비만의 진단과 바이오마커
Diagnosis of Obesity and Related Biomarkers
Article information
Trans Abstract
Obesity is associated with various comorbidities, such as type II diabetes, hypertension, dyslipidemia, and cardiovascular disease. Gastrointestinal complications are also frequent and obesity is a direct cause of nonalcoholic fatty liver disease, and are risk factors for gastroesophageal reflux disease, pancreatitis, gallstone disease, diarrhea, dyssynergic defection, and various gastrointestinal cancers. Diagnosis is usually made by measuring body mass index (BMI). Although BMI is correlated with body fat mass, it may overestimate subjects with high muscle mass and underestimate subjects with low muscle mass. Co-measurement of waist circumference as a reflection of abdominal obesity for subjects with BMIs ranging from 25 to 35 kg/m2 has been recommended; however, it is still an anthropometric diagnosis that does not clearly discriminate subjects at risk for developing comorbidities. Biomarkers reflect the underlying biological mechanisms of obesity and can be used to characterize the obesity phenotype (i.e., at high risk for disease development) as well as a target for disease-causing factors. In this article, we describe the conventional diagnosis, biomarkers of obesity, and current challenges.
서 론
비만은 당뇨나 심혈관 질환으로 대표되는 대사증후군의 발병과 연관이 있으며, 소화기 질환 중에서는 비알콜성 지방간 질환의 직접적인 발병 원인이고 위식도역류 질환, 설사, 췌장염, 담석과 여러 위장관 암의 위험인자이다[1]. 국내 건강검진 표본 코호트 데이터를 이용한 연구 결과 과체중(body mass index [BMI] 23 kg/m2 이상 25 kg/m2 미만) 및 비만(BMI 25 kg/m2 이상)으로 인한 암의 장애보정생존연수(disability-adjusted life year)는 남성의 경우 10만 명당 1,740명(8.0%)이고 여성은 10만명당 2,373명(12.5%)으로 비만으로 인한 암의 질병부담이 큰 것으로 조사되었다[2].
바이오마커는 정상적인 또는 질병 발생에 대한 생체반응을 반영하고 질병의 치료에 대한 생체반응을 확인할 수 있는 지표로 객관적으로 측정이 가능하다[3]. 비만은 생활습관과 연관된 만성 질환의 중요한 원인과 위험인자로 치료와 합병증과의 연관성에 많은 연구가 집중되었지만 진단에 대해서는 상대적으로 연구가 부족하다. 본고에서는 이차성 비만(유전성, 신경내분비계 질환 또는 약물로 인한 유발 등)을 제외한 일차성 비만의 일반적인 진단, 합병증 발생의 고위험군을 선별하는 바이오마커와 그 개발에 대한 현재 연구에 대하여 기술하고자 한다.
본 론
비만의 진단과 계측적 바이오마커(conventional diagnosis of obesity and anthropometric biomarkers)
비만은 몸속에 지방이 과도하게 축적된 상태로 체중의 증가와 반드시 비례하지는 않는다. 하지만 가장 보편적으로 사용되는 비만의 진단법은 BMI (weight [in kilograms]/height2 [in meters])를 측정하는 것으로 세계보건기구와 서양 가이드라인에서는 비만을 BMI 30 kg/m2 이상으로 정의하였다[4,5]. BMI는 체지방량과 연관이 있고 쉽게 측정이 가능하며 체중 변화에 따른 추적에도 용이하게 사용할 수 있다. 또한 합병증의 발생과도 연관이 있는데 119,859명을 대상으로 영국에서 시행된 멘델리안 무작위 분석법(Mendelian randomization analysis)의 연구 결과에서는 BMI가 높을수록 심혈관 질환과 대사 질환이 증가하였다[6]. 국내 건강보험공단 검진자료와 통계청 사망자료를 바탕으로 한 코호트 연구 결과에서는 BMI를 기준으로 한 저체중(underweight), 과체중(overweight), 비만(obesity) 단계에 해당하는 군이 정상체중(normal)에 해당하는 군보다 사망률이 높았다[7]. 그러나 BMI는 지방량과 근육량을 구별할 수 없기 때문에 신체의 지방축적 정도를 제대로 반영하지 못하는 문제를 갖고 있다. 또한 아시아인에서 같은 BMI를 가진 서양인에 비하여 체지방률이 높다는 보고가 있으며[8,9], 서양인에 비하여 낮은 BMI 수치에서도 합병증의 발생위험이 증가하는 것으로 알려져 있다[10]. 따라서 세계보건기구 아시아·태평양 지역의 가이드라인과 국내 가이드라인에서는 BMI의 기준을 23 kg/m2부터 과체중 또는 비만 전 단계(pre-obese)로 구분하였고, 25 kg/m2부터 비만으로 정의하였다[11,12] (Table 1).
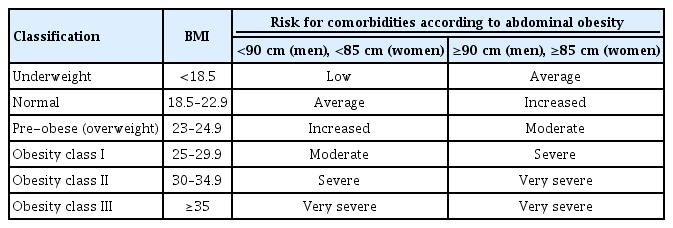
Classification of obesity/abdominal obesity and risk of comorbidities in Korea
비만과 관련된 합병증의 위험도는 지방의 분포 또한 영향을 미치는데, 피하지방보다는 내장지방(특히 복부)과 연관되어 있다[13-15]. 피하지방과 내장지방을 구성하는 면역세포와 그 분획이 다르며 절대적인 체내 지방의 양은 피하지방의 분획이 높지만 내장지방의 경우, 인슐린 저항성과 만성염증에 관여하는 물질을 보다 높은 비율로 분비한다[13,16]. 허리둘레(waist circumference)와 허리-엉덩이 둘레비(waist-to-hip ratio)가 BMI보다 내장지방량을 잘 반영하는 대표적인 지표로 허리둘레의 측정이 간편하기 때문에 선호되고 있다. 실제로 허리둘레의 경우 BMI가 낮은 환자의 경우에도 측정수치가 높을 경우 비만과 관련된 합병증의 발생 위험이 증가하는 것으로 알려져 있다[17]. 최근 발표된 국내 가이드라인에 따르면 허리둘레 90 cm (남성), 85 cm (여성) 이상을 복부비만의 기준으로 정하고 BMI와 함께 측정하여 비만 합병증 발생의 고위험군을 선별하고자 하였다[12] (Table 1). 하지만 이 지표들은 계측적인 바이오마커로 합병증 발생의 위험정도를 정확히 구별하기는 어렵다[18].
내장지방량과 그 분획을 정확히 측정하기 위해서 생체전기저항 분석법(bioimpedance analysis), 이중에너지 방사선 흡수법(dual-energy X-ray absorptiometry), 컴퓨터단층촬영(computed tomography), 자기공명영상(magnetic resonance imaging) 또는 자기공명분광법(magnetic resonance spectroscopy scan) 등의 방법을 사용할 수 있으나 계측적인 바이오마커에 비하여 측정이 복잡하기 때문에 보편적으로 사용되지 않는다[4].
새롭게 개발된 바이오마커(newly developing biomarkers)
비만과 합병증 발생의 주 병리기전은 인슐린축(insulin/insulin-like growth factor [IGF] axis) 신호전달체계의 저해와 지방조직의 면역반응으로 유발된 만성 염증이다[4]. 내장지방조직에서 분비되는 여러 사이토카인(cytokine)과 아디포카인(adipokine)이 비만과 합병증의 발생에 영향을 미치는 주요한 인자로 추측되었다. 앞서 기술한 신체의 수치를 측정하는 바이오마커의 경우 비만 환자를 선별할 수 있지만 합병증 발생의 위험을 가진 환자군을 정확히 선별하기는 어려웠다[18]. 분자생물학적 마커들의 경우에도 현재 비만환자의 진단이나 고위험군 선별에 사용하도록 권고되지는 않지만 비만과 합병증 발생의 유발기전을 탐구하거나 치료제 개발에 사용되고 있어 임상 진료에 적용하려는 시도가 지속되고 있다[4].
인슐린 축 신호전달체계 연관 바이오마커(insulin/insulin-like growth factor axis-related biomarkers)
Insulin-like growth factor 1
지방조직이 포화유리지방산과 tumor necrosis factor-α, interleukin-6와 같은 사이토카인을 과도하게 분비하면 인슐린 신호전달체계의 저해물질인 suppressor of cytokine signaling, c-Jun NH2-terminal kinase, protein-tyrosine phosphatase 1B 등의 물질을 활성화시켜 고인슐린혈증과 인슐린 저항성을 일으킨다[16,19]. 이는 비만이 당뇨나 고혈압, 심혈관 질환 등의 합병증을 일으키는 주 기전으로 알려져 있다[20]. 통상적으로 영양과잉 상태가 말초조직에서 인슐린 저항성을 일으키고 췌장의 인슐린 분비를 자극하여 고인슐린혈증이 발생하는 것으로 이해하였으나 비만 자체도 고인슐린혈증을 일으키고 간의 포도당신합성을 자극하여 인슐린 저항성을 일으키는 것으로 추측된다[21]. 인슐린의 대사는 IGF 축에 의하여 조절되는데 IGF-I은 정상세포뿐 아니라 유전적 손상이 있는 세포에서도 증식, 분화와 전이에 관여하고 있다[22]. IGF-I은 지방세포에서도 분비되는 호르몬으로, 비만 환자에서 체내 인슐린의 증가가 IGF-I의 활성도와 생체이용률(bioavailability)을 증가시킨다. 이는 곧 IGF binding protein (IGFBP-1, 2)의 생성을 감소시키며 간에서 IGF-I의 생성을 증가시킨다. 또한 인슐린 자체도 세포사멸을 저해하고 증식을 촉진시키는 작용을 갖고 있어, 체내 인슐린의 증가와 IGF-I의 생체이용률 증가가 비만이 암 발생에 관여하는 기전으로 추측된다[4]. IGF-I은 손상을 입은 혈관 내피에서 평활근세포를 증식시키는 작용이 있으며 세포사멸의 저해와 nitric oxide 합성관여 작용으로 인하여 동맥경화반을 안정화시키고 혈관 확장을 일으켜 비만이 심혈관 질환의 발생에도 기여하는 것으로 알려져 있다[23]. 하지만 IGF-I은 결합단백질에 따라 다양하고 복잡한 작용을 하는 호르몬이다. 혈중 인슐린이나 C-peptide의 측정은 BMI와 상관관계를 보이지만 혈중 총 IGF-I의 측정은 상관관계가 없었으며 free IGF-I의 경우만 비만 환자에서 정상 BMI군에 비하여 높은 수치를 보였다[4,24,25]. 대규모 코호트를 이용한 nested case-control 연구에서도 혈중 IGF-I이나 IGFBP-3를 측정하는 것이 대장암 발생의 위험과 연관성이 없었으며 메타분석에서도 IFG-I 수치와 대장암 발생의 상대위험도가 1.07 (95% 신뢰구간 1.01-1.14)이었다[26]. 또한 혈중 IGF-I 수치가 사망률이나 심혈관 질환의 발생과 U형 곡선형태의 연관성을 보이거나 IGF-1의 생체이용률이 대사증후군 구성요소의 숫자와 역 U형 곡선형태의 연관성을 보이는 등 어떤 형태의 IGF-1을 측정하는지에 따라서도(total, free, bound or bioactive IGF-1) 연구결과가 달라진다[27-30]. 따라서 IGF-I의 측정을 비만의 고위험군 선별 바이오마커로 임상에 적용하기에는 아직 근거가 부족하다.
Insulin-like growth factor binding protein
IGFBP-1의 경우 연구참가자의 체형을 “lean-stable”, “lean–moderate increase”, “lean–marked increase”, “medium-stable/increase”, “medium–marked increase”로 나누어 분석한 결과에서 BMI 수치를 보정 후 오직 “lean–marked increase”군에서만 “lean-stable”군에 비하여 낮은 수치를 보였다[31]. IGFBP-3의 경우에도 제2형 당뇨병을 가진 비만 환자에서 당뇨병이 없는 비만환자나 BMI가 정상인 환자에 비하여 혈중 수치가 증가하여 IGFBP-3가 인슐린 저항성이 있는 경우 증가하는 것으로 추측되나 앞서 기술한대로 비만 관련 합병증과는 연관성이 없거나 연구의 숫자가 적어 추가적인 연구가 필요하다[32].
Insulin/C-peptide
공복 인슐린 수치가 증가하는 것은 고혈압이나 관상동맥 질환의 발생과 연관이 있으며[33], C-peptide 수치의 상승이 기저 당뇨병이 없는 환자에서 심혈관 질환으로 인한 사망률과 연관성이 있다는 보고가 있다[34]. 또한 혈중 인슐린/C-peptide의 증가가 췌장암 또는 대장암의 발생이나 바렛식도 환자에서 식도선암의 발생과 연관이 있다는 보고가 있지만[34-37], 이 연구들은 비만 환자만을 대상으로 바이오마커를 개발하여 고위험군을 선별하고자 한 연구가 아니며 임상적인 검증이 이루어지지 않았기 때문에 진료에 그대로 적용하기는 어렵다. 하지만 IGF축에 대한 이해가 높아지는 만큼 인슐린, proinsulin, C-peptide 등의 전통적으로 연구되어온 마커들을 포함하여 IGF축과 연관된 바이오마커의 임상적인 검증이 가능하리라 생각한다.
아디포카인(adipokines)
비만은 지방세포에 과도한 에너지를 저장하고 이는 세포 비대와 과증식을 일으켜 소포체 스트레스(endoplasmic reticulum stress)와 미토콘드리아의 기능 이상을 일으킨다[38]. 또한 대식세포를 포함한 면역세포가 활성화되면서 아디포카인 분비의 불균형을 일으켜서 전신의 인슐린 저항성과 비만 합병증의 발생에 기여하는 것으로 생각된다[38]. 비만은 대표적으로 염증성 아디포카인인 leptin이나 resistin의 분비를 촉진하고 항염증성 아디포카인인 adiponectin의 분비를 감소시킨다.
Leptin
Leptin은 지방조직의 양을 반영하는 아디포카인으로 식욕을 조절하고 대사에 관여하여 에너지 소비를 조절한다(즉, 시상하부에 혈류에 의하여 전달되어 주로 식욕을 감소시키고 대사를 촉진하는 작용을 한다) [39]. 비만은 leptin 신호전달체계를 저해하여 혈중 leptin 농도의 상승을 일으킨다(leptin resistance) [40]. 이외에도 혈압이나 인슐린 감수성 조절, 지방산의 이화작용, 혈소판 응집과 혈전생성, 심근비대, 혈관신생 등에 관여하기 때문에 비만의 합병증 중에서 심혈관 질환을 예측하는 마커로 알려져 있다[41,42]. 역학 연구들을 대상으로 시행된 최근의 메타분석에서는 leptin 수치가 심혈관 질환이나 뇌졸중의 발생과 연관성이 없었으나[41,43], 일부 leptin receptor (LEPR) gene의 유전적 변이가 심혈관 질환의 발생과 연관이 있었다[42]. 암의 발생에 관해서는 환자-대조군 연구에서 혈중 leptin 수치가 높을수록 대장암 발생의 위험이 증가한다는 보고가 있었으나 메타분석에서는 유의하지 않았다[44]. 혈중 soluble leptin receptor를 측정하는 것이 대장암 발생의 위험과 역의 상관관계를 보인다는 역학 연구들이 있지만 단독 측정으로는 그 역할이 제한적이다[45,46]. 혈중 leptin 수치 증가가 바렛식도 환자에서 식도선암의 발생[38]이나 자궁내막암의 발생위험[47], 간세포암의 치료 후 재발과 연관이 있다는 보고[48]가 있지만 후속 연구가 부족하다.
Adiponectin
Adiponectin은 지방세포에서 분비되는 아디포카인이지만 복강 내 지방이 증가할 경우 그 분비가 감소하고 혈중 농도가 BMI와 역의 상관관계를 보이는 것으로 알려져 있다[49]. Adiponectin은 대식세포의 tumor necrosis factor-α 생성을 억제하는 등의 염증 억제기능을 갖고 있으며, 혈중 수치의 감소는 인슐린 저항성 증가와 관련이 있다. 또한 세포의 증식을 억제하고 세포사멸을 유도하여 암 발생기전을 억제하는 기능을 갖는 것으로 추측된다[50].
암 발생과의 연관성의 경우 전향적 코호트 연구에서 혈장 adiponectin의 농도는 남성에서 대장암 발생 위험도와 역의 상관관계를 보이는 것으로 분석되었으며[51], 메타분석에서도 남성에서 대장 신생물의 발생과 역의 상관관계를 보였다[52]. 또한 위암의 발생 위험과도 연관되어 있다는 보고[53]가 있지만, 관상동맥 질환이나 뇌졸중의 발생 위험과 연관성이 없으며[54], 대장암의 발생과 인과관계를 증명할 수 없다는 보고[55]도 있어 추가적인 연구가 필요하다. 또한 high-molecular weight adiponectin이 인슐린 감수성과 관련이 있으며 low-molecular weight adiponectin이 항염증작용과 관련이 있다는 보고가 있기 때문에 이들 분획을 구별한 검증도 필요하리라 생각한다[56].
Resistin
Resistin은 염증, 혈관내피 기능 이상(혈전생성, 혈관신생), 혈관의 평활근세포 증식 등에 관여하여 심혈관 질환의 발생에 영향을 주는 호르몬이다[57]. 당뇨나 관상동맥 질환을 대상으로 한 코호트 분석에서는 혈중 resistin 농도가 사망률과 연관성이 있는 것으로 분석되었으나, 메타분석에서는 전체 사망률 위험도 1.21 (95% 신뢰구간 1.03-1.42), 심혈관 질환 사망률 위험도 1.05 (95% 신뢰구간 1.01-1.10)로 그 증거가 다소 부족하였다[58]. 하지만 제2형 당뇨병 환자를 대상으로 혈중 resistin 농도와 전체 사망률과의 위험성을 확인한 코호트 연구 결과에서는 유의한 인과관계가 있다는 보고도 있어 추가적인 임상연구가 필요하다[59].
Apelin
Apelin은 체액의 항상성과 혈압 유지, 죽상경화보호, 에너지대사 등의 생리적 활성을 조절하는 리간드(ligand)인데 지방세포에서도 분비되기 때문에 아디포카인으로도 분류된다[60]. 혈중 apelin 수치의 감소가 백인에서 고혈압 발생의 위험이나[61] 관상동맥 질환의 발생과 연관성이 있다는 보고가 있지만[62], 모두 관찰 연구를 대상으로 한 메타분석의 결과로 비만 환자를 대상으로 한 연구는 아니었다. 비만 환자를 대상으로 한 연구에서는 혈중 apelin 수치가 비만에서 감소하거나[63,64] 증가한다는[65,66] 다양한 결과를 보였다[60]. 지방세포에서 apelin의 생성은 인슐린에 의해 유발되어 혈중수치가 고인슐린혈증이나 인슐린 저항성과 연관되어 있지만[67], 실제로는 신체 부위에 따라 apelin이 다른 발현을 보이기 때문에 일치된 결과를 보이지 않는 것으로 추측된다[60]. Homeostasis model assessment for insulin resistance를 기준으로 한 인슐린 저항성과 혈중 apelin 수치의 관계도 양의 상관관계나 음의 상관관계를 보인다는 연구들이 혼재되어 있어 결론을 내리기 어렵다[65]. 하지만 apelin은 에너지 대사에 관여하여 비만 발생 기전과 연관이 있으며 동물실험에서 인슐린 감수성을 증가시키고 지방조직을 감소시키는 효과를 보여 비만과 당뇨병의 치료제로 사용될 가능성이 활발히 연구되고 있어 추가적인 연구 결과가 기대된다[68]. 전체적으로 아디포카인이 비만과 그 합병증 발생에 관여하는 기전이 잘 알려져있으나 임상적인 검증은 아직 부족하다. 또한 아디포카인을 종류별로 병합하여 검증한 연구 또한 드물어 이들 간의 상호작용에 대한 이해가 필요하다.
Gastrointestinal hormones
대부분의 탄수화물은 소장 근위부에서 흡수되기 때문에 위배출(gastric emptying) 속도가 탄수화물의 전신 흡수를 조절할 수 있으며 위배출을 조절하는 위장관 호르몬들이 시상하부의 식욕이나 혈당조절에도 관여하기 때문에 비만치료의 중요한 기전으로 연구되었다[69]. 비만치료 후에 체중과 대사, 음식물에 대한 욕구의 변화가 오는데 위장관 호르몬의 변화는 이에 대한 주 기전(위장관 호르몬 변화, 담즙산 대사 변화, 장내세균 변화) 중 하나이다[70,71]. 인크레틴으로 대표되는 호르몬들(gastric inhibitory polypeptide [GIP], glucagon-like peptide [GLP] 1, peptide tyrosine–tyrosine [PYY], cholecystokinin [CCK])로 주로 위배출을 지연시켜 포만감을 유발한다[69]. 하지만 ghrelin이나 motilin의 경우 위배출을 촉진하여 배고픔을 유발하거나 식욕을 증가시키기 때문에 이들 호르몬이나 호르몬 수용체에 작용하는 기전을 조절하여 치료효과를 얻거나 비만 환자의 수술 후 변화를 측정하는 마커로 연구되었다[69].
Peptide tyrosine–tyrosine
PYY는 원위부 소장과 대장의 L형 장내분비세포(enteroendocrine L cell)에서 음식물과 영양소에 의하여 분비가 자극된다. 장내 음식물에 대한 반응으로 위배출과 장운동 속도가 저하되는 소위 ‘ileal brake’에 관여하며 식욕저하를 일으키는 것으로 알려져 있다[69]. 혈중 PYY 수치는 BMI와 역의 상관관계를 보이고 공복이나 식후의 PYY 수치가 비만 환자에서 낮은 수치를 보이며 체중 감량이 혈중 PYY 수치의 증가를 일으킨다는 보고[72]가 있다. 하지만 PYY 수치가 BMI나 체중과 연관성이 없다는 보고[73]도 있으며 고지방식이에 대해서만 수치의 변동을 일으킨다는 연구[74]도 있어 비만 발생기전의 이해에 추가적인 연구가 필요하다.
Pancreatic polypeptide
Pancreatic polypeptide는 식후에 췌장에서 분비되는 호르몬으로 식욕을 억제하고 위배출을 지연시키며 위 적응에도 영향을 미친다[70]. 공복의 혈장 pancreatic polypeptide 농도가 전신 자기공명촬영을 이용하여 측정한 내장지방의 정도나 간내 지방축적의 정도를 독립적으로 예측할 수 있다는 보고가 있지만 연구의 대상 환자 수가 적었다[75].
Motilin
Motilin은 소장에서 주로 분비되어 공복시에 발생하는 위의 운동인 phase III migrating motor complex를 유발한다. 비만 환자에서 대조군에 비하여 migrating motor complex 동안의 혈장 motilin 수치가 높고 Roux-en-Y gastric bypass 비만수술 이후에 그 수치가 감소한다는 보고가 있지만 연구의 대상 환자 수가 적었다[76].
전체적으로 위장관 호르몬을 통하여 비만의 고위험군을 선별하기는 아직 어려운 상태로 추가적인 연구가 필요하다. 하지만 인크레틴을 바탕으로 개발된 약물이 당뇨와 비만의 치료 및 치료제 개발에 사용되고 있어 기타 위장관 호르몬들의 연구를 통하여 추가적인 바이오마커의 개발이 가능하리라 생각된다.
Multi-Omics biomarkers
질병 발생의 생물학적 경로는 복잡한 방식으로 상호작용하며, 이는 특정 바이오마커의 개발을 어렵게 만드는 요인이다[38]. 이를 극복하기 위하여 genomics, transcriptomics, metabolomics, proteomics 등의 “Omics” 기반의 바이오마커 개발이 이루어지고 있다. 역학 연구를 바탕으로 추출된 샘플을 통하여 Omics 플랫폼의 분석을 적용하여 바이오마커를 개발하고 임상 검증을 하는 것이 일반적인 순서이다.
2,577명의 Korean Association REsource (KARE) 코호트를 대상으로 비만과 관련해서 가장 활발히 연구되었고 강력한 유전적 영향을 미치는 것으로 알려져 있는 fat mass and obesity associated (FTO) gene의 대사물질을 분석하여 제2형 당뇨와 비만과 연관된 7개의 phosphatidylcholine metabolic pathway 연관 대사물질을 발견한 국내 연구가 수행되었으나 추가적인 임상 검증이 이루어지지 않았다[77].
MicroRNA (miRNA)는 비발현 RNA 분자 중 하나로 유전자 발현을 조절하는 기능을 갖고 있으며 체액에서 안정적으로 검출이 가능하다. 또한 특정 질환들의 임상 발현 이전에도 진단에 사용할 수 있는 것으로 알려져 있어 바이오마커로 연구되었다. 하지만 비만의 경우 연구의 대상 환자 수가 적거나 연구마다 결과가 상이하여 다양한 miRNA를 바이오마커로 각각 제시하고 있어 임상 적용이 어렵다[38,78].
전반적으로 비만과 연관되어 알려진 유전자 변이의 숫자가 많고 각 변이의 효과 크기는 크지 않아 임상에 적용하기가 어렵다. 하지만 최근 유전자의 상호작용을 검증하는 연구들이 수행되고 있고 전장유전체 연관 분석을 통하여 확보된 single nucleotide polymorphisms (SNP)를 대상으로 개인의 유전적 위험도 계산(genetic risk score, polygenic risk score)이 가능한 만큼 추후 omics 기반의 바이오마커의 임상 적용이 가능하리라 생각된다[79,80].
최근 노르웨이에서 시행된 대규모 코호트 연구 결과 유전적으로 비만 발생의 위험이 높은 군(기존에 밝혀진 96개의 비만 관련 SNP를 바탕으로 유전적 위험도를 계산)은 위험이 낮은 군에 비하여 더 높은 BMI를 보였다[81]. 하지만 유전적으로 비만의 위험도가 낮은 군 역시 1960년대 중반부터 2000년대 중반까지 꾸준히 BMI가 증가하여 유전적 요인 이외에도 환경적인 요인 역시 비만의 발생에 중요한 영향이 있음을 시사하였다[81]. 상기 연구에서 FTO SNP의 BMI 관련성을 조사하였으나 여러 SNP를 병합하여 유전적 위험도를 계산하였을 때보다 관련성이 낮은 것으로 조사되었다. 따라서 전장유전체 연관분석 뿐만 아니라 유전-환경 상호작용 연구(genome-wide interaction study) 또한 중요함을 시사하였다. 비만의 발생을 설명력이 낮은 단일 유전자 변이로 설명할 수는 없으며 여러 유전자 변이를 통한 유전적 위험도 계산과 함께 환경적인 요인과의 상호 작용을 고려하는 연구들이 더욱 늘어난다면 비만과 합병증 발생의 고위험군을 선별하는 데 도움이 될 것으로 기대된다.
Gut microbiome
장내세균의 불균형(dysbiosis)은 세균 종이나 그 수의 변화로 인한 다양성이 저하되어 발생하며 항생제 사용, 감염, 면역 이상 등에 의하여 발생이 가능하다. 장내세균의 불균형이 비만의 바이오마커로 활용될 수 있는지 연구되었으며 비만은 장내세균의 다양성이 감소하고[82], 특히 Bacteroidetes phylum이 감소하고 Firmicutes phylum이 증가하는 등의 특징적인 구성을 보인다고 분석되었다[83]. 하지만 이는 비만에서만 보이는 특징은 아니며 임상적인 검증 연구가 이루어지지는 않았다. 고지방, 고당, 저섬유소 식이는 장 투과성을 증가시키고 이는 세균전위나 혈액 내 세균의 내독소를 증가시켜 전신성 염증을 일으키고 대사성 질환의 발생에 기여한다. 하지만 소위 새는 장 증후군(leaky gut syndrome)으로 불리는 이런 현상 역시 비만에서만 관찰되는 것이 아니며 임상적인 검증 연구가 드물다. 최근에는 특정 균의 대사적인 특징을 고려한 분석이 이루어지고 있어 새로운 진단과 치료제 개발이 기대된다.
Combined biomarkers
Triglyceride and glucose (TyG) index는 triglyceride와 공복 glucose 수치를 이용하여 계산하는 지표로 인슐린 저항성과 연관성이 있으며 제2형 당뇨, 고혈압, 대사증후군을 선별하기 위한 바이오마커로 연구되었다[84]. 최근 국민건강영양조사 자료를 이용하여 비만의 계측적인 바이오마커들과 TyG index를 병합하여 homeostasis model assessment for insulin resistance를 기준으로 한 인슐린 저항성을 예측하기 위한 연구가 수행되었다. 여러 지표들 중에서 TyG index와 BMI를 병합하였을 때 area under the curve 값이 0.748로 가장 높은 수치를 보였지만 전향적 검증이 이루어지지 않은 단면 연구로 추가적인 자료가 필요하다[84].
Visceral adiposity index (VAI)는 허리둘레와 BMI, 혈청 triglyceride, high-density lipoprotein (HDL) cholesterol 수치를 이용하여 계산한 지표로 인슐린 저항성과 관련이 있으며 심혈관계 질환의 발생 위험도와의 연관성이 보고되었다. 2,204명의 국내 환자를 대상으로 시행된 코호트 연구에서 VAI가 높을수록 Wildman criteria를 바탕으로 정의한 metabolically healthy obesity에서 metabolically unhealthy obesity로 전환되는 비율이 높다고 분석되었다[85]. 하지만 VAI는 Caucasian을 대상으로 개발된 지표로 국내 환자를 대상으로 활용하기에는 제한이 있었다. 최근 우리나라에서 개발된 새로운 VAI는 평균 혈압과 나이를 지표에 추가하여 기존의 VAI보다 심뇌혈관 질환의 발생을 보다 잘 예측할 수 있는 것으로 분석되었다[86].
앞서 기술한대로 혈중 soluble leptin receptor를 측정하는 것이 대장암 발생의 위험과 연관이 있지만 단독 측정으로는 그 역할이 제한적이다. 최근 nested case-control 연구에서 여러 바이오마커의 조합 중 HDL cholesterol, 비고분자 adiponectin (non-high molecular weight adiponectin)과 함께 soluble leptin receptor를 측정하는 것이 지방축적과 대장암 발생과의 관계를 설명할 수 있는 바이오마커로 분석되었지만 후속 연구가 부족하다[45].
기존에 연구되어온 계측적인 바이오마커나 아디포카인 등과 같은 혈액 내 표지자 그리고 최근에 연구되는 장내세균 또는 “Omics” 기반 바이오마커를 병합한 연구는 찾아보기 어렵다. 비만의 발생기전이 복합적이고 개인마다 다양할 가능성이 있어 비만의 다양한 병리기전을 대변하는 바이오마커의 병합 연구가 필요하다.
Functional gastrointestinal disorders-related biomarkers
기능성 위장 질환과 비만과의 관계는 위식도역류 질환과 배변 장애 등에서 유의한 결과를 보이고 있고 이외에는 증상별로 일치되는 결과를 보이지 못하고 있으나 설사와의 연관성이 높게 제시되고 있다[1]. 이런 연관성이 인과관계인지는 자료가 부족하나 체중 감량이 상하복부 증상들을 경감시킨다는 보고가 있어 잠재적인 인과관계가 있다고 추측된다[87].
전화면담(ROME III criteria), 복부 컴퓨터단층촬영, 상부 위장관 내시경 건강검진 자료를 이용한 후향적 연구로 기능성 소화불량과 비만과의 연관성을 조사한 결과 visceral adipose tissue area와 visceral adipose tissue area/subcutaneous adipose tissue area 비율이 기능성 소화불량과 연관성이 있는 것으로 조사되었으나 단면 연구이고 기전을 탐색하는 연구는 아니었다[88].
328명을 대상으로 한 전향적 연구에서 비만 환자는 포만감을 느끼기 위한 위용적이 정상 BMI군보다 크며 BMI가 클수록 보다 큰 위 용적을 보였다[89]. 위 배출시간 또한 비만 환자에서 정상 BMI군보다 빨랐지만 상기 지표들은 비만의 고위험군을 선별하기 위한 바이오마커는 아니며 기존 비만 진단을 대체하기는 어렵다.
13명의 특발성 위 마비 환자와 19명 대조군의 위벽 전층 조직 검사를 통한 분석 결과 비만 환자에서 근육의 수축과 연관된 mRNA의 발현이 증가하여 위의 운동성 증가와 비만과의 관계를 시사하였다[90]. 위 마비 환자군에서는 platelet-derived growth factor BB subunit 관련 mRNA의 발현이 감소하여 위의 운동성 감소를 시사하였으며 비만 환자군과 위 마비 환자군이 공통적으로 염증과 관련된 유전적 변형을 보여 비만과 기능성 질환과의 연관성을 시사하였다[90].
전반적으로 비만과 기능성 위장 질환과의 연관성을 탐색하거나 발생기전에 대한 연구가 수행되었지만 바이오마커에 대한 연구는 드물다. 체중 감량이 기능성 위장 질환의 증상 경감과 연관이 있다는 보고가 있는 만큼 바이오마커 개발을 통한 비만 환자의 위험도 구분이 기능성 위장 질환의 치료에 영향을 미치는지 확인이 필요하다.
Current perspectives
현재 비만의 바이오마커 개발현황은 비만 자체의 마커보다는 비만을 고려하지 않은 합병증(당뇨, 고혈압, 심혈관 질환, 대사증후군 등)의 바이오마커가 대부분이다. 어떤 연구대상을 선택하는지에 따라 선택편향이 발생할 수 있으며 해석 또한 달라지기 때문에 비만 환자를 대상으로 한 바이오마커의 개발 연구가 필요하다. 또한 바이오마커의 개발을 위하여 후향적으로 환자 대조군 연구를 시행하여 이미 질병이 진단된 상태에서 환자의 샘플을 통하여 분석을 시행할 경우 기저질환에 의해 샘플이 영향을 받는 경우가 있다(reverse causation) [4]. 전향적 코호트를 이용한 바이오마커의 기능 검증 연구가 드문 것 또한 임상적인 적용이 어려운 이유이다. 한 종류의 바이오마커가 복잡한 질병기전을 가진 비만의 합병증을 모두 예측하기는 어렵기 때문에 여러 바이오마커를 병합한 합병증 발생 예측모델의 개발이 필요하다. 또한 아시아인을 대상으로 한 비만 연구는 서양의 연구와 종종 다른 결과를 보이기 때문에 인종에 따른 분석 또한 필요하다. 이런 내용들을 고려할 때 새로운 바이오마커가 현재의 BMI와 허리둘레 측정을 기준으로 하는 계측적인 진단법을 아직 대체할 수는 없지만 이것이 합병증 발생의 고위험군을 정확히 선별하기는 어렵다는 점을 고려할 때 바이오마커의 개발 연구는 여전히 중요하다(Table 2).
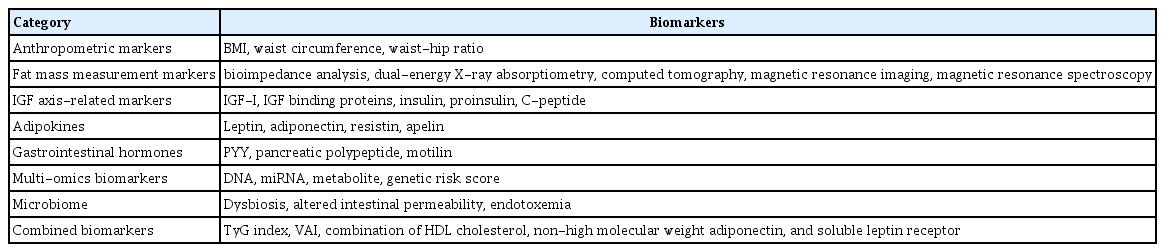
Potential obesity biomarkers
결 론
비만의 유병률이 증가하고 있으나 모든 비만 환자가 합병증 발생의 고위험군은 아니기 때문에 동일한 방식의 선별 검사를 적용하는 것은 무리가 있다. 인구의 고령화와 더불어 심혈관 질환과 당뇨 등의 대사증후군 요인에 대한 선별 검사가 강조되는 만큼 비만의 바이오마커 개발이 더욱 중요한 시점이다. 통상적으로 비만의 진단에 사용되는 BMI와 허리둘레의 측정 이외에는 비만의 고위험군을 간단히 구별할 수 있는 마커는 아직 개발되지 않았다. 국내 환자를 대상으로 기존에 개발된 마커들을 검증하는 연구와 잠재적인 바이오마커들을 병합한 연구들을 통하여 비만의 합병증 발생을 예측할 수 있는 고위험군의 선별이 가능한 시대를 기대해 본다.