수년간 지속된 요통을 호소하는 22세 여자
A 22-year-old Woman with Chronic Back Pain
Article information
Trans Abstract
Low back pain, categorized as nociceptive, neuropathic, or nociplastic, is the leading cause of disability in terms of years lived among young people. The lumbar spine may produce specific or non-specific pain. Treatment depends on the underlying cause of low back pain. This review discusses the classification, prevalence, diagnosis, and treatment of low back pain in young adults.
22세 여자가 수년간 지속된 저리는 양상의 요통이 있다고 하였다. 1개월 전 외상 없이 앉아 있는 상태에서 허리와 함께 우측 하지로 방사통이 발생하였고, 가만히 있거나 허리를 숙일 때 악화되고 움직이면 호전된다고 하였다. 허리에서부터 우측 엉덩이로 통증이 내려오고 우측 무릎 전면부, 발목 앞뒤가 저리듯이 통증이 발생한다고 하였다. 하지직거상 검사(straight leg raise test), FABER test, distraction test 결과 우측에서 통증이 있었고 요추 부위 압통은 없었지만 L3/4, L4/5 후관절, 우측 천장관절, 우측 이상근에서 압통이 있었다. 하지의 운동감각신경 저하는 없었다. 염증성 요통을 감별하기 위해 시행한 검사에서 적혈구침강속도 3 mm/h (정상 범위: 0-20 mm/h), C-반응단백질 0.03 mg/dL (정상 범위: 0.01-0.3 mg/dL), HLA-B27 음성으로 확인되었고 영상 검사로 X-ray, 척추 컴퓨터단층촬영(computed tomography, CT), 자기공명영상(magnetic resonance imaging, MRI)을 순차적으로 시행하였다.
임상경과
CT에서 L4-5 추간판팽륜(disc bulging)과 우측 천장관절에 부분적으로 연골하 불규칙적인 모양이 관찰되었고(Fig. 1), MRI에서는 L4-5 척추사이구멍으로 머리쪽으로 이동한 추간판탈출과 L4 신경뿌리가 척추신경공으로 전위되어 있었으며 우측 천장관절의 부분적인 연골하 골수부종이 확인되었다(Fig. 2). 비스테로이드 소염제와 근이완제에 효과가 없어 마취통증의학과에 의뢰하여 L4 경신경공 경막외주사(transforaminal epidural injection)와 우측 천장관절 차단술을 시행 후 요통이 호전되었다. 상기 환자는 젊은 나이, 만성 요통 양상, 일측성 천장관절염 소견이 동반되어 있었으나, 임상증상/치료 경과(NSAID non-response)/혈액 검사 결과를 종합하여 강직성척추염이 아닌 추간판 탈출과 이로 인한 신경뿌리 통증으로 진단되었다.
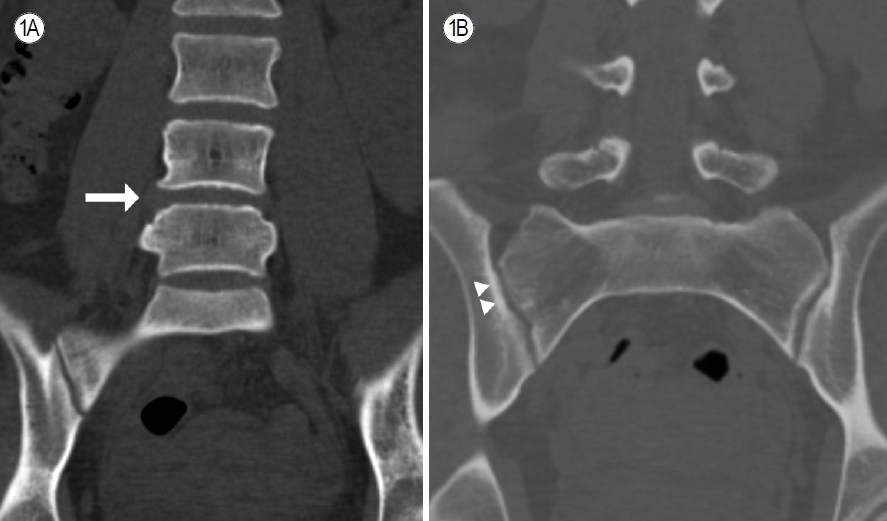
Computed tomography of the spine and sacroiliac joint. (A) Disc bulge between L4 and 5 (arrow) and (B) localized subchondral irregularity of the right sacroiliac joint (arrowheads).
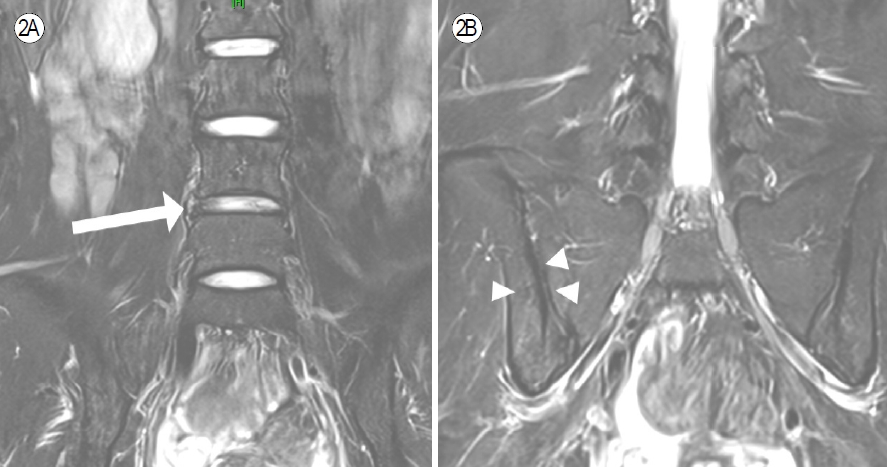
T2-weighted magnetic resonance imaging of the spine and sacroiliac joint. (A) Disc extrusion (arrow) in the right foraminal zone and cranial migration at L4-5 and (B) localized subchondral bone marrow edema (arrowheads) in the right sacroiliac joint, suggestive of sacroiliitis.
서 론
요통은 해부학적으로 12번 갈비뼈부터 엉덩뼈능선(iliac crest)까지의 범위에서 발생하는 통증으로 종종 둔부 통증이 동반되기도 하지만 둔부 통증은 해부학적으로 엉덩뼈능선에서 엉덩이주름(gluteal fold)까지의 부위를 말한다. 요통은 통각 통증(nociceptive pain), 신경병 통증(neuropathic pain) 그리고 통각가소성 통증(nociplastic pain)의 양상으로 나타난다[1]. 1년간 요통의 유병률은 높게는 80%까지 나타나며, 20세가 되기 전까지 39%에서 발병하는 것으로 확인되었다[2,3]. Jhun과 Park [4]은 제4회 대한민국 국민건강영양조사 분석 결과에서 2007년 대한민국 성인의 18.4%가 요통 증상이 있었고 5.4%에선 만성적인 양상을 보인다고 하였다. 본고에선 높은 유병률과 신체 장애의 주요 원인이 되는 젊은 사람에서 발생하는 요통의 종류와 영상 검사 및 치료에 대해서 살펴보았다. 요통의 분류는 이전 논문들을 참고하여 부위별로 나누었고 도표로 정리하였다(Fig. 3).
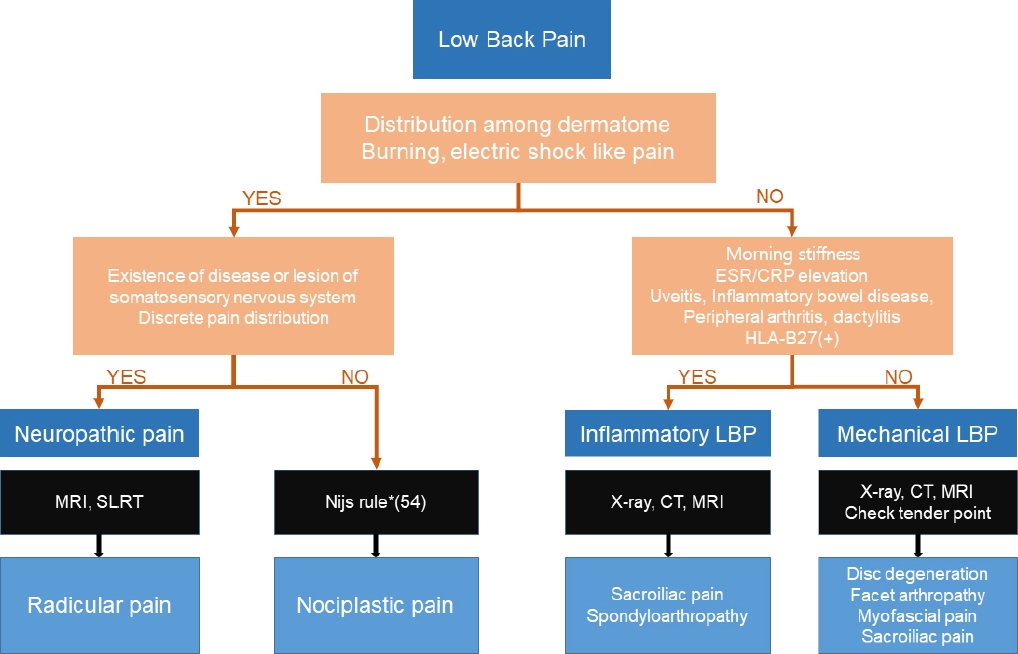
Diagnosis of LBP. Based on the Nijs rule, LBP is diagnosed if the following three criteria are present. First, pain is disproportionate to the nature and extent of injury or pathology. Second, pain is diffuse; allodynia and hyperalgesia are present. Third, there is hypersensitivity to stimuli unrelated to the musculoskeletal system. ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; HLA-B27, human leukocyte antigen-B27; MRI, magnetic resonance image; SLRT, straight leg raising test; CT, computed tomography; LBP, low back pain. *Nijs rule: 1) pain experience disproportionate to the nature and extent of injury or pathology, 2) diffuse pain distribution, allodynia, and hyperalgesia, 3) hypersensitivity of senses unrelated to the musculoskeletal system.
본 론
분류 및 진단
추간판 변성(disc degeneration)
추간판 변성은 수핵(nucleus pulposus), 섬유륜(annulus fibrosus) 그리고 연골성 종말판(cartilaginous endplate)의 변화와 연관되어 있다. 추간판은 외부 압력에 대항하여 수핵으로부터 오는 방사형 압력과 섬유륜의 저항하는 인장 강도로 팽팽하게 유지되어 있다. 만약 추간판 내 압력이 소실된다면 섬유륜은 안팎으로 튀어나오거나 휘게 된다. 추간판 변성이 되면 종말판에 손상이 생기고 연골하골의 경화(sclerosis)가 나타난다. MRI 검사 시행 시 확인된 추간판 변성의 유병률은 운동선수가 아닌 젊은 사람(중간값 26세, 16-28세)에서 30-53.8%, 젊은 운동선수(중간값 28세, 18-30세)에선 81.5-100%로 요통의 유무와 상관없이 상당히 높은 것으로 확인되었다[5,6]. 영상 검사로는 방사선 검사가 가장 먼저 시행되며, CT는 후방 골증식을 평가하여 수술 계획을 세울 때 유용하고, MRI는 추간판의 높이나 형태의 변화를 보며 Pfirrmann grading을 시행할 수 있어 진단 시 gold standard 검사이다[7].
신경뿌리 통증(radicular pain)
신경뿌리 통증은 척수신경의 감각신경뿌리 혹은 뒤뿌리 신경절의 기계적인 자극이나 염증 매개 물질에 의하여 발생하는 통증으로 정의되나, 피부 분절로 분포하거나 모호한 여러 임상적인 특징을 갖는, 주관적으로 묘사되는 것을 칭하기도 한다. 젊은 사람에서의 유병률은 평균 나이 25세에서 2% 정도로 확인되었다[8]. 젊은 사람에서 좌골신경통은 35-55세에 가장 많이 나타나고 가장 흔한 원인은 95%에서 나타나는 요추간판탈출증이다[9]. 하지직거상 검사는 신뢰성 있는 검사로 시행이 권고되고 있고 MRI는 환자의 임상 증상과 연관된 신경병증을 평가하는 데 사용할 수 있다.
후관절병증(facet arthropathy)
후관절은 추간판과 함께 척추를 지지하고 안정화하며 모든 방면으로의 과도한 움직임을 제한함으로써 부상을 방지하는 기능을 한다. 40세 미만에서의 grade 2 이상의 후관절병증의 유병률은 요통이 있을 때 4%이고, 요통이 없을 때 6%로 확인되었다[10]. CT와 MRI를 활용하여 후관절의 변화를 확인할 수 있다. 후관절은 두 레벨의 척수신경의 뒤가지(dorsal ramus)의 내측가지(medial branch)에서 신경이 들어오기 때문에 진단과 치료를 위해 내측지신경차단술(medial nerve branch block)이나 후관절주사(Facet joint injection)를 시행할 수 있다.
근막 통증(myofascial pain)
등근육은 여러갈래근(multifidus), 가장긴근(longissimus), 가시근(spinalis) 및 엉덩갈비근(iliocostalis)으로 이루어져 있으며 통증의 부위가 된다. 허리 근막통증의 유병률은 평균 나이 43.6세에서 증상이 없을 때 1.9%, 허리엉치 신경뿌리병증이 있을 때 76.4%에서 엉덩이에 압통점이 확인되었다[11]. 근막통증은 여러 진단 기준들이 제시되어 있는데, 그중 4가지 진단기준이 가장 흔하게 사용되고 있다: 1) 근육의 taut band에서의 압통점, 2) 압통 부위 촉진 시 환자의 통증 지각, 3) 압통 부위 촉진 시 예상되는 통증의 분포, 4) 국소 경련(twitch) 반응[12].
천장관절통(sacroiliac joint pain)
천장관절통은 허리 통증의 14.5% 정도를 차지한다고 보고되었다[13]. 천장관절통 유발 검사들의 타당성과 신뢰도를 비교한 연구에서 천장관절통이 있는 경우에 양성으로 확인되는 검사 순서는 FABER test (91.5%), compression test (78.7%), posterior shear test (71.8%), sacral thrust test (72.0%), distraction test (68.4%) 그리고 Gaenslen test (56.4%) 순으로 확인되었다[14]. 진단을 위한 영상 검사로는 X-ray, CT, MRI가 사용되며 MRI가 골수부종와 염증을 신뢰성 있게 확인할 수 있는 검사이고 저선량 CT 또한 MRI보다는 정확도가 떨어지지만 미란과 관절유착을 확인하는 데 사용할 수 있으며 경화에서는 유의미한 차이 없이 X-ray가 MRI보다 우세하였다.
척추관절병증(spondyloarthropathies)
척추관절염의 유병률은 세계적으로 20-30세에서 0.16%, 30-40세에서 0.34%로 확인된다. 대표적인 질환은 강직성척추염으로 한국에서의 유병률은 2015년 10만 명당 52명으로 추산되었고, 해마다 증가하는 추세이다[15,16]. 척추관절병증은 염증성 관절염으로 혈액 검사에서 erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) 등의 급성기 반응 물질이 상승하고, 30분 이상 지속되는 조조강직감을 특징으로 한다. 또한 관절 증상 외에도 포도막염, 건선, 염증성 장질환이 동반될 수 있고, 관절 주위 증상으로 손발가락염(dactylitis), 부착부염(enthesitis)이 발생할 수 있다. 강직성척추염 외에도 반응관절염, 건선관절염, 염증성 장질환 연관 척추염 및 미분화 척추관절염이 있으며 HLA-B27 양성과 연관이 있다[17]. MRI는 골수부종와 염증을 관찰하여 조기 진단에 유용하며 CT는 미란, 경화성 변화나 뼈의 구조적 변화를 평가하는 데 민감도가 높다.
통각가소성 통증(nociplastic pain)
통각가소성 통증은 외부 자극이나 유해 자극으로 인한 통증인 통각 통증이나 원발 부위나 질병에 의해 말초 체성감각계로 유발되는 신경병 통증과는 구별되는 통증으로 제안되었다[18,19]. 원인이 불분명한 요통은 최대 85% 정도까지 확인되었다. 요통의 중추 감작은 뇌의 신경적응 변화로 뇌피질의 활성이 증가하거나 같은 압력에도 더 심한 통증과 기능성 MRI (functional MRI)에서 통증으로 유발되는 신경 활성이 더 광범위한 패턴으로 나타나거나 더 약한 자극에도 비슷한 강도의 신경 활성에 의한 것으로 지속적인 통각 자극이 요통의 중추 감작을 일으키는 것으로 보인다. Nijs rule이 중추 감작을 진단하는 데 사용될 수 있다[20]: 1) 손상과 병리와 일치하지 않는 통증 경험, 2) 미만성 통증 분포, 이질통 및 통각 과민, 3) 근골격계와 관련 없는 감각 과민증. 아직 명확한 진단 기준은 없으나 Nijs rule은 통각가소성 통증에 대한 안면 타당도가 있다[19,21].
치 료
약물 치료
American college of physician에 의한 요통의 가이드라인은 급성과 아급성 요통의 경우 비약물적 요법에 효과가 없다면 비스테로이드소염제와 근이완제를 환자의 선호도에 따라 먼저 시작해 보는 것을 추천하였다[22]. 만성 요통의 경우 비약물적 요법에 효과가 없다면 초기 치료로 비스테로이드소염제를 사용하고 두 번째로 tramadol이나 duloxetine을 고려해볼 수 있다고 하였다. 아편유사진통제와 항우울제 중 duloxetine을 사용해 볼 수 있다. 좌골신경통의 경우 다이아제팜을 사용해 볼 수 있으며 척추관절염은 첫 번째로 비스테로이드 소염제 및 설파살라진과 같은 질환조절항류마티스약제를 사용하는 것이 권고된다. 이러한 약물 치료에 적절한 치료 효과가 없을 경우 tumor necrosis factor (TNF) inhibitor, interleukin-17 (IL-17) inhibitor, 또는 Janus kinase inhibitor를 사용하는 것이 권고된다.
비수술 치료
결 론
요통은 나이가 들수록 유병률이 증가하고 대다수의 사람들이 겪는 증상이며 신체 장애의 가장 중요한 원인으로 상당수에서 만성 통증이 되어 삶의 질을 감소시킨다. 요통의 원인은 한 가지로 국한되지 않고 여러 부위가 혼합되어 나타나는 경우가 많기 때문에 진단을 위해 다각적으로 접근하고 치료 시에도 다각적인 치료를 시도해야 한다. 특히 젊은 나이에 발생한 요통은 기계적 원인이나 신경 관련 통증뿐만 아니라 척추관절염과 같은 염증성 요통의 가능성까지 고려하여 진단 및 치료를 하는 것이 중요하다.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conception and design: SHK, HKM; Drafting of the manuscript: SHK; Critical revision for intellectual contents: HKM, SHL, HRK; Final approval of the manuscript: all authors.