢśņ¦Ćļ¦ī ĒØźļ»ĖļĪŁĻ▓īļÅä ņØ┤ļ¤¼ĒĢ£ Ļ▓░Ļ│╝ļŖö ļ”¼ļ░öļĪØņé¼ļ░ś[151]ņØ┤ļéś ņĢäĒöĮņé¼ļ░ś[152]Ļ│╝ Ļ░ÖņØĆ Factor Xa inhibitor Ļ│äņŚ┤ņØś NOACļōżņŚÉņä£ ļ¬©ļæÉ ņ£Āņé¼ĒĢśĻ▓ī ĒÖĢņØĖļÉśĻ│Ā ņ׳ņ¢┤ Ē¢źĒøä ņČöĻ░ĆņĀüņØĖ ņŚ░ĻĄ¼ļōżņØ┤ ĒĢäņÜöĒĢ£ ņŗżņĀĢņØ┤ļŗż. ĻĘĖļ¤╝ņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā ENGAGE AF ņŚ░ĻĄ¼ņØś ņé¼Ēøä ļČäņäØņŚÉ Ļ▓░Ļ│╝ ņŗĀĻĖ░ļŖźņŚÉ ļö░ļØ╝ ņŚÉļÅģņé¼ļ░śņØś ņĢłņĀäņä▒ ļ░Å ņĀäļ░śņĀüņØĖ ņ×äņāü Ēś£ĒāØ(net clinical benefit)ņØĆ ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ ļīĆļ╣ä ņØ╝Ļ┤ĆņĀüņØĖ Ļ▓āņ£╝ļĪ£ ĒÖĢņØĖļÉśņŚłļŗżļŖö ņĀÉ[153], ĻĄŁļé┤ļź╝ ļ╣äļĪ»ĒĢ£ ņĢäņŗ£ņĢä ĒÖśņ×ÉļōżņØś ņ▓┤Ļ▓® ļ░Å CrClņØ┤ ņä£ĻĄ¼ņÖĆļŖö ņāüļŗ╣ĒĢ£ ņ░©ņØ┤Ļ░Ć ņ׳ņ¢┤ ņĢ×ņä£ ņ¢ĖĻĖēĒĢ£ ņä£ĻĄ¼ņØś ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļź╝ ĻĄŁļé┤ņŚÉ ņĀüņÜ®ĒĢśĻĖ░ņŚÉļŖö ļ¼┤ļ”¼Ļ░Ć ņ׳ļŗżļŖö ņĀÉņØä Ļ│ĀļĀżĒĢĀ ļĢī ĻĄŁļé┤ ļŹ░ņØ┤Ēä░ļź╝ ĻĖ░ļ░śņ£╝ļĪ£ ĒĢ£ ņČöĻ░ĆņĀüņØĖ ņŚ░ĻĄ¼Ļ░Ć ĒĢäņÜöĒĢśļŗż. ĻĄŁļé┤ņŚÉņä£ļŖö ļåÆņØĆ ņŗĀĻĖ░ļŖź ĒÖśņ×ÉņŚÉ ļīĆĒĢ£ ņČöĻ░ĆņĀüņØĖ ĻČīĻ│Ā ņé¼ĒĢŁņØĆ ņĢäņ¦ü ņŚåļŗż.
Ļ▓ĮļÅä ļ░Å ņżæļō▒ļÅäņØś ņŗĀņ¦łĒÖś(CrCl Ōēź 30 mL/min)ņŚÉņä£ņØś Ļ▓ĮĻĄ¼ ĒĢŁņØæĻ│ĀņĀ£
ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£Ļ░Ć Ļ▓ĮļÅä ļ░Å ņżæņ”ØļÅäņØś ņŗĀņ¦łĒÖśņØä ļÅÖļ░śĒĢ£ ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉņØś ļćīĻ▓Įņāē ļ░Å ņé¼ļ¦ØļźĀņØä Ļ░Éņåīņŗ£Ēé©ļŗżļŖö Ļ▓░Ļ│╝ļŖö ņØ┤ļ»Ė ņל ņĢīļĀżņĀĖ ņ׳ļŗż[154-157]. ņØ┤ņÖĆ ņ£Āņé¼ĒĢśĻ▓ī 4Ļ░£ņØś NOAC ļ¬©ļæÉ 3ņāü ņ×äņāü ņŚ░ĻĄ¼ļōżņŚÉņä£ Ļ▓ĮļÅä ļ░Å ņżæņ”ØļÅäņØś ņŗĀņ¦łĒÖś ĒÖśņ×ÉĻĄ░ņŚÉņä£ ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ ļīĆļ╣ä ņØ╝Ļ┤ĆņĀüņØĖ ĒÜ©ļŖź ļ░Å ņĢłņĀäņä▒ņØä ļ│┤ņØ┤Ļ│Ā ņ׳ļŗż[153,158-161]. ĒŖ╣Ē׳ ARISTOTLE ņŚ░ĻĄ¼ņØś ļČäņäØ Ļ▓░Ļ│╝ņŚÉņä£ļŖö CrCl Ļ░ÆņØ┤ ļé«ņØĆ ĒÖśņ×ÉņŚÉņä£ļÅä ņĢäĒöĮņé¼ļ░śņØś ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ ļīĆļ╣ä ļćīĻ▓Įņāē Ļ░Éņåī ĒÜ©ļŖźņØĆ ņ£Āņ¦ĆļÉśļ®┤ņä£ ņČ£Ēśł ņ£äĒŚśļÅä Ļ░ÉņåīņØś ņĀĢļÅäĻ░Ć ļŹö ļæÉļō£ļ¤¼ņ¦ĆļŖö Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉ£ļŗż[149,161]. ļ░śļ®┤ ļŗżļ╣äĻ░ĆĒŖĖļ×Ć 110 mg 1ņØ╝ 2ĒÜī ņÜ®ļ▓ĢņŚÉņä£ ļ│┤ņśĆļŹś ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ ļīĆļ╣ä ņČ£Ēśł ņ£äĒŚśļÅäņØś Ļ░ÉņåīļŖö CrCl < 50 mL/min ļ»Ėļ¦īņØś ĒÖśņ×ÉņŚÉņä£ļŖö ļ¬ģĒÖĢĒĢśņ¦Ć ņĢŖņØĆ Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉ£ļŗż[160].
ļ”¼ļ░öļĪØņé¼ļ░ś, ņĢäĒöĮņé¼ļ░ś, ņŚÉļÅģņé¼ļ░śņØś Ļ▓ĮņÜ░ Ļ░üĻ░üņØś 3ņāü ļ¼┤ņ×æņ£ä ļīĆņĪ░ ņŚ░ĻĄ¼ļōżņŚÉņä£ ņŗĀĻĖ░ļŖźņŚÉ ļö░ļØ╝ ņÜ®ļ¤ēņØä Ļ░Éļ¤ēĒĢśņśĆļŹś Ļ▓āņŚÉ ļ╣äĒĢśņŚ¼ ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØś ņ×äņāüņŚ░ĻĄ¼ņØĖ RE-LY ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņŗĀĻĖ░ļŖźņŚÉ ļö░ļźĖ Ļ░Éļ¤ē ņŚåņØ┤ 150 mg 1ņØ╝ 2ĒÜī ņÜ®ļ▓ĢĻ│╝ 110 mg 1ņØ╝ 2ĒÜī ņÜ®ļ▓ĢņØä ļ¼┤ņ×æņ£ä ļ░░ņĀĢĒĢśņŚ¼ ĻĘĖ ņ×äņāü Ļ▓░Ļ│╝ļź╝ ļ╣äĻĄÉĒĢśņśĆņ£╝ļ®░, Ēśäņ×¼ ņĢĮĒÆł ņ▓śļ░® ņäżļ¬ģņä£ņŚÉņä£ļŖö CrCl < 50 mL/minņØ┤ļ®┤ņä£ ņČ£ĒśłņØś Ļ│Āņ£äĒŚśĻĄ░ ĒÖśņ×ÉņŚÉņä£ļŖö 110 mg 1ņØ╝ 2ĒÜī ņÜ®ļ▓ĢņØä ĻČīņןĒĢśĻ│Ā ņ׳ņ£╝ļ®░, ņØ┤ļź╝ ļ░śņśüĒĢśņŚ¼ ļīĆĒĢ£ļČĆņĀĢļ¦źĒĢÖĒÜī ņŗ¼ļ░®ņäĖļÅÖ ĒĢŁņØæĻ│ĀņĀ£ ņäĀĒāØ ļ░Å ņÜ®ļ¤ē ĻČīĻ│Ā ņ¦Ćņ╣©ņŚÉņä£ļŖö ņØ┤ ĒÖśņ×ÉĻĄ░ņŚÉņä£ 110 mg 1ņØ╝ 2ĒÜī ņÜ®ļ▓ĢņØä ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż(Fig. 7).
ĒĢ£ĒÄĖ ņĀüņĀłņ╣ś ļ¬╗ĒĢ£ ņÜ®ļ¤ēņØś NOAC ņé¼ņÜ®ņØĆ ļīĆĻĘ£ļ¬© ŌĆśreal-worldŌĆÖ ĒÖśņ×ÉĻĄ░ņŚÉņä£ ņóŗņ¦Ć ņĢŖņØĆ ņśłĒøäļź╝ ļ│┤ņØ┤ļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ņ£╝ļ®░, ĒŖ╣Ē׳ ņŗĀĻĖ░ļŖź ņĀĆĒĢśĻ░Ć ļ¬ģĒÖĢĒĢśņ¦Ć ņĢŖņØĆ ĒÖśņ×ÉĻĄ░ņŚÉņä£ ņĀüņĀłņ╣ś ļ¬╗ĒĢ£ ņĀĆņÜ®ļ¤ē NOACņØś ņé¼ņÜ®ņŗ£ ņČ£Ēśł Ļ░ÉņåīņØś ņןņĀÉņØĆ ļÜ£ļĀĘĒĢśņ¦Ć ņĢŖņ£╝ļ®┤ņä£ ļćīĻ▓Įņāē ņ£äĒŚśņä▒ļ¦ī ņ”ØĻ░ĆĒĢśļŖö Ļ▓āņ£╝ļĪ£ ĒÖĢņØĖļÉśĻ│Ā ņ׳ņ¢┤ ņĀüņĀłĒĢ£ ņÜ®ļ¤ē Ļ▓░ņĀĢņØĆ ņ×äņāüņĀüņ£╝ļĪ£ ļ¦żņÜ░ ņżæņÜöĒĢ£ ņé¼ņĢłņØ┤ļØ╝ ĒĢĀ ņłś ņ׳Ļ▓Āļŗż[162].
ņżæņ”Ø ņŗĀņ¦łĒÖś(CrCl 15-29 mL/min)ņŚÉņä£ņØś Ļ▓ĮĻĄ¼ ĒĢŁņØæĻ│ĀņĀ£
ļīĆļČĆļČäņØś NOAC ļ¼┤ņ×æņ£ä ļīĆņĪ░ ņŚ░ĻĄ¼ļōżņŚÉņä£ļŖö CrCl < 30 mL/min ĒÖśņ×ÉĻĄ░ļōżņØä ņĀ£ņÖĖĒĢśņśĆĻĖ░ ļĢīļ¼ĖņŚÉ(ļŗ©, ņĢäĒöĮņé¼ļ░śņØś Ļ▓ĮņÜ░ ņåīņłśņØś CrCl 25-30 mL/min ĒÖśņ×ÉĻĄ░ ĒżĒĢ©) ņØ┤ ĻĄ¼Ļ░äņØś ņŗĀĻĖ░ļŖź ņĀĆĒĢśļź╝ Ļ░Ćņ¦ä ĒÖśņ×ÉĻĄ░ņŚÉ ļīĆĒĢ£ ļ¼┤ņ×æņ£ä ļīĆņĪ░ ņŚ░ĻĄ¼ ļŹ░ņØ┤Ēä░ļŖö ņĪ┤ņ×¼ĒĢśņ¦Ć ņĢŖļŖöļŗż. ļśÉĒĢ£, ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ ļśÉĒĢ£ ņØ┤ ĻĄ¼Ļ░äņØś ĒÖśņ×ÉĻĄ░ņŚÉņä£ ņĀäĒ¢źņĀüņ£╝ļĪ£ ĒÖĢņØĖļÉ£ ļ░öļŖö ņŚåļŖö ņāüĒā£ņØ┤ļŗż. ņØ┤ ĒÖśņ×ÉĻĄ░ņŚÉņä£ļŖö ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØś Ļ▓ĮņÜ░ Ēł¼ņŚ¼ ĻĖłĻĖ░ņØ┤ļ®░, ņØ┤ļź╝ ņĀ£ņÖĖĒĢ£ ļ”¼ļ░öļĪØņé¼ļ░ś, ņĢäĒöĮņé¼ļ░ś ĻĘĖļ”¼Ļ│Ā ņŚÉļÅģņé¼ļ░śņØś Ļ▓ĮņÜ░ Ļ░Éļ¤ēĒĢśņŚ¼ ņé¼ņÜ®ĒĢśļŖö Ļ▓āņØ┤ ņŖ╣ņØĖļÉśņ¢┤ ņ׳ļŗż(Fig. 6). Ļ░ü ņĢĮņĀ£ņØś ņĢĮļĀźĒĢÖ/ņĢĮļÅÖĒĢÖ ļ░Å ņŗĀļ░░ņäż ļ╣äņ£©, ņŗĀĻĖ░ļŖź ņĀĆĒĢś ĒÖśņ×ÉĻĄ░ņŚÉņä£ ĒÖĢņØĖļÉ£ ņĢłņĀäņä▒ņØä Ļ│ĀļĀżĒĢĀ ļĢī ņØ╝ļ░śņĀüņ£╝ļĪ£ļŖö ņĢäĒöĮņé¼ļ░ś ļśÉļŖö ņŚÉļÅģņé¼ļ░śņØś ņé¼ņÜ®ņØ┤ ņäĀĒśĖļÉśĻ│Ā ņ׳ņ£╝ļéś ņČöĻ░ĆņĀüņØĖ ļ¼┤ņ×æņ£ä ļīĆņĪ░ ņŚ░ĻĄ¼Ļ░Ć ĒĢäņÜöĒĢ£ ņŗżņĀĢņØ┤ļŗż.
ļ¦ÉĻĖ░ ņŗĀņ¦łĒÖś(CrCl < 15 mL/min ļśÉļŖö Ēł¼ņäØņ╣śļŻī)ņŚÉņä£ņØś Ļ▓ĮĻĄ¼ ĒĢŁņØæĻ│ĀņĀ£
ļ¦ÉĻĖ░ ņŗĀņ¦łĒÖśņØä Ļ░Ćņ¦ä ņŗ¼ļ░®ņäĖļÅÖ ĒÖśņ×ÉņŚÉĻ▓ī ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ņØś ĒÜ©ļŖźĻ│╝ ņ×äņāüņĀü ņØ┤ņØĄņŚÉ ļīĆĒĢ┤ņä£ļŖö ņĢäņ¦üĻ╣īņ¦Ć ļģ╝ļ×ĆņØ┤ ļ¦ÄņØĆļŹ░, ņØ┤ļŖö ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ņØś ļćīĻ▓Įņāē Ļ░Éņåī ĒÜ©Ļ│╝ļŖö ļČäļ¬ģĒĢśļéś ņČ£Ēśł ņ£äĒŚśņä▒ņØ┤ ĻĖēĻ▓®Ē׳ ņ”ØĻ░ĆĒĢśĻĖ░ ļĢīļ¼ĖņØ┤ļŗż[154,155,157]. Ēł¼ņäØņØä ļ░øļŖö ĒÖśņ×ÉĻĄ░ņŚÉņä£ņØś ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ņØś ĒÜ©ņÜ®ņä▒ņØä ņĪ░ņé¼ĒĢ£ ņ£ĀņØ╝ĒĢ£ ļō▒ļĪØ Ļ┤Ćņ░░ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņé¼ļ¦ØļźĀ ļō▒ņØä ĒżĒĢ©ĒĢśņŚ¼ ņĀäļ░śņĀüņØĖ ņ×äņāü Ēś£ĒāØ(net clinical benefit)ņØ┤ ĒÖĢņØĖļÉśņ¦Ć ņĢŖņĢśļŗż[154]. ļ¦ÉĻĖ░ ņŗĀņ¦łĒÖś ĒÖśņ×ÉņŚÉņä£ ņ£ĀņØśĒĢ┤ņĢ╝ ĒĢĀ ņé¼ņŗżņØĆ ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£Ļ░Ć ļ¦Éņ┤łļÅÖļ¦ź ļō▒ ĒśłĻ┤ĆņŚÉ ņäØĒÜīĒÖöļź╝ ņ£Āļ░£ĒĢśļŖö ņ╣śļ¬ģņĀüņØĖ ĒĢ®ļ│æņ”ØņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ļŗżļŖö ņĀÉņØ┤ļŗż[163-165].
ĒĢ£ĒÄĖ, ļ¦ÉĻĖ░ ņŗĀņ¦łĒÖś ļ░Å Ēł¼ņäØ ĒÖśņ×ÉĻĄ░ņŚÉņä£ņØś NOACņØś ĒÜ©ļŖźĻ│╝ ņĢłņĀäņä▒ ņŚŁņŗ£ ņ×ģņ”ØļÉśņ¦Ć ņĢŖņĢśņ£╝ļ®░, ņØ┤ņŚÉ ļö░ļØ╝ ĻĄŁļé┤ņŚÉņä£ ņØ┤ļ¤¼ĒĢ£ ĒÖśņ×ÉĻĄ░ņŚÉņä£ NOACņØś ņé¼ņÜ®ņØĆ ĻĖłĻĖ░ņØ┤ļŗż. ņĄ£ĻĘ╝ Ēł¼ņäØ ĒÖśņ×ÉņŚÉĻ▓ī(FDA ņŖ╣ņØĖ ņŚåņØ┤) ņ▓śļ░®ļÉ£ ļ”¼ļ░öļĪØņé¼ļ░ś ļ░Å ļŗżļ╣äĻ░ĆĒŖĖļ×ĆņØś Ļ▓ĮņÜ░ ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ ļīĆļ╣ä ņ×ģņøÉņ£© ļ░Å ņé¼ļ¦ØļźĀņØä ņ”ØĻ░Ćņŗ£ĒéżļŖö Ļ▓āņØ┤ ĒÖĢņØĖļÉ£ ļ░ö ņ׳ļŗż[166].
ļ░śļ®┤ ļ»ĖĻĄŁ(ņ£Āļ¤ĮņØĆ ĒĢ┤ļŗ╣ ņŚåņØī)ņŚÉņä£ļŖö ņĢĮļĀźĒĢÖ/ņĢĮļÅÖĒĢÖ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļź╝ ņ░ĖĻ│ĀĒĢśņŚ¼ ņŗĀļ░░ņäż ļ╣äņ£©ņØ┤ Ļ░Ćņן ņĀüņØĆ NOACņØĖ ņĢäĒöĮņé¼ļ░śņØś 5 mg 1ņØ╝ 2ĒÜī ņÜ®ļ▓ĢņØ┤ Ēśäņ×¼ Ēł¼ņäØ ĒÖśņ×ÉĻĄ░ ņé¼ņÜ®ņŚÉņä£ ļ»ĖĻĄŁ FDAņØś ĒŚłĻ░Ćļź╝ ļ░øņØĆ ņāüĒā£ņØ┤ļŗż. ĻĘĖļ¤¼ļéś 5 mg 1ņØ╝ 2ĒÜī ņÜ®ļ▓ĢņŚÉ ļ╣äĒĢśņŚ¼ 2.5 mg 1ņØ╝ 2ĒÜī ņÜ®ļ▓ĢņØ┤ ļŹö Ēśłņżæ ļåŹļÅäĻ░Ć ĒĢ®ļŗ╣ĒĢśļŗżļŖö ņŚ░ĻĄ¼ Ļ▓░Ļ│╝Ļ░Ć ņ׳ļŗż[167]. ļ░śļ®┤ ņĄ£ĻĘ╝ņŚÉļŖö 5 mg 1ņØ╝ 2ĒÜī ņÜ®ļ▓ĢņØ┤ ļćīĻ▓Įņāē/ņĀäņŗĀņāēņĀäņ”Ø ņ£äĒŚśļÅä ļ░Å ņé¼ļ¦ØļźĀņØä ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ ļīĆļ╣ä Ļ░Éņåīņŗ£Ēé©ļŗżļŖö ĒøäĒ¢źņĀü ņŚ░ĻĄ¼Ļ░Ć ļ░£Ēæ£ļÉ£ ļ░ö ņ׳ņ¢┤[168], ņĢäņ¦üĻ╣īņ¦Ć ņĀüņĀłĒĢ£ ņÜ®ļ¤ēņŚÉ ļīĆĒĢ£ ļŗĄņØĆ ņŚåļŗż. ļŗżļźĖ NOACņØś Ļ▓ĮņÜ░, ļ¦ÉĻĖ░ ņŗĀņ¦łĒÖś ĒÖśņ×ÉņŚÉņä£ņØś ņĀüņĀłĒĢ£ Ēśłņżæ ļåŹļÅäļź╝ ļ│┤ņØ╝ ņłś ņ׳ļŖö ņĢĮļ¼╝ņØś ņÜ®ļ¤ēņØä ņŚÉļÅģņé¼ļ░śņØś Ļ▓ĮņÜ░ 15 mg 1ņØ╝ 1ĒÜī, ļ”¼ļ░öļĪØņé¼ļ░śņØś Ļ▓ĮņÜ░ļŖö 10 mg 1ņØ╝ 1ĒÜī ņÜ®ļ▓Ģņ£╝ļĪ£ ļ│┤Ļ│ĀĒĢ£ ņŚ░ĻĄ¼ļōżņØ┤ ņ׳ļŗż[169,170].
ĒĢśņ¦Ćļ¦ī Ļ░Ćņן ņżæņÜöĒĢ£ ņĀÉņØĆ Ēśłņżæ ļåŹļÅä ļ░Å Ļ┤Ćņ░░ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļŖö ņ░ĖĻ│Ā ņ×ÉļŻīņŚÉ ļČłĻ│╝ ĒĢśļ®░, NOACļź╝ ļ¦ÉĻĖ░ ņŗĀņ¦łĒÖś ĒÖśņ×ÉņŚÉĻ▓ī ņé¼ņÜ®ĒĢśĻĖ░ ņ£äĒĢ┤ņä£ļŖö ļīĆĻĘ£ļ¬© ņŚ░ĻĄ¼ļź╝ ĒåĄĒĢ£ ņ×äņāüņĀü ņØ┤ļōØņØ┤ ļ░ØĒśĆņĀĖņĢ╝ ĒĢĀ Ļ▓āņØ┤ļØ╝ļŖö ņĀÉņØ┤ļŗż. Ēśäņ×¼ ņĢäĒöĮņé¼ļ░śņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ 2Ļ░£ņØś ņŚ░ĻĄ¼Ļ░Ć ņ¦äĒ¢ē ņżæņØ┤ĻĖ░ ļĢīļ¼ĖņŚÉ ĻĘĖ Ļ▓░Ļ│╝Ļ░Ć ņŻ╝ļ¬®ļÉ£ļŗż.
ņŗĀņØ┤ņŗØņØä ļ░øņØĆ ĒÖśņ×ÉĻĄ░ņŚÉņä£ņØś NOAC ņé¼ņÜ®ņØĆ Ēśäņ×¼Ļ╣īņ¦Ć ļŹ░ņØ┤Ēä░Ļ░Ć ņŚåņ£╝ļ®░, ņØ┤ļ¤¼ĒĢ£ ĒÖśņ×ÉĻĄ░ņŚÉĻ▓ī NOACļź╝ ņ▓śļ░®ĒĢĀ ļĢīņŚÉļŖö ņŗĀĻĖ░ļŖźņŚÉ ļ¦×ņČöņ¢┤ ņÜ®ļ¤ēņØä Ļ▓░ņĀĢĒĢśļÉś ļīĆļČĆļČäņØś ĒÖśņ×ÉļōżņØ┤ ļ®┤ņŚŁņ¢ĄņĀ£ņĀ£ļź╝ ļ│ĄņÜ®ĒĢśĻ│Ā ņ׳ĻĖ░ ļĢīļ¼ĖņŚÉ ņĢĮņĀ£ Ļ░ä ņāüĒśĖņ×æņÜ®ņŚÉ ņŻ╝ņØśĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż.
Ļ░äņ¦łĒÖśņŚÉņä£ņØś NOAC ņé¼ņÜ®
ņ¦äĒ¢ēļÉ£ Ļ░äņ¦łĒÖśņØĆ ņČ£Ēśł ņ£äĒŚśņä▒ņØä ļåÆņØ╝ļ┐É ņĢäļŗłļØ╝ ĒśłņĀä ņāØņä▒ņØä ņ┤ēņ¦äņŗ£Ēé¼ ņłś ņ׳ļŗż[171]. ļśÉĒĢ£ Ļ░ä ļ░░ņäż ļ░Å ņĢĮļ¼╝ ļīĆņé¼ņŚÉ ņśüĒ¢źņØä ņŻ╝ņ¢┤ ņĢĮļ¼╝ ļ░śņØæņØä ļ│ĆĒÖöņŗ£Ēéżļ®░ ņĢĮļ¼╝ ņ£Āļ░£ Ļ░ä ņåÉņāüņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ļŗż[172]. ļśÉĒĢ£ ņ¦äĒ¢ēļÉ£ Ļ░äņ¦łĒÖś ļ░Å ņØæĻ│Ā ņןņĢĀļź╝ Ļ░Ćņ¦ä ĒÖśņ×ÉļŖö INR ņłśņ╣śĻ░Ć ņ×Éņ▓┤ņĀüņ£╝ļĪ£ ņāüņŖ╣ļÉśņ¢┤ ņ׳ļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦ÄņĢä ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ļź╝ ņ▓śļ░®ĒĢĀ Ļ▓ĮņÜ░ ņĀüņĀłĒĢ£ ņÜ®ļ¤ē ņĪ░ņĀłņØ┤ ņēĮņ¦Ć ņĢŖņØĆ Ļ▓ĮņÜ░Ļ░Ć ļ¦Äļŗż[173]. ļ¬ģļ░▒ĒĢ£ ĒÖ£ļÅÖņä▒ Ļ░äņ¦łĒÖśņØä Ļ░Ćņ¦ä ĒÖśņ×ÉĻĄ░, ņ”ē Ļ░äĻ▓Įļ│ĆņØ┤ ņ׳Ļ▒░ļéś ņ¦ĆņåŹņĀüņØĖ Ļ░äņłśņ╣ś ļ░Å ĒÖ®ļŗ¼ ņłśņ╣śņØś ņāüņŖ╣ņØä ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░ ļīĆĻĘ£ļ¬© NAOC 3ņāü ļ¼┤ņ×æņ£ä ļīĆņĪ░ ņŚ░ĻĄ¼ņŚÉņä£ ņĀ£ņÖĖļÉśņŚłļŗż[21,23,24,174]. ĻĘĖļ¤¼ļ»ĆļĪ£ 4Ļ░£ņØś NOAC ļ¬©ļæÉ Child-Truscott-Pugh CņØś Ļ░äĻ▓Įļ│Ć ļō▒ ņØæĻ│Ā ņןņĢĀ ļ░Å ļåÆņØĆ ņČ£Ēśł ņ£äĒŚśņä▒ņØä Ļ░Ćņ¦ä Ļ░äņ¦łĒÖśņŚÉņä£ļŖö ĻĖłĻĖ░ņØ┤ļŗż(Table 5). Child B Ļ░äĻ▓Įļ│Ć ĒÖśņ×ÉņØś Ļ▓ĮņÜ░ ļ”¼ļ░öļĪØņé¼ļ░ś ņé¼ņÜ®ņ£╝ļĪ£ Ļ░ä ņłśņ╣ś ņāüņŖ╣ņØ┤ ļ│┤Ļ│ĀļÉśņŚłĻĖ░ ļĢīļ¼ĖņŚÉ ĻĖłĻĖ░ņØ┤ļ®░[175], ļŗżļ╣äĻ░ĆĒŖĖļ×Ć, ņĢäĒöĮņé¼ļ░ś ĻĘĖļ”¼Ļ│Ā ņŚÉļÅģņé¼ļ░śņØś Ļ▓ĮņÜ░ļŖö ņŻ╝ņØś ĒĢśņŚÉ Ļ░Éļ¤ēĒĢśņŚ¼ Ēł¼ņŚ¼ĒĢĀ Ļ▓āņØ┤ ĻČīĻ│ĀļÉ£ļŗż. 2006ļģäņŚÉ Ļ░ä ļÅģņä▒ņ£╝ļĪ£ ņØĖĒĢśņŚ¼ ximelagatranņØ┤ ņŗ£ņןņŚÉņä£ Ēć┤ņČ£ļÉśņŚłĻĖ░ņŚÉ NOACņØś Ļ░ä ļÅģņä▒ņŚÉ ļīĆĒĢ£ ņÜ░ļĀżĻ░Ć ņ׳ņŚłņ£╝ļéś[176], NOAC ņŚ░ĻĄ¼ļōżņŚÉņä£ Ļ░ä ļÅģņä▒ņŚÉ ļīĆĒĢ£ ļ│┤Ļ│ĀļŖö ņŚåņŚłĻĖ░ņŚÉ ņŗżņĀ£ņĀüņØĖ NOACņØś Ļ░ä ļÅģņä▒ņØĆ ļ╣äĒāĆļ»╝ K ĻĖĖĒĢŁņĀ£ļ│┤ļŗż ļé«ņØä Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż[177,178].
Ļ▓░ ļĪĀ
NOACļŖö ņÖĆĒīīļ”░ņŚÉ ļ╣äĒĢśņŚ¼ ļ╣äĻĄÉņĀü ņēĮĻ▓ī ņé¼ņÜ®ĒĢĀ ņłś ņ׳ļŗż. ĒĢśņ¦Ćļ¦ī ņé¼ņÜ®ņŚÉ ļÅäņøĆņØ┤ ļÉśļŖö Ļ▓ĮņÜ░ņØĖņ¦Ć ņÜ░ņäĀ ņĀüņØæņ”ØņŚÉ ļīĆĒĢ£ ĒÖĢņØĖņØ┤ ĒĢäņÜöĒĢśļŗż. Ēśäņ×¼ ĻĄŁļé┤ņŚÉņä£ļŖö ļäż Ļ░Ćņ¦ĆņØś NOACĻ░Ć ņ▓śļ░® Ļ░ĆļŖźĒĢśļ®░ ļéśņØ┤, ņ▓┤ņżæ ļ░Å ņŗĀĻĖ░ļŖźĻ│╝ Ļ░ÖņØĆ ņ×äņāü ņÜöņØĖĻ│╝ ļ│ĄņÜ®ļ░®ļ▓ĢņŚÉ ļö░ļźĖ ĒÖśņ×ÉņØś ņäĀĒśĖļÅä ļō▒ņŚÉ ļö░ļØ╝ ņĢīļ¦×ņØĆ NOACļź╝ ņäĀĒāØĒĢśĻ│Ā Ļ░üĻ░üņØś ņÜ®ļ¤ē Ļ░Éļ¤ē ĻĖ░ņżĆņŚÉ ļö░ļØ╝ Ļ░Éļ¤ēĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż. ļŗżļźĖ ņĢĮņĀ£ņÖĆņØś ņāüĒśĖņ×æņÜ®ņØ┤ ņÖĆĒīīļ”░ļ│┤ļŗżļŖö ņĀüņ¦Ćļ¦ī ņĪ┤ņ×¼ĒĢśļ»ĆļĪ£ NOACņØś ņ▓śļ░®ņØä ņŗ£ņ×æĒĢśĻ▒░ļéś ņ£Āņ¦ĆĒĢĀ ļĢī Ēśäņ×¼ ļ│ĄņÜ®ĒĢśĻ│Ā ņ׳Ļ▒░ļéś ņāłļĪŁĻ▓ī ņČöĻ░ĆļÉ£ ņĢĮņĀ£ņŚÉ ļīĆĒĢ£ ĒÖĢņØĖņØ┤ ĒĢäņÜöĒĢśļŗż. NOACļŖö ņÖĆĒīīļ”░Ļ│╝ ļŗ¼ļ”¼ ņ¦¦ņØĆ ļ░śĻ░ÉĻĖ░ļź╝ Ļ░Ćņ¦Ćļ»ĆļĪ£ ņ▓śļ░®ņØä ņ£Āņ¦ĆĒĢĀ ļĢī ņĢĮņĀ£ ņł£ņØæļÅäļź╝ ņ£Āņ¦ĆĒĢśļŖö Ļ▓āņØ┤ ņżæņÜöĒĢśļŗż. ļö░ļØ╝ņä£ ņØ┤ļź╝ ņ£äĒĢśņŚ¼ ĒÖśņ×ÉņØś ĻĄÉņ£Ī ļō▒ Ļ░ĆļŖźĒĢ£ ļ¬©ļōĀ ļ░®ļ▓ĢņØä ņĀüņĀłĒĢśĻ▓ī ņé¼ņÜ®ĒĢśņŚ¼ņĢ╝ ĒĢśĻ▓Āļŗż. ĻĘĖ ņÖĖ ņŗĀĻĖ░ļŖź ļśÉļŖö Ļ░äĻĖ░ļŖź ņןņĢĀĻ░Ć ņ׳ļŖö Ļ▓ĮņÜ░ ņé¼ņÜ®ņŚÉ ņ£ĀņØśĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






