허혈성 대장염에서 내시경 지혈로 조절되지 않는 출혈에 대한 영상의학적 중재 치료: 증례군 보고
Radiologic Intervention for Endoscopy-Uncontrolled Bleeding in Ischemic Colitis: A Case Series
Article information
Trans Abstract
Ischemic colitis (IC), a common cause of lower gastrointestinal bleeding, is typically managed with conservative treatment. However, when hematochezia persists despite endoscopic hemostasis, radiologic intervention becomes a viable therapeutic alternative. This report aims to present three cases of IC associated with massive bleeding successfully treated using radiologic therapies. One patient with IC secondary to occlusive disease, characterized by significant stenosis at the superior mesenteric artery orifice, underwent stent placement, while the other two patients with non-occlusive IC were treated with embolization using microcatheters and Gelfoam. All cases resulted in technical and clinical success, with no procedure-related complications. This case series highlights the potential role of radiologic intervention as an effective, minimally invasive treatment option for select patients with IC who present with persistent hematochezia despite conservative or endoscopic management.
INTRODUCTION
Ischemic colitis (IC), the most common cause of gastrointestinal ischemia, is the second leading cause of hematochezia among hospitalized patients [1]. Arterial bleeding occurs in approximately 11.8% of severe IC cases and is associated with adverse outcomes, including higher rates of rebleeding, increased need for surgical intervention, and longer hospital stays than other colonic pathologies [1]. Risk factors for bleeding include anticoagulant use, severe pulmonary disease, and renal dysfunction [1,2]. Inpatient-onset bleeding is associated with higher risks of both rebleeding and mortality [1]. Clinical presentation ranges from mild, reversible mucosal injury to irreversible transmural necrosis, with symptoms such as hematochezia, non-bloody diarrhea, anemia, and hypotension [3]. Most patients (75-85%) experience self-limited disease and respond well to medical management [1]. Initial medical management includes intravenous fluid resuscitation, blood transfusion, and bowel rest [2]. However, while most cases resolve with conservative treatment, severe presentations associated with hemodynamic instability may require additional therapeutic interventions. When hematochezia is persistent or associated with signs of arterial bleeding, timely intervention beyond supportive care may be necessary. These cases often involve focal ischemic ulcers or visible vessels, both of which are associated with a heightened risk of ongoing or recurrent bleeding despite medical management [1,2].
In cases involving bleeding from a few ulcerations, endoscopic hemostasis may serve as the initial treatment approach [1]. If bleeding persists despite endoscopic therapy, surgical intervention should be considered [4]. As a less invasive alternative, radiologic intervention, typically performed via endovascular angiographic embolization, may serve as an effective salvage strategy. In select cases where IC results from vascular occlusion, stent placement may be appropriate. Therefore, this report aims to present cases of severe hematochezia secondary to IC that were successfully managed with radiologic intervention.
This study was approved with an exemption from full review by the Institutional Review Board (IRB) of Bundang Jesaeng Hospital (IRB No. DMC 2025-06-001), as it involved a retrospective chart review posing no more than minimal risk to participants.
CASE REPORT
We present three cases of ischemic colitis manifesting as severe hematochezia, all of which were successfully managed with radiologic intervention (Table 1).

Baseline characteristics and clinical outcomes of the patients
Case 1
A 67-year-old male patient presented to the hospital with watery diarrhea and abdominal pain as his primary complaints. He had no known underlying medical conditions. Before admission, he experienced five episodes of hematochezia, with an estimated blood loss of approximately one cup per episode. He sought medical attention at the gastroenterology department and was admitted with a provisional diagnosis of ischemic colitis.
On physical examination, the patient exhibited tachycardia. His vital signs were as follows: blood pressure, 149/98 mmHg; heart rate, 118 beats per minute; body temperature, 36.1℃. Initial laboratory investigations revealed a hemoglobin level of 14.1 g/dL (reference range, 13-17), indicating no evidence of anemia. However, there was a mild elevation in C-reactive protein at 3.57 mg/dL (reference range, 0.00-0.80).
On the day of admission, sigmoidoscopy was performed, revealing findings consistent with ischemic colitis (Fig. 1A, B). Abdominopelvic computed tomography (CT) conducted the same day demonstrated ischemic colitis involving the ascending and descending colon. The imaging findings suggested ischemia within the superior mesenteric artery (SMA) territory, likely due to significant stenosis at the SMA orifice. Further evaluation of the CT scan revealed more than 70% stenosis at the SMA origin.

Endoscopic images of diffuse ulcerative edematous mucosal wall thickening consistent with ischemic colitis. (A, B) Endoscopic findings revealed diffuse ulcerative and edematous thickening of the colonic mucosa, consistent with ischemic colitis in patient 1. (C, D) Diffuse ischemic changes of the mucosa and longitudinal, shallow ulcers at the mid-transverse colon in patient 2, with endoscopic hemoclipping performed. (E, F) Multiple active ulcers with exposed vessels at the distal descending colon in patient 3. Hemoclips were applied to the ulcers for hemostasis.
Despite conservative management, the patient’s symptoms persisted, with ongoing hematochezia. Given the lack of clinical improvement and concerns regarding persistent bowel ischemia due to significant stenosis at the SMA orifice, radiologic intervention was performed 2 days after sigmoidoscopy to restore mesenteric perfusion and prevent further ischemic injury. A balloon-mounted metallic stent was successfully deployed at the site of severe focal stenosis at the SMA orifice (Fig. 2A). Post-procedural abdominal aortography confirmed significant improvement in arterial patency, with resolution of the stenosis (Fig. 2B). No complications were observed. The patient showed a favorable clinical response and was successfully discharged 6 days after stent placement.
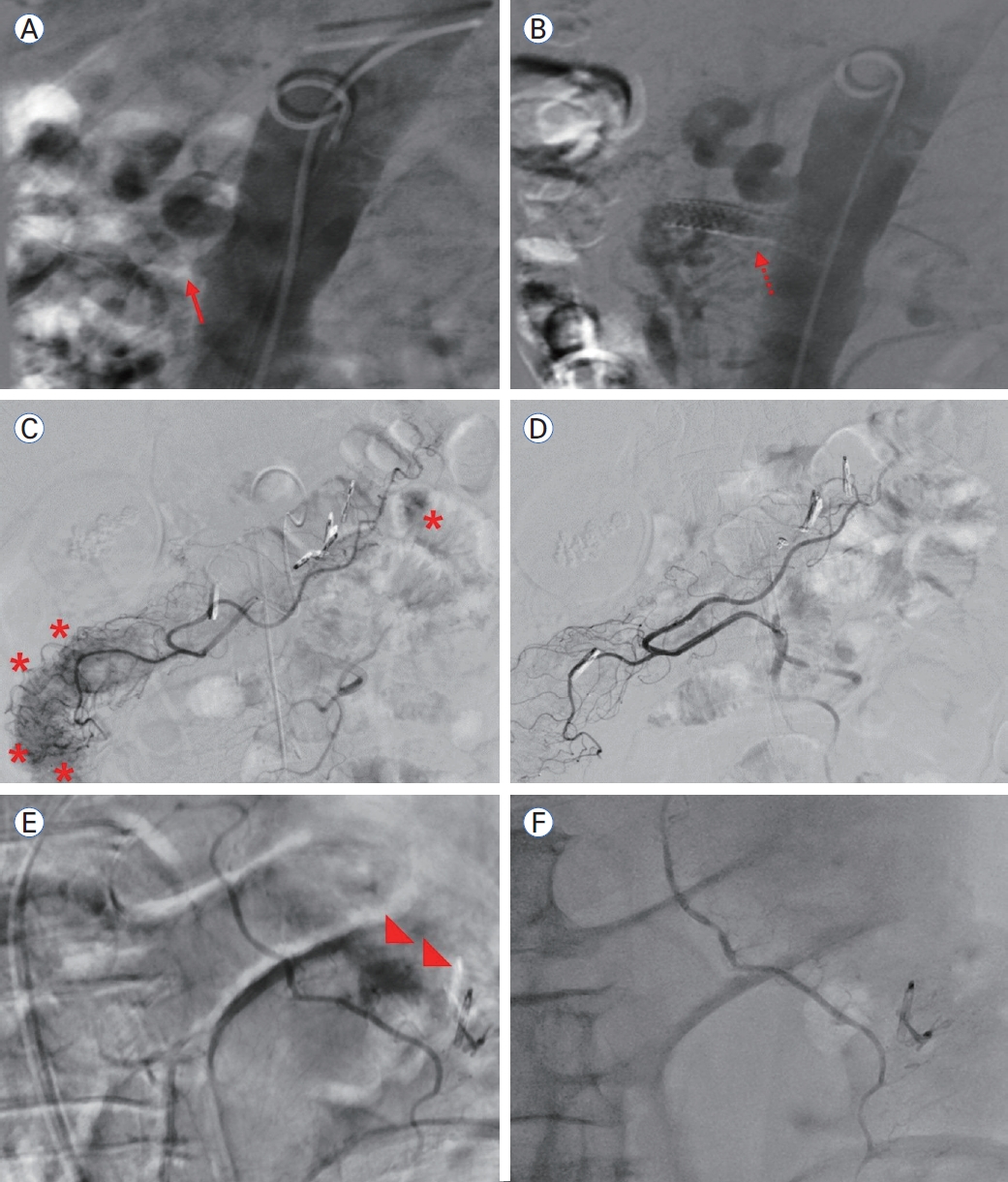
(A) Severe focal stenosis is observed at the SMA orifice (arrow). (B) A balloon-mounted metallic stent was inserted at the SMA orifice, restoring blood flow (dotted arrow). (C, E) Diffuse active arterial bleeding is observed from the middle colic artery of the SMA (asterisks and arrowheads). (D, F) Embolization was performed using a microcatheter and gelfoam, resulting in the cessation of bleeding. SMA, superior mesenteric artery.
Case 2
A 69-year-old male patient with a history of colon cancer surgery presented to the emergency department with hematochezia. His medical history was significant for hypertension, chronic kidney disease, stroke, and small cell lung cancer. He was admitted to the gastroenterology department for further evaluation and management of hematochezia.
On admission, the patient exhibited hemodynamic instability, with a blood pressure of 99/65 mmHg, heart rate of 107 beats per minute, and body temperature of 36.2℃. Initial laboratory investigations revealed severe anemia and thrombocytopenia, with a hemoglobin level of 4.1 g/dL (reference range, 13.0-17.0) and a platelet count of 75,000/mm3 (reference range, 150,000-400,000).
Despite 6 days of conservative management, hematochezia persisted. Therefore, a colonoscopy was performed, which revealed findings consistent with ischemic colitis (Fig. 1C). Endoscopic hemostasis was achieved using clip placement for a Forrest Ib ulcer bleed (Fig. 1D). Although the hematochezia temporarily resolved, the patient experienced a severe recurrence the following day. Given the ongoing hemorrhage and the patient’s high-risk clinical profile, including hemodynamic instability, severe anemia, thrombocytopenia, and multiple comorbidities, as well as poor endoscopic visualization during the prior procedure, radiologic intervention was pursued as a salvage therapy to achieve definitive hemostasis and prevent further clinical deterioration. Angiography demonstrated contrast extravasation in multiple branches of the SMA (Fig. 2C). Superselective embolization of the middle colic artery, a branch of the superior mesenteric artery, was performed using a microcatheter and gelfoam. Post-embolization angiography confirmed the absence of active arterial bleeding (Fig. 2D), and the procedure was completed without complications. A follow-up CT scan of the abdomen and pelvis performed the next day showed no evidence of ongoing hemorrhage. The patient remained hemodynamically stable and was discharged safely on post-procedure day 9.
Case 3
A 79-year-old male patient presented to the emergency department with dyspnea as the primary complaint. His medical history was significant for asbestosis and hypertension. Upon arrival, the patient was initially alert; however, he progressively became drowsy, with a respiratory rate increasing to 35 breaths per minute. Given the deterioration in respiratory status, endotracheal intubation was performed in the emergency department, and the patient was subsequently admitted to the intensive care unit for the management of pneumonia.
On initial evaluation, the patient exhibited hypertension and tachycardia, with a blood pressure of 158/72 mmHg, heart rate of 103 beats per minute, and body temperature of 36.7℃. Arterial blood gas analysis demonstrated respiratory acidosis, with a pH of 7.2 (reference range, 7.35-7.45), partial pressure of carbon dioxide (pCO2) of 66.7 mmHg (reference range, 32-45), partial pressure of oxygen (pO2) of 130.0 mmHg (reference range, 75-100), and bicarbonate concentration of 23.6 mmol/L (reference range, 21-29). Additionally, laboratory findings were notable for anemia (hemoglobin, 10.7 g/dL; reference range, 13.0-17.0) and thrombocytopenia (platelet count, 125,000/mm3; reference range, 150,000-400,000).
On hospital day 13, the patient developed severe hematochezia. Abdominal CT angiography was performed, revealing active bleeding and bowel wall thickening in the descending colon. Subsequent sigmoidoscopy confirmed ischemic colitis and identified an ulcer with an exposed vessel (Fig. 1E). Endoscopic clipping was performed on the ischemic ulcer to achieve hemostasis (Fig. 1F), resulting in temporary cessation of bleeding. However, recurrent hemorrhage occurred shortly thereafter, and given the patient’s advanced age, hemodynamic instability, and poor general condition due to pneumonia, radiologic intervention was deemed necessary to achieve definitive hemostasis and prevent further clinical decline.
Selective SMA angiography demonstrated active extravasation of contrast medium near the clipping site in the descending colon (Fig. 2E). Embolization of the actively bleeding site within the middle colic artery was performed using a microcatheter and gelfoam. Post-embolization angiography confirmed successful hemostasis, with no evidence of residual arterial bleeding (Fig. 2F). No immediate procedure-related complications were observed.
The following day, a repeat abdominal and pelvic CT scan demonstrated no ongoing bleeding. Seven days after embolization, follow-up sigmoidoscopy indicated that the ischemic colitis was in the healing phase. While the patient remained free of hematochezia, he ultimately succumbed to pneumo-nia 58 days after embolization.
DISCUSSION
IC may lead to several complications, including transmural necrosis, stricture formation, perforation, and arterial bleeding [1,5]. Among these, arterial bleeding, while relatively uncommon, significantly affects patient outcomes. Studies show that arterial bleeding occurs in approximately 11.8% of patients with IC presenting with severe hematochezia and is associated with higher rates of rebleeding, surgical intervention, and mortality [2]. These findings highlight the need for early recognition and timely management of such complications.
The pathogenesis of IC is primarily attributed to ischemia-reperfusion injury, with transient hypoperfusion inducing tissue hypoxia. Subsequent reperfusion exacerbates mucosal damage through oxidative stress and inflammatory cascades. Ischemic injury typically begins in the mucosal layer, the most vulnerable to hypoxia, and progresses to full-thickness necrosis within hours if ischemia persists. The susceptibility of the colon to ischemia is due to its relatively low baseline blood flow, limited microvascular density, and vulnerability of the vasa recta to vasospasm. Additionally, the reperfusion phase generates reactive oxygen species and activates inflammatory mediators, further exacerbating tissue injury [6].
While IC may be due to embolic events or underlying vascular lesions, transient and self-limited colonic hypoperfusion is a more common cause [5]. Regardless of the underlying etiology, the clinical spectrum ranges from reversible mucosal injury to transmural necrosis.
Managing IC complications depends on severity. Conservative measures remain the first-line approach in most cases, while transmural necrosis or perforation may require surgical resection [2]. In cases of severe hematochezia due to focal ulcer bleeding with major stigmata of recent hemorrhage, endoscopic hemostasis -particularly hemoclipping-is both effective and safe, especially in patients with bleeding diathesis or those on anticoagulation therapy [2]. However, hemoclipping may offer only transient hemostasis in ischemic ulcers, and rebleeding may occur. For patients with persistent or recurrent hemorrhage, radiologic interventions, such as superselective embolization, represent a viable alternative, facilitating targeted control of arterial bleeding while minimizing the risk of bowel ischemia.
While relatively uncommon, arterial bleeding in ischemic colitis is associated with increased risks of rebleeding, surgical intervention, and mortality. Recent studies report several risk factors for poor outcomes, including advanced age, chronic kidney disease, poor performance status, and right-sided colonic involvement. Among these, chronic kidney disease and higher Eastern Cooperative Oncology Group performance status scores are particularly associated with an increased risk of surgery or death [7]. These findings highlight the importance of early recognition and proactive management in patients at high risk.
As previously discussed, most patients recover with conservative management, typically including bowel rest, intravenous fluid resuscitation, and, when indicated, packed red blood cell transfusion. However, surgical intervention should be considered when conservative management fails, severe hematochezia persists, or hemodynamic instability develops [1]. This study shows that radiologic interventions may be employed as an alternative to surgery. Radiologic intervention should be considered in patients with persistent or recurrent arterial bleeding.
When performed with precision, superselective embolization using microcatheters and temporary embolic agents achieves effective hemostasis with a low risk of bowel infarction [8]. In our analysis, case 1 was classified as vascular occlusive IC, while cases 2 and 3 were identified as vascular non-occlusive IC. This differentiation was based on CT findings, serving as the primary imaging modality for classification in all three cases. These three cases indicate that radiologic intervention can serve as an effective treatment strategy for IC presenting with hematochezia. In vascular occlusive IC, stent placement may restore vascular patency (case 1). Conversely, in vascular non-occlusive IC, embolization can achieve hemostasis (cases 2 and 3).
All three cases presented with hematochezia associated with IC, confirmed by endoscopic evaluation. Studies characterize the endoscopic findings of IC, commonly including edematous and friable mucosa, ischemic ulceration, colonic wall necrosis, and interspersed pale areas. Additional endoscopic findings may include hemorrhagic nodules, segmental erythema with or without ulceration, and longitudinal linear ulcers [9,10]. Our case series is consistent with these established descriptions, as endoscopic evaluation revealed diffuse mucosal edema, erythema, ischemic ulcers, and interspersed pale areas, findings consistent with those of previous studies.
IC is conventionally not considered an indication for endoscopic intervention in managing gastrointestinal bleeding. However, in cases presenting with severe bleeding or endoscopic signs of recent hemorrhage within ischemic ulcers, endoscopic hemostasis should be considered. Among available endoscopic techniques, hemoclipping is the preferred modality, as it facilitates direct ligation of the underlying artery while minimizing tissue injury. Furthermore, hemoclipping is considered a relatively safe approach, even in patients with coagulopathies or those receiving anticoagulation therapy [2]. In this study, endoscopic hemostasis was initially attempted with hemoclipping in two cases (cases 2 and 3). However, in both cases, only transient hemostasis was achieved, and sustained hemostatic control was not maintained.
Beyond hemoclipping, thermal endoscopic hemostatic techniques, such as multipolar electrocoagulation and argon plasma coagulation, may be considered for patients with IC presenting with hematochezia. However, these modalities pose a relatively higher risk of ulceration and perforation due to excessive thermal injury and gas insufflation [2]. Owing to these potential complications, thermal techniques were not utilized in our cases.
Studies show that radiologic interventions, including angiographic embolization, may be effective in achieving hemostasis in patients with IC and hematochezia, particularly when bleeding persists despite endoscopic therapy [2,4]. In this study, radiologic intervention was performed in severe cases, yielding successful clinical outcomes. In contrast to previous studies, our case series specifically highlights severe presentations with radiologic intervention serving central in therapeutic management.
For IC presenting with hematochezia, angiography can be performed to identify vascular abnormalities, such as atherosclerosis or stenosis, before initiating radiologic intervention [11]. The presence of vascular stenosis on angiography supports a diagnosis of occlusive-type IC, with interventional procedures such as stent placement or angioplasty being appropriate. Conversely, when vascular stenosis is absent, non-occlusive IC is favored, and embolization may be considered as a therapeutic option. Embolization offers the advantage of achieving hemostasis for severe bleeding without requiring bowel preparation.
However, this approach has some inherent risk. In non-occlusive IC, with baseline perfusion already compromised, embolization may exacerbate ischemia or even lead to bowel infarction. Recent studies report a 1-4% incidence of bowel ischemia following embolization, highlighting the importance of careful superselective techniques to reduce these complications [12]. Techniques such as superselective catheterization and the use of temporary embolic agents, including Gelfoam, are recommended to preserve collateral circu-lation and minimize the risk of bowel infarction [8]. In this case series, this approach -specifically, microcatheter-guided Gelfoam embolization in cases 2 and 3-was performed without complications, supporting its safety in hemodynamically stable patients without evidence of transmural necrosis.
While some studies have investigated the role of angiography in managing IC [7], these findings suggest that, in cases of significant hematochezia, angiography followed by radiologic intervention may offer both diagnostic and therapeutic value.
Our findings suggest that radiologic intervention may serve as an effective rescue strategy in cases of IC complicated by significant arterial bleeding, particularly when conservative treatment and endoscopic hemostasis have failed. Angiography assists in identifying bleeding sources or vascular abnormalities requiring targeted embolization, and superselective embolization using microcatheters and Gelfoam achieves immediate hemostasis in select cases. However, given the few existing reports, further studies involving larger cohorts are necessary to better define the indications, safety, and efficacy of these interventions in this specific clinical context.
In conclusion, while IC is typically managed with conservative therapy, a subset of patients may experience severe arterial bleeding refractory to both medical and endoscopic interventions. In these cases, radiologic interventions, including superselective embolization and, when appropriate, arterial stent placement, offer effective, minimally invasive hemostasis. These interventions may serve as a viable alternative to surgery in appropriately selected patients. This approach is particularly valuable for individuals with advanced age, poor performance status, chronic kidney disease, or right-sided colonic involvement, factors associated with increased risk of adverse outcomes. Although concerns remain regarding the potential for bowel ischemia, improvements in embolization techniques and embolic materials have significantly reduced the incidence of serious complications. Our findings support radiologic intervention as a crucial rescue therapy for managing bleeding complications of IC. To better define its role in clinical practice, further prospective studies are needed to clarify indications, enhance safety, and assess long-term outcomes.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conception and design: Jun-young Seo.
Analysis and interpretation of the data: Jaehyung Park and Jun-young Seo.
Drafting of the article: Jaehyung Park and Jun-young Seo.
Critical revision of the article for intellectual content: Jae Woo Yeon, Jun-young Seo.
ACKNOWLEDGEMENTS
None.