한국인에서 D-Dimer의 위양성과 관련된 인자와 검사의 정확도 향상을 위한 Cut-Off Value
Cut-Off Value and Factors Associated with a False Positive D-Dimer Result for Venous Thromboembolism in Koreans
Article information
Abstract
목적:
폐동맥 색전증과 심부 정맥 혈전증 이외에 D-dimer 검사의 양성 결과를 나타내는 여러 질환들이 보고되고 있으나, 현재까지 한국인에서 위양성을 유발하는 인자에 대해서는 명백하게 알려진 바가 없다. 따라서 한국인에서 위양성을 초래하는 인자들을 확인하고, 정확도를 향상시키기 위한 새로운 cut-off value를 제시하고자 한다.
방법:
2009년 1월부터 12월까지 본원에 방문한 환자 중 다양한 이유로 D-dimer 검사를 시행 받은 2,047명의 환자를 대상으로 분석하였고, 위양성을 유발하는 인자들을 확인하기 위해 오즈비와 95% 신뢰구간을 로지스틱 회귀분석을 이용하여 분석하였다. 새로운 cut-off value는 ROC curve를 이용하여 구하였다.
결과:
연령의 증가, 외상, 수술의 기왕력, 급성 감염, 결핵, 뇌혈관 질환, 악성종양, 만성 신부전, 급성 관동맥 증후군, 심부전, 호흡기 질환 등이 D-dimer 검사의 위양성을 유발하는 인자로 확인되었다. 또한 민감도와 특이도를 향상시키기 위해 ROC curve를 이용하여 구한 새로운 cut-off value는 0.68 mg/L였다(65세 이하에서는 0.58 mg/L, 65세 이상에서는 0.77 mg/L).
결론:
여러 인자들이 D-dimer 위양성과 관련이 있었으며, 임상에서 D-dimer 검사를 시행하고 임상에 적용할 때에는 이러한 인자들이 결과치에 영향을 줄 수 있음을 충분히 고려하여야겠다.
Trans Abstract
Background/Aims:
The D-dimer value is a simple blood test used to evaluate venous thromboembolism (VTE). However, due toits low specificity, another test is needed for a definite diagnosis, such as a radiographic test. We evaluate the factors associated witha false positive D-dimer test and propose a new cut-off value for detecting VTE more effectively in Koreans.
Methods:
This was a retrospective, observational study. From January 2009 to December 2009, 2,047 patients (988 men, 63 ± 15years) had the D-dimer value checked to evaluate VTE. The main outcome of interest was a positive D-dimer test. Odds ratio and95% confidence intervals were determined using logistic regression analysis. The new D-dimer cut-off was evaluated usingreceiver operating characteristics (ROC) curves.
Results:
The result was positive in 1,093 patients (53%), for a false positive percentage for VTE of 95% and a false negativepercentage for VTE of 1%. Significant false positive predictors for a positive D-dimer were increasing age, trauma, postoperative,acute infection, tuberculosis, stroke, malignancy, chronic renal failure, acute coronary syndrome, heart failure, and lung disease.The discriminative value of the D-dimer test was assessed using ROC curve analysis. A D-dimer value of 0.68 mg/L on admissionwas the best cut-off value for predicting the development of VTE with a sensitivity of 95% and specificity of 57%.
Conclusions:
Many factors affect the D-dimer value and we must consider these factors before using the D-dimer value to evaluateVTE. A D-dimer value of 0.68 mg/L appears to be a good cut-off value for evaluating VTE more effectively in Koreans. (Korean JMed 2013;84:372-378)
서 론
혈청 D-dimer 측정은 일반적으로 급성 폐동맥 색전증을 진단하기 위해 일차적으로 시행되는 검사다. D-dimer 검사는 비관혈적이고, 결과를 빨리 확인할 수 있어 폐동맥 색전증을 확인하기 위한 매우 유용한 검사이다[1]. 그러나 D-dimer 검사는 특이도가 40%에서 60% 정도로 낮기 때문에 그 유용성이 제한된다[2]. 폐동맥 색전증과 심부 정맥 혈전증을 제외하고, 몇 가지 질환에서 D-dimer의 양성 소견을 보이는데, 고령의 나이, 악성 종양 그리고 임신과 같은 경우에서 폐동맥 색전증과 심부 정맥 혈전증이 없음에도 불구하고 D-dimer가 양성 값을 보이는 것으로 보고되었다[3-11]. 특히, 환자의 연령이 높아질수록 특이도가 유의하게 낮아지기 때문에 나이가 많은 환자에서 D-dimer의 유용성은 현저하게 낮아진다[3,4].
현재까지 한국인에서 D-dimer의 위양성에 영향을 미치는 질환에 대해서는 명백하게 알려진 바가 없고, 실제 임상에서 폐동맥 색전증과 심부 정맥 혈전증이 발생한 환자를 대상으로 D-dimer의 결과치와 그에 따른 민감도와 특이도에 대해서도 명확히 알려진 바가 없다. 따라서 본 연구는 한국인에서 D-dimer 검사의 폐동맥 색전증과 심부 정맥 혈전증 진단의 민감도와 특이도를 구하고, 좀 더 효과적으로 이를 진단할 수 있는 새로운 cut-off value를 제시하며, 또한 D-dimer 위양성을 초래하는 인자들을 확인하고자 시행하였다.
대상 및 방법
대상
2009년 1월부터 12월까지 본원에 방문한 환자 중 폐동맥 색전증과 심부정맥 혈전증을 진단하기 위해 D-dimer 검사를 시행 받은 2,047명의 환자를 대상으로 후향적 분석을 하였다. 평균나이는 63 ± 15세였으며 남자가 988명, 여자가 1,059명이었다.
연구 방법
2,047명의 환자를 대상으로 환자의 나이, 성별, 동반 질환과 최종 진단명에 대해 전자 의무기록을 분석하여 얻었다. 환자들은 효소-연결면역 흡수측정검사(enzyme-linked immunosorbent assay; VIDAS D-dimer exclusion, bioMérieux, SA, USA)를 이용하여 혈청 D-dimer를 측정하였고, D-dimer의 농도가 0.5 mg/L 이상인 경우를 양성으로 정의하였다. 폐동맥 색전증과 심부 정맥 혈전증은 다검출기 전산화 단층촬영 검사, 폐 환기-관류 스캔, 압박 정맥 초음파검사, 고식적 정맥조영술을 통해 진단하였다.
통계 분석
연속형 변수는 평균 ± 표준편차로 나타냈고, 범주형 변수는 빈도 및 퍼센트로 나타냈다. 통계 분석은 윈도우용 SPSS 14.0 (Statistical package for the social science, SPSS-PC Inc. Chicago, IL, USA)을 이용하였다. 오즈비(odds ratio)와 95%신뢰구간(confidence interval)은 로지스틱 회귀분석을 시행하였다. 통계 분석 결과 p 값이 0.05 미만에서 통계학적으로 유의한 것으로 간주하였다. D-dimer의 새로운 cut-off value는 ROC curve를 이용하여 분석하였다.
결 과
임상적 특징
총 2,047명의 환자에서 D-dimer 검사가 시행되었다. D-dimer가 양성인 1,093명 중, 폐동맥 색전증과 심부 정맥 혈전증으로 진단된 환자는 56명으로 양성예측도는 5%였으며, D-dimer가 음성인 954명 중, 폐동맥 색전증과 심부 정맥 혈전증이 진단되지 않은 환자는 946명으로 음성 예측도는 99%였다. D-dimer 검사의 cut-off value를 현재 사용되고 있는 0.5 mg/L로 했을 때에 민감도는 88%, 특이도는 48%였고, 위양성률은 95%, 위음성률은 1%로 관찰되었다(Fig. 1). D-dimer 검사가 시행된 전체 환자의 평균 연령은 63 ± 15세였다. 연령이 증가할수록 D-dimer 양성률이 증가하는 경향을 보였으며, 60대 이상에서는 50% 이상에서 D-dimer 양성 결과를 보였다. 각 기저질환 별로 진양성에 대한 위양성의 비율, 곧 D-dimer가 양성으로 나왔을 때, 그 양성 결과가 위양성일 확률이 높은 질환으로는 급성 감염, 수술을 받은 기왕력, 외상 등 이었다(Table 1). 특히, 급성 감염의 경우 그 수치가 가장 높았는데 급성 감염의 종류로는 신우 신염, 간농양, 봉와직염 등 다양한 감염병(220명)이 확인되었고, 특히 폐렴 (104명, 47.2%)의 빈도가 가장 높았다. 그리고 수술의 기왕력의 경우 정형외과적 수술이 가장 많았고(55명, 73.3%), 수술한 뒤 D-dimer 검사는 수술일에서부터 수술 후 44일까지 시행되었으며, 중간값은 8일이었다. 외상의 경우 대부분의 환자에서 골절이 동반된 외상이었으며, 골절이 확인되지 않은 환자의 경우 외상에 의한 지주막하 출혈, 교통사고 등에 복합적인 타박상 등 중증의 외상에서 D-dimer 검사가 시행되어(80명) 대부분의 환자에서 D-dimer의 양성 소견이 관찰되었다(78명, 98%).
The study population. VTE, venous thromboembolism.

Baseline characteristics
D-dimer 검사의 위양성 결과와 관련된 질환들에 대한 로지스틱 회귀분석
D-dimer 검사에서 양성 결과를 보이는 질환들에 대한 로지스틱 회귀분석의 결과, 연령의 증가, 외상, 수술의 기왕력, 급성 감염, 결핵, 뇌혈관 질환, 악성종양, 만성 신부전, 급성 관동맥 증후군, 심부전, 호흡기 질환 등이 D-dimer 위양성을 유발하는 인자로 확인되었다(Table 2). 이 중 가장 관련성이 높은 질환은 수술의 기왕력이었고(OR = 42.70 [95% CI = 5.55 to 328.80], p< 0.001), 폐결핵, 기관지 결핵, 결핵성 흉막염 등, 결핵에 의한 감염도 유의한 유발인자로 관찰되었다(OR = 6.36 [95% CI = 2.73 to 14.77], p< 0.001). 그리고 안정형 협심증과 변이형 협심증을 포함한 심혈관 질환의 경우 D-dimer 검사의 위양성 결과와 관련성이 없었으나, 급성 관동맥 증후군만을 분석하였을 때는 D-dimer 검사의 위양성을 유발하는 인자로 확인되었다(OR = 3.01 [95% CI = 1.21 to 7.48], p= 0.018). 그리고 연령을 65세 기준으로 나누었을 때 65세 이상의 환자들이 65세 미만의 환자들에 비해 위양성을 나타낼 가능성이 높았다(OR = 1.93 [95% CI = 0.66 to 12.38], p= 0.008).
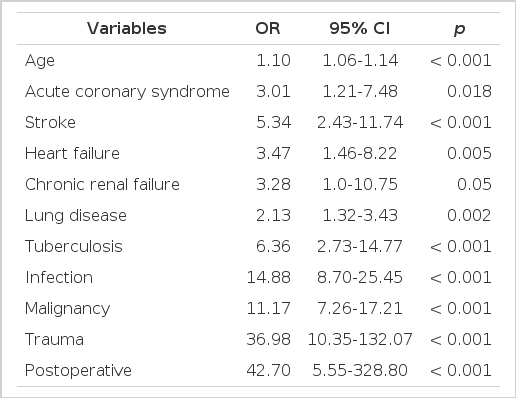
Multivariate analysis of the factors associated with a false positive D-dimer result
Cut-off value의 평가
폐동맥 색전증과 심부 정맥 혈전증의 선별을 위한 최적의 D-dimer의 값을 알아보기 위해 receiver-operating characteristic (ROC) curve를 이용하여 분석한 결과 cut-off value는 0.68 mg/L로 이때의 민감도는 95%, 특이도는 57%로 나타났다(Fig. 2). 그리고 65세를 기준으로 나누어 분석해 보았을 때, 65세 이하 환자들에서의 cut-off value는 0.58 mg/L로 민감도는 100%, 특이도는 71%였으며, 65세 초과 환자들에서의 cut-off value는 0.77 mg/L로 민감도는 89%, 특이도는 47%였다(Fig. 3).
The receiver operating characteristic (ROC) curve of D-dimer used to obtain the new cut-off value.
The receiver operating characteristic (ROC) curve of D-dimer used to obtain the new cut-off value divided by the age of 65 years.
고 찰
본 연구는 폐동맥 색전증과 심부 정맥 혈전증 선별을 위한 D-dimer 검사에서 위양성을 일으킬 수 있는 인자들을 확인하고, D-dimer 검사의 민감도와 특이도를 향상시킬 수 있는 새로운 cut-off value을 알아보기 위한 연구였다. 본 연구를 통해 연령의 증가, 외상, 수술의 기왕력, 급성 감염, 결핵, 뇌혈관 질환, 악성종양, 만성 신부전, 급성 관동맥 증후군, 심부전, 호흡기 질환 등이 D-dimer 검사의 위양성을 유발할 수 있는 예측인자로 관찰되었다. 또한 본 연구에서 D-dimer 검사의 cut-off value를 기존의 0.5 mg/L에서 0.68 mg/L로 하였을 때 민감도를 88%에서 95%로, 특이도를 48%에서 57%로 향상시킬 수 있었다.
이전 연구를 통해 연령이 증가함에 따라 D-dimer의 특이도가 유의하게 감소하는 것이 알려져 있고[3,4], 본 연구에서도 이전의 연구에서와 같이 연령이 증가함에 따라 D-dimer 양성률이 증가하는 결과를 보였다. 50대까지는 D-dimer 양성률이 32%로 연령에 따른 영향이 크지 않았으나 60대 50%, 70대 61%, 80대 이상에서는 90%의 환자에서 D-dimer가 양성으로 나타나 연령이 증가할수록 D-dimer의 양성률이 증가하는 경향을 보였다. 반면 진양성에 대한 위양성의 비율은 연령이 증가할수록(50대; 66.5, 60대; 17.8, 70대; 17.9, 80대 이상; 14.3) 감소되는 경향을 보였는데, 이는 연령이 증가할수록 폐동맥 색전증과 심부 정맥 혈전증의 발생률도 증가하기 때문으로 사료된다. 악성종양, 수술의 기왕력, 만성 폐질환, 울혈성 심부전, 뇌혈관 질환과 혈관염 등은 폐동맥 색전증을 유발하는 기저질환으로 알려져 있다[5,6]. 그러나 악성종양[7,8,12], 감염[12-14], 수술의 기왕력[15-17], 외상[12,18], 뇌혈관 질환[12,19-21], 허혈성 심질환[12,22-24] 등은 또한 폐동맥 색전증이나 심부 정맥 혈전증이 없이 D-dimer의 수치를 상승시키는 것으로 보고되었다. 특히 여러 연구에서 수술의 기왕력이 D-dimer의 위양성 결과와 관련이 깊은 질환으로 보고되고 있는데, 본 연구에서도 수술의 기왕력은 D-dimer 위양성과 가장 관련성이 높은 질환으로 나타나 기존의 연구들과 유사한 결과를 보여줬다. 또한 급성 감염병, 악성종양, 외상, 뇌혈관 질환 등의 질환에 대하여도 이전 보고된 연구 결과들과 마찬가지로 D-dimer 검사에서 위양성 결과와 관련이 있는 것으로 확인되었다. 반면, 본 연구에서는 호흡기 질환, 심부전이나 만성 신부전 특히, 우리나라에서 비교적 흔한 결핵균에 의한 감염도 D-dimer 검사에서 위양성 결과와 관련이 있는 것으로 확인되었다. 기존의 연구에서는 허혈성 심질환이 D-dimer의 상승과 관련이 있는 것으로 보고하였으나[22-24], 본 연구에서는 심혈관 질환 중에서 병태 생리학적으로 혈전의 생성이 관련되어 있다고 알려져 있는 급성 관동맥 증후군만이 D-dimer의 위양성과 관련되어 있는 것으로 나타난 것도 흥미로운 결과라고 생각한다. 이처럼 연령의 증가, 외상, 수술의 기왕력, 급성 감염, 결핵, 뇌혈관 질환, 악성종양, 만성 신부전, 급성 관동맥 증후군, 심부전, 호흡기 질환 등의 기저 질환이 있는 경우 D-dimer 검사가 위양성의 결과를 나타낼 가능성을 항상 염두에 두어야 할 것으로 생각한다.
본원에서 시행되고 있는 D-dimer 검사는 효소-연결면역흡수측정검사(enzyme-linked immunosorbent assay; VIDAS D-dimer exclusion)를 이용하여 혈청 D-dimer 농도 측정하고, 일반적으로 cut-off value 0.5 mg/L 이상일 때를 양성으로 한다. VIDAS D-dimer assay의 cut-off value를 0.5 mg/L로 하였을 때, 이전의 연구에서는 96-99%의 민감도와 38-40%의 특이도를 보였다[25,26]. 하지만 현재까지 국내에서는 실제 임상에서 폐동맥 색전증과 심부 정맥 혈전증이 발생한 환자를 대상으로 D-dimer의 결과치와 그에 따른 민감도와 특이도에 대해 보고된 연구가 없었다. 이에 저자들은 본 연구를 통하여 한국인에서 VIDAS D-dimer assay법에 의한 민감도와 특이도를 구하였다. D-dimer 검사의 cut-off value를 현재 사용되는 0.5 mg/L로 했을 때의 민감도는 88%, 특이도는 48%였고, 위양성률은 95%, 위음성률은 1%로 관찰되었다. 또한, 민감도와 특이도를 향상시킬 수 있는 D-dimer의 새로운 cut-off value을 ROC curve을 통하여 0.68 mg/L로 정하였고 이때 민감도는 95%, 특이도는 57%로 향상시킬 수 있었다. 그리고 65세를 기준으로 나누어 분석해 보았을 때, 65세 이하 환자들에서의 cut-off value는 0.58 mg/L로 민감도는 100%, 특이도는 71%였으며, 65세 초과 환자들에서의 cut-off value는 0.77 mg/L로 민감도는 89%, 특이도는 47%로 확인되었다.
본 연구는 후향적 연구로 단일기관의 결과이며, D-dimer 검사를 시행한 목적이 폐동맥 색전증과 심부 정맥 혈전증을 배제하기 위한 것이었음을 추측할 뿐 그 이유가 정확히 무엇이었는지 확인할 수는 없었으며, 각 환자들에서 폐동맥 색전증을 임상적으로 예측할 수 있는 Revised Geneva score나 Wells score를 확인하지 못하였고, cut-off value를 분석하기에는 폐동맥 색전증과 심부 정맥 혈전증을 진단받은 환자들의 수가 적었다는 제한점이 있었다. 결론적으로 폐동맥 색전증과 심부 정맥 혈전증을 선별하기 위하여 시행되는 D-dimer 검사는 연령의 증가, 외상, 수술의 기왕력, 급성 감염, 결핵, 뇌혈관 질환, 악성종양, 만성 신부전, 급성 관동맥 증후군, 심부전, 호흡기 질환 등이 있는 환자에서 검사의 위양성이 증가하게 되어 낮은 특이도를 나타내었다. 또한 현재 VIDAS D-dimer assay법에 사용되고 있는 cut-off value인 0.5 mg/L를 0.68 mg/L로 정하였을 때, 민감도 88%, 특이도 48%를 민감도 95%, 특이도 57%로 향상시킬 수 있었다. 따라서 임상에서 D-dimer 검사를 시행하고 적용할 때는 이러한 인자들이 결과치에 영향을 줄 수 있음을 충분히 고려하여야 하겠다.