위 저부 부속 간엽 내 초점성 결절성 과형성: 점막하 종양으로 오인된 증례
Focal Nodular Hyperplasia within an Accessory Liver Lobe Presenting as a Gastric Subepithelial Tumor: A Case Report
Article information
Trans Abstract
A 33-year-old man was referred for evaluation of a 4-cm subepithelial mass located in the gastric fundus, initially suspected to be a gastrointestinal stromal tumor based on endoscopic findings. Abdominal computed tomography revealed a well-enhancing mass along the gastric wall, with no apparent anatomical continuity with the liver. Endoscopic ultrasonography demonstrated a well-circumscribed, hypoechoic lesion confined to the serosal layer, suggesting an extramural origin. Subsequent magnetic resonance imaging showed arterial phase enhancement with persistent delayed enhancement and a central hypointense area characteristic of focal nodular hyperplasia (FNH). Laparoscopic resection was performed, and intraoperative indocyanine green fluorescence confirmed the hepatic origin of the mass. Histopathological analysis confirmed FNH arising from an accessory lobe of the liver. This case underscores the importance of recognizing the atypical presentations of hepatic lesions and highlights the diagnostic value of sequential imaging modalities for distinguishing hepatic tumors from gastric subepithelial lesions.
서 론
부속 간엽은 간 본체와 연결되어 존재하는 드문 선천성 기형으로 형태에 따라 stalk을 통해 연결된 경성(pedunculated type)과 넓은 기반을 가지는 무경성(sessile type)으로 구분된다. 부속 간엽은 대부분 무증상이며 영상 검사나 수술 중 우연히 발견되는 경우가 많다. 하지만 비전형적인 위치에 존재할 경우 인접 장기의 병변으로 오인될 수 있어 진단에 어려움을 초래한다. 초점성 결절성 과형성(focal nodular hyperplasia, FNH)은 간에서 흔히 발견되는 양성 종양으로 전형적인 영상 소견(중심성 반흔과 방사형 혈관)을 통해 진단이 가능하지만 부속 간엽 내 발생은 극히 드물어 감별이 어려울 수 있다[3,4].
증 례
33세 남자 환자가 건강 검진을 위하여 타 병원에서 시행한 상부위장관 내시경 검사에서 위 저부(fundus)에 위치한 약 4 cm 크기의 점막하 종괴가 발견되었고 이후 정밀 평가를 위하여 본원으로 의뢰되었다. 환자는 보고된 가족력이나 과거 질환은 없었으며 내원 시 시행한 신체 검사, 일반 혈액 검사 및 생화학 검사 결과 모두 정상 소견을 보였다. 내시경 소견상 병변은 정상 점막으로 피복되어 있었으며 육안상 특징이 명확하지 않아 점막하 병변으로 판단되었다(Fig. 1). 일반적으로 위저부에 발생하는 점막하 병변은 위장관 기질 종양(gastrointestinal stromal tumor, GIST), 평활근종, 외부 압박 등이 주요 감별 대상이다. 본 증례에서는 병변이 내강 쪽으로 융기되어 있어 내재성 병변 가능성이 우선 고려되었다.
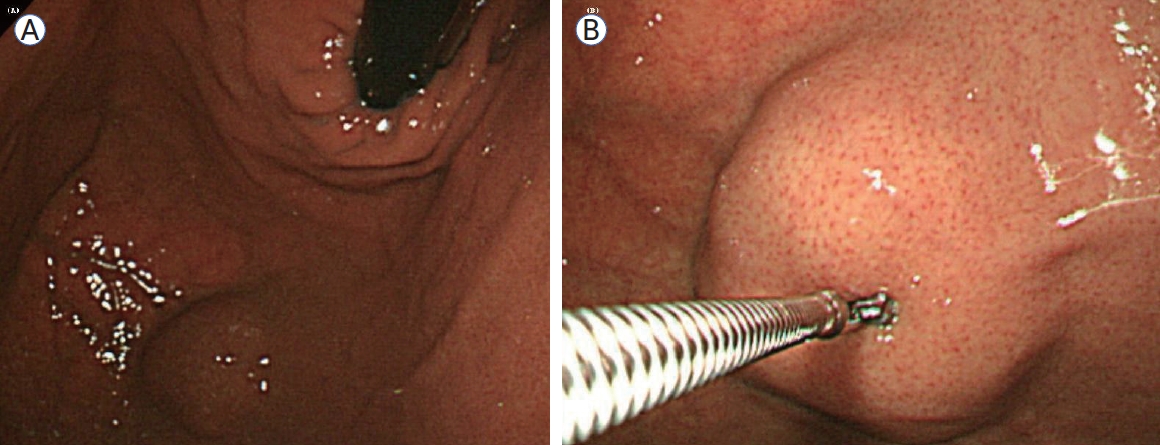
Endoscopic findings. A subepithelial lesion with intact overlying mucosa at the gastric fundus (A) and a biopsy showing a visible vascular pattern (B).
복부 조영증강 전산화단층촬영(computed tomography, CT)에서는 병변이 위 저부에 국한되어 조영증강되었고(Fig. 2) 인접한 간과의 해부학적 연속성이 관찰되지 않아 초기에는 위벽 기원 병변으로 추정되었다. 일반적으로 부속 간엽의 경우 stalk이 관찰되거나 간과의 연속성이 시사되나[2] 본 증례에서는 CT상 명확히 구별되지 않았다.
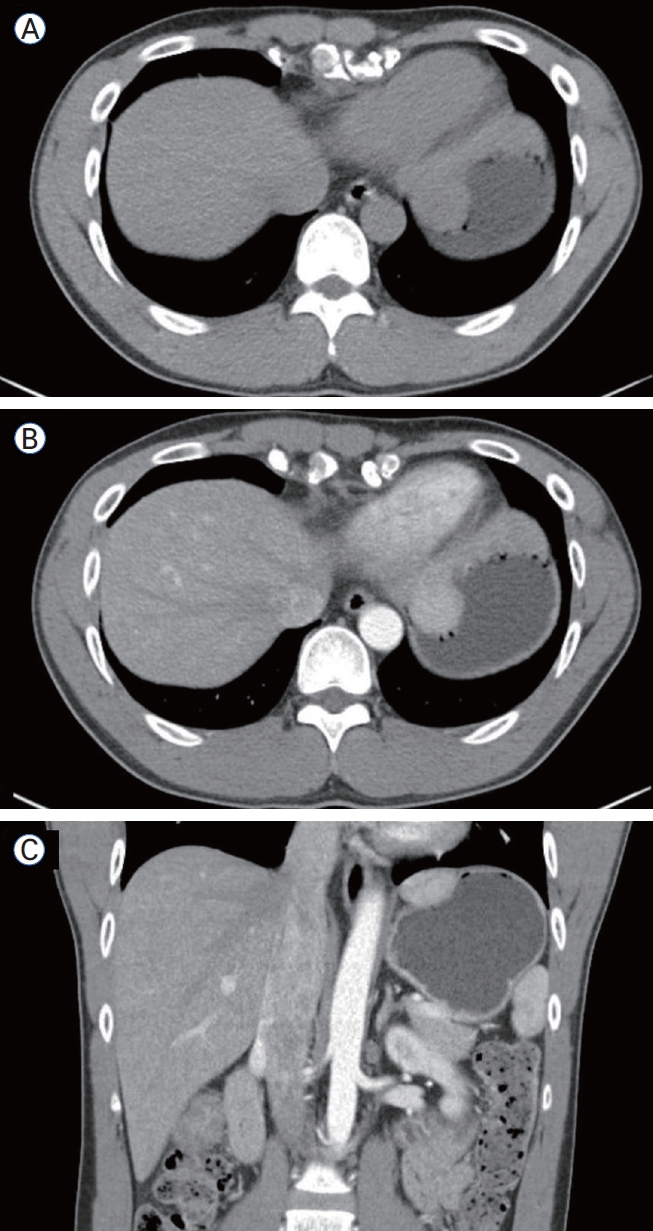
Abdominal CT findings. Low-attenuation lesion at the gastric fundus on pre-contrast axial view (A), showing enhancement on contrast-enhanced axial and coronal views (B, C). CT, computed tomography.
내시경 초음파(endoscopic ultrasound, EUS)에서 병변은 serosa layer에 국한된 균일한 저에코성(hypoechoic) 병변으로 관찰되었으며 muscularis propria와는 명확히 구분되어 있어 위장관벽 기원보다는 외부 기원의 가능성을 고려하게 하였다(Fig. 3). 그러나 종괴의 실제 기원층이 확정되지 않아 조직학적 판단 또는 영상학적 추가 평가가 필요하다고 판단되었다.
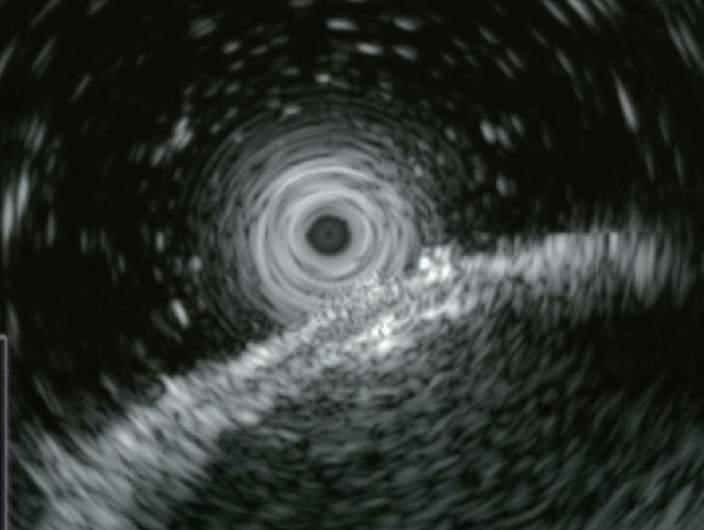
Endoscopic ultrasonography. A homogeneous hypoechoic mass confined to the serosal layer without clear layer of origin.
간 자기공명영상(magnetic resonance imaging, MRI)을 시행한 결과 병변은 arterial phase에서 조영증강되고 delayed phase에서 중심성 반흔을 시사하는 저신호 영역이 관찰되었는데, 이는 FNH의 전형적인 영상 소견과 일치하였다. 이러한 소견은 병변의 간 유래 가능성을 강력히 시사하였다(Fig. 4).
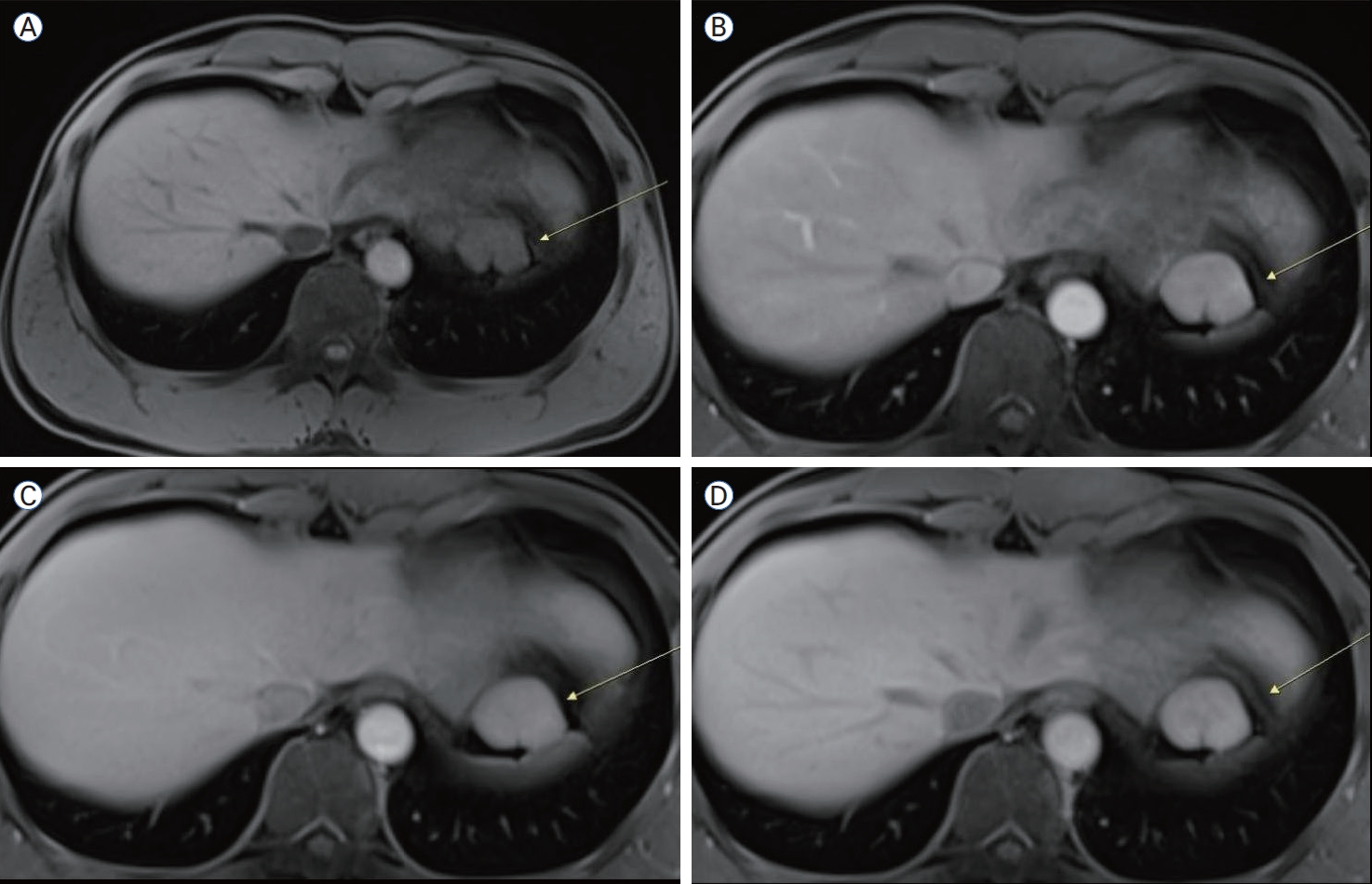
Liver MRI findings. Pre-contrast T1 image showing low-signal (A), arterial (B), venous (C), and delayed-phase (D) images demonstrating progressive enhancement and a central scar (yellow arrows). MRI, magnetic resonance imaging.
복강경 수술을 통해 확인한 병변은 위 저부의 장막면에서 외측으로 돌출되어 있었고 stalk을 통해 고정된 구조였다(Fig. 5). 육안으로 병변의 간 조직 여부를 명확히 확인하기 어려웠기 때 문에 실시간 indocyaine green (ICG) 형광조영을 이용하여 간 유래 조직임을 확인하였고 이후 절제를 시행하였다. 병리 조직 검사에서는 소엽성 간세포 배열, 중심성 반흔, 담관 증식 등의 소견이 확인되었으며(Fig. 6) 이는 FNH의 전형적인 조직학적 특징과 부합하였다.

Intraoperative and indocyanine green (ICG) findings. Laparoscopic view showing a pedunculated lesion from the gastric fundus (A) and fluorescence under ICG, indicating a hepatic origin (B).

Gross and histopathologic f indings. Gross specimen with encapsulated nodular appearance (A), cut surface showing a central stellate scar characteristic of focal nodular hyperplasia (B), low-power histological view (H&E, × 40) demonstrating a central fibrous scar with radiating fibrous septa (C), and high-power histological view (H&E, × 100) showing ductular reactions and thick-walled blood vessels within the fibrous septa, consistent with FNH features (D). H&E, hematoxylin and eosin; FNH, focal nodular hyperplasia.
고 찰
이소성 간(ectopic liver)은 본 간과 해부학적, 혈관학적 연속성이 없는 간 조직이 복강 내 이소 부위에 존재하는 드문 기형이다. 가장 흔한 위치는 담낭이며 위, 장간막, 비장 주위 등에서도 보고된 바 있다[1]. 이소성 간은 대부분 무증상이며 영상 검사 또는 수술 중 우연히 발견되지만 해부학적 구조가 비전형적이기 때문에 종종 인접 장기의 병변으로 오인될 수 있다. 특히 위장관 점막하 종양과 구별이 어려운 경우가 많아 임상가의 높은 인지도가 요구된다.
FNH는 간에서 비교적 흔히 발견되는 양성 종양으로, 혈류 이상에 반응한 간세포의 과형성으로 알려져 있다. 일반적으로 간 내에서 발견되며 중심성 반흔, 균일한 간세포 판, 담관 증식 등의 병리학적 특징과 함께 간 MRI에서의 전형적인 영상 소견(arterial phase에서 조영증강, delayed phase에서 조영 유지 및 중심성 저신호 영역)을 통해 진단이 가능하다. 그러나 이러한 FNH가 부속 간엽이나 이소성 간에서 발생하는 경우는 극히 드물며 전형적 소견이 명확하지 않은 위치에서는 감별이 어려워진다[2].
본 증례에서는 영상학적 소견과 위치적 특이성으로 인하여 GIST 또는 평활근종으로 오인될 가능성이 있었으며 실제 CT 및 내시경 소견상에서는 위벽 기원 병변으로 추정되었다. 그러나 EUS와 MRI에서 점차 간 조직과 유사한 특성을 확인할 수 있었고 ICG 형광조영의 보조적 사 용은 수술 중 간 조직임을 실시간으로 확인하는 데 결정적 역할을 하였다. 병리학적으로 FNH의 조직학적 특징이 명확히 확인되어 최종 진단에 도달할 수 있었다.
따라서 위장관에서 비전형적으로 관찰되는 점막하 종괴를 평가할 때에는 이소성 간 또는 부속 간엽 기원의 병변도 반드시 감별 진단에 포함되어야 하며 영상 진단의 한계가 있는 경우 수술 중 ICG 조영제 활용이 진단적 정확성을 높이는 데 유용할 수 있다.
본 증례는 위 저부 점막하 종양으로 오인된 부속 간엽 내 FNH의 드문 사례로 위장관 점막하 종괴 감별 시 간 유래 병변 가능성을 반드시 고려해야 함을 시사한다.
부속 간엽은 본 간과 해부학적으로 연결되어 존재하는 드문 선천성 기형으로 형태에 따라 경성(pedunculated type)과 무경성(sessile type)으로 구분된다. 경성은 얇은 stalk을 통해 간과 연결되며 무경성은 넓은 기반으로 부착되어 있다. FNH는 간에서 비교적 흔히 발견되는 양성 병변이지만 부속 간엽내 발생은 극히 드물다. 본 증례는 건강 검진 중 시행한 상부위장관 내시경 검사에서 위 저부에 발견된 4 cm 크기의 점막하 종괴를 주소로 내원한 33세 남성 환자에 대한 보고이다. EUS에서는 정상 점막 아래로 종괴가 관찰되었고 복부 CT와 MRI에서는 위 저부에 경계가 명확한 조영증강 병변이 확인되어 간 유래가 의심되었다. 복강경 절제술 중 stalk을 가진 부속 간엽이 확인되었고 병리 조직 검사 결과 FNH로 확진되었다. 본 증례는 위 점막하 종괴로 오인될 수 있는 부속 간엽 내 FNH의 드문 사례로 위장 내 비전형적 종괴 평가 시 간 유래 병변 가능성을 고려해야 함을 시사한다.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
None.
AUTHOR CONTRIBUTIONS
June Kim: Conceptualization, Data curation, Investigation, Writing.
Dong Hyun Lee: Conceptualization - review & editing, Supervision, Project administration.
All authors have shared responsibility for the final version of the manuscript.
ACKNOWLEDGEMENTS
None.