원발성 췌장 점막 연관 림프조직 림프종
Primary Lymphoma of Pancreatic Mucosa-Associated Lymphoid Tissue (MALT)
Article information
Abstract
원발성 췌장 림프종은 췌장 종양 중에서 매우 드문 질환이다. 원발성 췌장 림프종의 치료는 대부분 외과적 수술보다는 항암 치료 또는 방사선 치료를 먼저 시행하므로 췌장에 발생하는 다른 종양과의 감별진단이 중요하다. 또한 본 증례와 같이 림프종 중에서도 조직 아형에 따라 치료 원칙이 차이가 있을 수 있으므로 정확한 조직 진단이 치료 방침을 결정하는 데 중요하다. 저자들은 췌장 두부 종양에서 초음파 내시경 유도하에 중심부 바늘 조직 검사를 시행해서 국내에서 처음으로 원발성 췌장 MALT 림프종을 진단하였기에 이를 보고한다.
Trans Abstract
Primary lymphoma of pancreatic mucosa-associated lymphoid tissue (MALT) is extremely rare. Initial suspicion of primary pancreatic lymphoma is hampered by its low incidence. However, it should always be included in a differential diagnosis of pancreatic mass with unusual features, because an accurate diagnosis can avoid unnecessary surgical intervention. A 70-year-old woman presented with melena associated with a mass on the pancreatic head. Endoscopic ultrasonography-guided core-needle biopsy of the pancreatic mass revealed MALT lymphoma. The patient is currently undergoing radiation therapy. We present a case of primary lymphoma of the pancreatic MALT with a review of the literature.
서 론
췌장에서 원발성으로 발생한 림프종은 매우 드물어서, 전체 림프종의 0.6%에 불과한 것으로 알려져 있다. 또한, 췌장의 림프종은 췌장의 악성 종양 중에서도 드물어, 전체 췌장 악성 종양의 약 4.9% 정도를 차지하는 것으로 알려져 있다[1]. 원발성 췌장 림프종은 일반적인 췌선암이나 췌장염과 종종 임상 증상과 영상 소견이 비슷하여 감별이 어려울 수 있다. 그러나 원발성 췌장 림프종은 이들 병변과 비교할 때, 치료와 예후에 차이가 있어 감별 진단이 중요하다.
점막 연관 림프조직(mucosa-associated lymphoid tissue, MALT) 림프종은 림프절이 아닌 점막조직이 만성적인 염증이나 감염으로 인하여 지속적으로 항원에 노출되어 림프구 증식이 일어나는 것으로, 이로 인하여 유전자가 비가역적으로 재배열됨으로써 발생하게 된다. 점막 연관 림프조직 림프종은 점막조직이 존재하는 대부분의 장기에서 발생할 수 있으며 발생 장기는 위에서 가장 많이 발생하고 침샘, 안와 부속기, 피부, 폐, 소장 등이 흔히 발생하는 장기로 알려져 있다. 원발성 췌장 MALT 림프종은 저자들이 문헌 고찰한 바로는 현재까지 세계적으로 일본에서만 3예가 보고되었고[2-4], 국내에서는 아직 보고된 적이 없는 매우 드문 질환이다. 저자들은 췌장 두부에서 기원한 MALT 림프종 증례 1예를 경험하였기에 문헌 고찰과 함께 보고하는 바이다.
증 례
70세 여자가 흑색변으로 연고지 병원을 방문하였다. 환자는 상기 증상으로 상부위장관 내시경 검사를 시행받았다. 그 결과 십이지장 구부에서 점막의 뚜렷한 이상 소견 없이 십이지장 내강으로 외부에서 밀고 들어오는 양상의 종괴성 병변이 관찰되었다(Fig. 1). 이 병변의 일부 점막 함몰 부위에서 출혈이 관찰되어 내시경 클립으로 지혈하였다. 당시 타원에서 촬영한 복부 컴퓨터단층촬영(computed tomography, CT)에서 췌장 두부에 장경 약 6 cm 크기의 종양이 관찰되었다. 이 종양은 조영 증강 시 동맥기에서 정상 췌장 실질보다 불균질한 저음영을 보이고 지연기로 갈수록 조영 증강을 보였다(Fig. 2A and 2B). 췌장 두부에 위치한 총담관은 종양에 의하여 둘러 싸여 있었고, 추적 가능한 정도로 좁아져 있었으나 간내 담관 확장은 동반되지 않았다(Fig. 2C). 환자는 추가 검사 및 치료를 위하여 전원되었다.
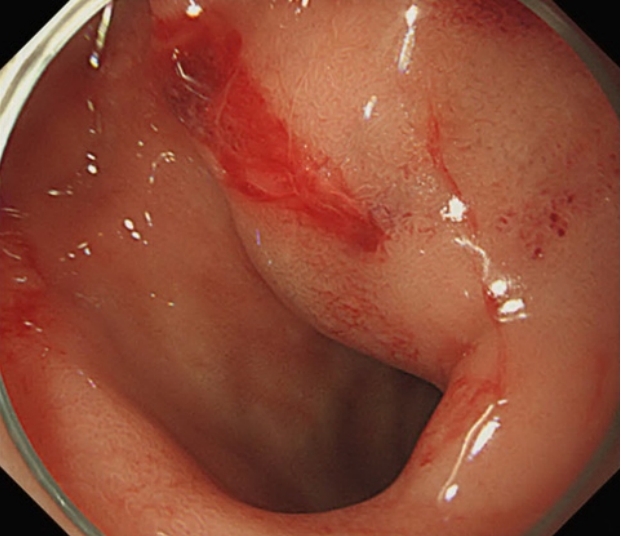
Duodenoscopic findings. A mass with a smooth margin and a normal-looking overlying mucosa that was bulging into the lumen was noted in the duodenal bulb. Blood oozing was noted from a small dimple on the surface of the mass.

Abdominal computed tomography (CT) findings. (A) Arterial-phase CT image showing a 6 cm, ill-defined, heterogenous, low-attenuation mass (arrow) and a unilocular cystic lesion (arrowhead) on the pancreatic head. (B) Portal venous-phase CT image showing an iso-attenuating mass (arrow) on the pancreatic head, indicating delayed enhancement. (C) Coronal CT image showing a smoothly stenotic common bile duct (arrowhead), not associated with dilatation of the intrahepatic duct.
환자는 과거력에서 고혈압 이외에는 특이 병력이 없었으며, 음주력 및 흡연력은 없었다. 내원 당시 활력 징후는 혈압 105/72 mmHg, 심박수 70/분, 호흡수 18/분, 체온 36.5℃였고, 체중 67 kg, 신장 160 cm였다. 환자가 호소하는 증상은 없었고, 신체 진찰에서 특이 소견은 없었다.
내원 당시 혈액 검사에서 백혈구 5,000/mm3;, 혈색소 14.2 g/dL, 혈소판 293,000/mm3이었다. 생화학 검사에서 아스파르테이트아미노전달효소 20 U/L, 알라닌아미노전달효소 14 U/L, 알칼라인산분해효소 89 U/L, 총 빌리루빈 0.4 mg/dL였다. 아밀라아제는 83 U/L, 리파아제는 32 U/L였다. 종양표지자는 carbohydrate antigen (CA) 19-9 3.5 U/mL, carcinoembryonic antigen (CEA) 1.4 ng/mL로 정상이었다. 혈청 면역글로불린 G (immunoglobulin G, IgG) 및 G4 (IgG4)는 각각 1,120 mg/dL (700-1,600 mg/dL), 36 mg/dL (<140 mg/dL)였다.
입원하여 시행한 자기공명담췌관조영 검사(magnetic resonance cholangiopancreatography, MRCP)에서 췌장 두부 종양을 관통하는 주췌관이 잘 관찰되었다. 종양의 상류쪽 주췌관 확장을 동반하지 않았으며 주췌관 협착이 관찰되지 않았다(Fig. 3A). 이와 함께 시행한 F-18 fludeoxyglucose 양전자방출단층촬영(positron emission tomography, PET)에서는 췌장 두부의 standardized uptake value (SUV) 6.3의 고대사성(hypermetabolic) 병변이 관찰되었으며 다른 곳의 병변은 관찰되지 않았다(Fig. 3B).
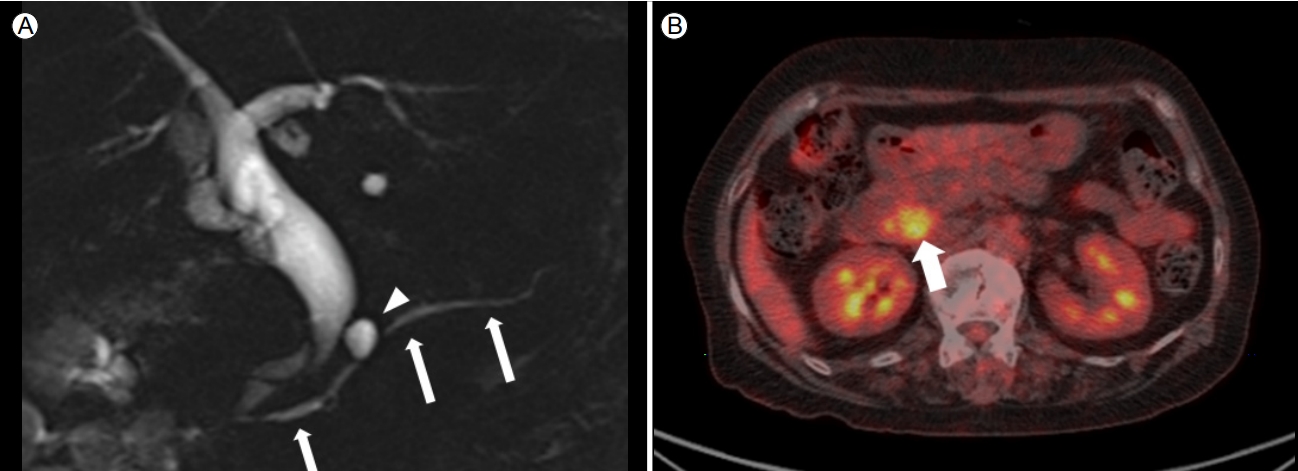
Magnetic resonance cholangiopancreatography (MRCP) and F-18 fludeoxyglucose positron emission tomography findings. (A) Main pancreatic duct clearly visible on MRCP (arrows) without irregular narrowing. Pancreatic duct penetrates through the pancreatic mass. A unilocular pancreatic cyst (arrowhead) detected by computed tomography. (B) Positron emission tomography showing hypermetabolism (SUVmax, 6.3) of the mass (arrow) on the pancreatic head.
내시경 초음파(endoscopic ultrasonography, EUS)를 시행해서 종양의 대부분이 췌장 두부에 위치함을 확인하였고, 췌장 두부에 저에코성 종양을 관찰할 수 있었다. 췌장 두부 종양 병변에서 EUS 유도하에 22G 바늘(AcquireTM, Boston Scientific Korea, Seoul, Korea)로 중심부 바늘생검을 시행하였다(Fig. 4).
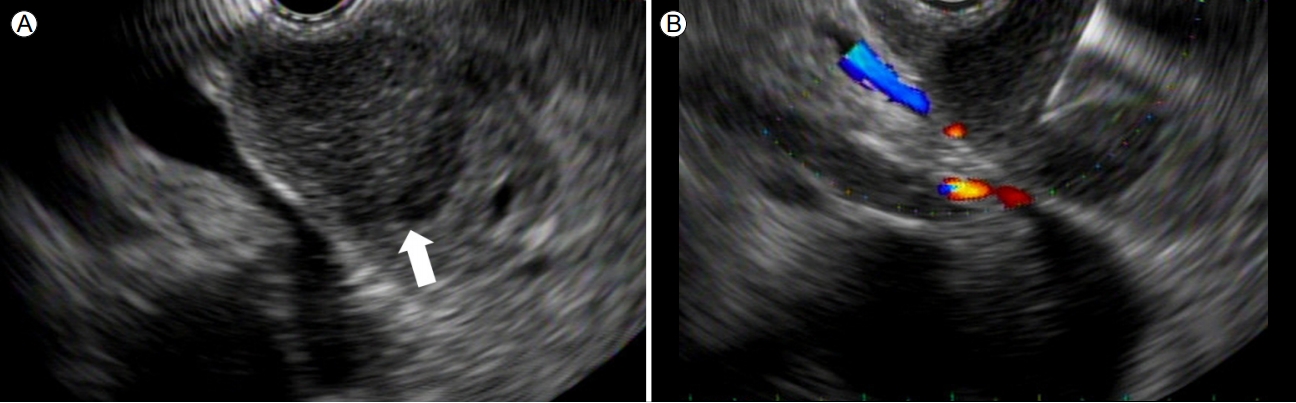
Endoscopic ultrasonographic findings. (A) A relatively well-defined hypoechoic mass (arrow) at the pancreatic head. (B) Endoscopic ultrasonography-guided core needle biopsy using a 22 G core-biopsy needle (AcquireTM, Boston Scientific Korea, Seoul, Korea).
병리 소견상 림프구의 증식이 관찰되며 림프 표재성 병변이 확인되었다(Fig. 5A). 이 림프세포들은 면역조직화학염색 결과 CD20 (+), Bcl2 (+), CD3 (-), CD5 (-), CD10 (-), Bcl6 (-) 소견을 보여, 변연부 B세포 림프종임을 확인할 수 있었다(Fig. 5B-E). Ki-67은 10% 미만으로 확인되어, 저등급 B세포 림프종 소견을 보였다(Fig. 5F). IgG4 면역화학염색에서 양성인 형질구는 관찰이 되지 않았다. 이상의 소견을 종합하여 췌장의 종양은 림프절 외 변연부 B세포 MALT 림프종으로 진단을 내릴 수 있었다.
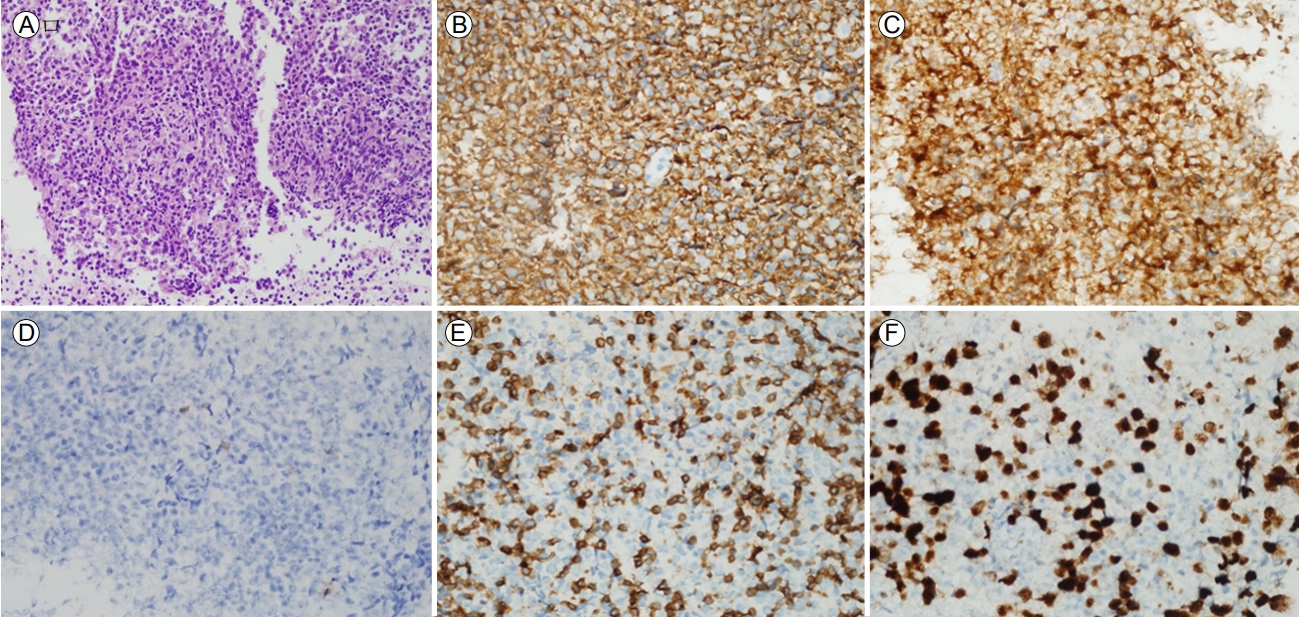
Histopathology and immunohistochemistry findings of the pancreas. (A) A dense and monotonous population of centrocyte-like cells with residual germinal centers (HE, ×200). (B) The neoplastic cells show diffuse positivity for CD20, suggesting B-cell-lineage lymphoma. (C) Diffuse positivity for BCL2 (×400), indicating B-cell-lineage lymphoma. (D) The neoplastic cells are negative for the germinal-center marker CD10 (×400), indicating a marginal-zone pattern surrounding reactive follicles. (E) Reactive T cells are positive for CD3 (×400). (F) Ki-67 labeling index is ~ 10%, as determined manually.
MALT 림프종의 병기 결정을 위하여 흉부 및 경부 CT를 시행하였고, 특별한 이상 소견은 관찰되지 않았다. 골수 조직 검사를 시행하였고 림프종의 골수 침범의 증거는 없었다. 이에 대하여 환자는 방사선 치료 중이며 17회에 걸쳐 총 30.7 Gy의 방사선 치료를 진행할 예정이다.
고 찰
원발성 췌장 림프종은 매우 드문 질환으로, 저자들이 문헌 고찰한 바로는 현재까지 국내에 보고된 원발성 췌장 림프종 증례는 8예가 있다(Table 1) [5-9]. 조직 소견은 광범위 큰 B세포 림프종이 4예로 가장 많고, T세포 림프종 2예, 역형성 대세포 림프종 1예, 버킷 림프종 1예가 있다. 첫 증상으로는 복통이 7예로 가장 많았고, 그중 3예는 임상적으로 급성 췌장염을 동반하였다. 본 증례와 같이 상부 위장관 출혈로 나타난 경우는 없었다. 외국 문헌 고찰에 따르면 원발성 췌장 림프종의 약 60%가 광범위 큰 B세포 림프종에 해당하였다. 또한 주된 임상 발현은 복통이 83%로 가장 많았고 상부위장관 출혈은 2%에 불과하였다[10].

Diagnosis, clinical presentation, and treatment of patients with primary lymphoma of pancreatic MALT in South Korea
원발성 췌장 림프종 중에서도 원발성 췌장 MALT 림프종은 국내에서는 아직 보고된 적이 없고, 현재까지 세계적으로 일본에서만 3예가 보고된 매우 드문 질환이다[2-4]. 첫 번째 보고는 2008년 Miwa 등[2]이 보고하였고, 77세 여자가 당뇨의 스크리닝 목적으로 복부 초음파를 시행 후 종양이 확인되었다. EUS 세침 흡인 생검을 시행하였고, MALT 림프종으로 진단받았다. 방사선 치료를 시행하였고 완전 관해를 얻었다. 두 번째 보고[3]는 55세 남자가 건강검진 목적으로 복부 초음파를 시행하였고 다발성 췌장 종양이 발견되었다. EUS 세침 흡인 생검을 시행하였고 악성 림프종이 의심되었으나 최종 진단을 얻지 못하였다. 따라서 수술을 시행하여 췌장 체부 국소 절제를 시행하였고 최종적으로 MALT 림프종으로 진단되었다. 방사선 치료를 시행하였고 완전 관해를 얻었다. 세 번째 보고[4]는 55세 남자가 건강검진 목적으로 복부 초음파를 시행하였고 췌장 두부의 종양이 확인되었다. 개복 하에 췌장 종양 절제 생검을 시행하였고 MALT 림프종으로 진단되었다. Rtuximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone (R-CHOP) 화학요법을 시행하였고 완전 관해를 얻었다.
원발성 췌장 림프종을 췌장 선암 및 췌장에서 발생하는 다른 종양과 감별하는 것은 여러 가지 진단 방법을 필요로 하며 종종 진단에 어려움을 초래하는 경우가 있다. 진단에 따라 이들 종양의 치료방법과 예후가 다르므로 감별진단이 중요하다. 이러한 질병의 특징으로 인하여, 조직 검사가 이루어지기 전까지 췌장의 림프종이 아닌 다른 종양성 질환들로 오인될 수 있으며 통상적인 췌장암 등으로 오인될 수 있는 여지도 있다. 본 증례의 경우 원발성 췌장 림프종과 췌장 선암과의 감별진단이 필요하였다. CT 검사(Fig. 2)에서 췌장에 비교적 커다란 종괴를 형성하면서도 간내 담관의 확장을 동반하지 않으며 황달 증상이 없었다. MRCP 검사(Fig. 3A)에서 소위 “duct penetrating sign” 소견인 췌장 두부 종양을 관통하는 주췌관이 잘 관찰되었고, 종양 상류 주췌관 확장이 동반되지 않았던 점은 췌장 선암보다는 원발성 췌장 림프종을 시사하는 소견이다[7]. 또한 췌장 선암은 조영 증강 CT에서 일반적으로 동맥기와 지연기 모두에서 정상 췌장 실질보다 저음영을 보인다. 하지만 원발성 췌장 림프종은 본 증례와 같이 조영증강 CT상 동맥기에서 정상 췌장 실질보다 저음영을 보이고 지연기로 갈수록 조영 증강을 보인다(Fig. 2). 또한, PET-CT에서 다른 장기에 원발성 종양을 의심할 만한 증거가 없고 다른 기관에 전이 소견이 없다는 점에서 전이암의 가능성은 떨어진다. 한편, 원발성 췌장 림프종은 자가면역성 췌장염으로도 오인될 수 있다[9]. 위에서 언급한 췌장 림프종의 췌장 영상 소견이 자가면역성 췌장염에서도 관찰될 수 있으며, 실제로 과거 자가면역성 췌장염 증례가 영상 판독상 췌장 림프종으로 오인되기도 하였다. 본 증례에서는 MRCP 검사에서 주췌관의 뚜렷한 협착이 관찰되지 않았다(Fig. 3A). 또한 혈청 IgG4 증가가 없었으며 췌장 생검 조직에서 시행한 IgG4 면역조직화학염색에서 양성인 형질구가 관찰이 되지 않았다.
원발성 췌장 림프종의 가장 흔한 조직 진단인 광범위 큰 B세포 림프종은 고등급 림프종으로, 이 경우 전신적 항암화학요법을 시행한다[10]. 반면에 저등급 림프종인 MALT 림프종의 경우, 위에서 발생하는 MALT 림프종은 Helicobacter pylori (H. pylori) 감염과 관련 있음이 알려져 있고, 위 MALT 림프종의 치료로는 H. pylori 제균 요법이 확립되어 있다. 그러나 위 이외의 장기에 발생하는 MALT 림프종의 경우에는 치료 방침이 아직까지 명확하게 확립되어 있지 않고[3], H. pylori 제균 요법의 효과 또한 입증되어 있지 않다. 위 이외의 장기에 발생하는 국소성 MALT 림프종은 방사선 치료를 우선적으로 고려할 수 있고, 다발성 장기 침범을 동반한 MALT 림프종의 경우에는 전식적 항암화학요법을 최우선으로 고려한다. 국소성 MALT 림프종은 중간 선량의 방사선 치료만으로 좋은 치료 결과와 예후를 보인다고 알려져 있다[3]. MALT 림프종은 일반적으로 다른 고등급 림프종과 비교할 때 좋은 치료 성적과 예후를 보이므로 정확한 조직 진단이 중요하다.
본 증례는 흑색변으로 내원한 환자에서, 췌장 두부 종양을 초음파 유도 내시경 하에 중심부 바늘 조직 검사를 통해서 원발성 췌장 MALT 림프종을 진단한 국내 첫 번째 증례이다. 수술 전 조직 진단을 통해서 불필요한 수술을 피할 수 있었으며 병변에 대하여 방사선 치료를 시행 중이다.