한국인 자가면역성 간염을 진단하기 위한 Simplified Scoring Criteria의 가치 및 유용성
Diagnostic Value and Utility of the Simplified International Autoimmune Hepatitis Group (IAIHG) Criteria for Autoimmune Hepatitis in Korea
Article information
Abstract
목적:
자가면역성 간염(AIH)을 진단하기 위한 revised original scoring criteria는 지나치게 번거로워 임상에서의 적용이 쉽지 않았다. 이러한 단점을 보안하기 위해 2008년 Hennes 등[19]에 의해 simplified scoring criteria가 발표되었다. 이에 저자 등은 이 criteria를 한국인에게 적용하였을 경우, 진단적 가치 및 유용성을 평가하고자 연구를 시행하였다.
방법:
Original revised scoring criteria에 의해 AIH이 진단된 22예와 자가면역 간염/원발성담즙 간경변증(autoimmune hepatitis/primary biliary cirrhosis, AIH/PBC) 중복증후군을 진단받은 5예, 그리고 대조군으로 독성간염 50예, 비알코올성 지방간(NAFLD) 18예, 원발성담즙 간경변증(PBC) 11예를 후향적으로 분석하였다.
결과:
AIH 중 20명(90.9%)과 AIH/PBC 중복 증후군 5명 모두가 simplified scoring criteria에 의해 AIH로 진단되었다. 그리고 PBC 중 3명인 27.3%에서 새로운 진단기준을 적용하였을 경우 위양성을 보였다. AIH 진단에 대한 simplified scoring criteria의 민감도와 특이도는 각각 90.9%와 96.2%였다.
결론:
한국인에게 simplified scoring criteria는 중복증후군을 포함한 자가면역성 간염을 진단하는 데 유용하게 사용될 수 있을 것으로 생각한다.
Trans Abstract
Background/Aims:
The diagnostic criteria for autoimmune hepatitis (AIH) were created and revised by the InternationalAutoimmune Hepatitis Group (IAIHG) in 1999. Simplified scoring criteria based on four clinical components were recentlyproposed. The aim of this study was to assess the diagnostic value and usefulness of these simplified criteria in Korea.
Methods:
We applied the simplified scoring criteria to 22 AIH patients diagnosed according to the original revised scoring criteriaproposed in 1999. Furthermore, in order to compare the predictive power of these two sets of diagnostic criteria, we included 84patients with liver diseases [toxic hepatitis (n = 50), nonalcoholic fatty liver disease (n = 18), primary biliary cirrhosis (PBC) (n = 11), and PBC/AIH overlap syndrome (n = 5)] other than AIH.
Results:
Twenty (90.9%) patients with AIH and five (100%) with PBC/AIH overlap syndrome were diagnosed with AIHaccording to the simplified scoring criteria. Three (27.3%) patients with PBC were false-positive for AIH according to thesimplified scoring criteria. Those patients diagnosed according to the simplified scoring criteria showed an increased frequency ofANA and/or SMA of ≥ 1:80 (p= 0.491) and an increased frequency of serum IgG levels at or above the upper normal limitcompared to patients with PBC (p= 0.006). The sensitivity and specificity of the simplified scoring criteria for the diagnosis of AIHwere 90.9 and 96.2%, respectively.
Conclusions:
The simplified scoring criteria offer a reliable and simple method for excluding AIH; however, these criteria mayhave limitations in the diagnosis of patients with atypical features, especially those with low autoantibody and IgG levels. (Korean J Med 2011;81:340-350)
서 론
자가면역 간염(autoimmune hepatitis, AIH)은 계면간염(interface hepatitis)을 특징으로 하는 만성 간염 형태의 조직 소견과 혈청 내 자가 항체의 존재, 고감마글로불린혈증, 그리고 면역억제제 투여 후 호전을 특징으로 하는 만성 간질환이다[1]. 1950년대 초 Waldenström에 의해 처음 증례가 보고된[2] 이후 연평균 북유럽 백인 10,000명당 1.9명에서 발생하고[3], 전체 간이식의 2.6-5.5%를 차지하는 것으로 알려져 있다[4]. 우리나라의 경우 알코올성 간질환을 제외한 만성 간질환 중 B형 및 C형 바이러스 간염이 80-90%로 대부분을 차지하고 있다. 따라서 자가면역 간염에 대한 관심도는 상대적으로 낮은 상태이며, 현재까지 정확한 국내 발병률도 조사되지 않은 상태이다. 자가면역 간염은 주로 여성에서 호발하고[5] 전 연령층에서 발병할 수 있다[6]. 대부분은 서서히 발병하지만 약 40%는 급성 발병을 보이며[7] 전격 간염으로 발현하기도 한다[8]. 또한 1/3에서는 증상이 없고[9], 성인 환자 중 30%는 진단 당시 간경변이 동반되어 있다[10]. 증상의 유무는 염증의 정도 및 간경변 동반과 관련이 없으며, 경한 상태라 하더라도 15년 내 49%에서는 간경변이 동반되고 10%는 간부전으로 사망할 수 있다. 따라서 질환의 만성 여부를 확인하기 위해 6개월 정도를 기다리는 것은 불필요한 과정이다[11]. 그러나 자가면역 간염은 특이적인 진단 검사법이 없고[12], 비교적 특징적인 소견으로 알려진 자가 항체가 다른 간 질환에서도 발견될 수 있기 때문에 다른 원인의 비알코올성, 비바이러스성 간질환과의 감별이 쉽지 않다[13-15]. 이에 1993년 IAIHG (International Autoimmune Hepatitis Group, IAIHG)은 자가면역 간염의 진단을 위해 최소 필요 지표(minimum required parameter)와 조직 검사 결과 및 치료 후 반응에 따른 추가 지표(additional parameter)를 이용한 점수 체계(scoring system)을 제시하였고[16], 이후 1999년 개정된 점수 체계(original revised scoring criteria)를 발표하였다(Table 1) [17]. 이 점수 체계는 15개 항목을 평가하여 의증(probable)과 확진(definite)으로 자가면역 간염을 진단하며 담즙정체 간질환을 확실히 배제하기 위해 alkaline phosphatase (ALP)/aspartate aminotransferase (AST) 비 및 조직소견의 중요성을 부각시켰고, 항미토콘드리아항체(antimitochondrial antibody, AMA) 양성과 약제 복용력이 있을 때 감점의 폭이 가장 컸다. 그러나 개정된 진단체계는 지나치게 번거로워 임상에서의 적용이 쉽지 않으며, 진단을 위해 조직검사 결과와 치료 반응이 모두 포함되어야 하기 때문에 어떤 환자에게 간 조직검사와 면역 억제제 투여를 시도해야 하는지 적응증을 제공하지 못한다는 단점이 있다. 또한 전반적인 특이도가 98.1%로 향상된 것에 비해, 다른 간질환이 동반되어 있거나, 자가면역 간염 중복 증후군(AIH overlap syndrome)일 경우, 민감도가 66.7%와 50%로 낮아지는 현상을 보였다[18].
Original revised scoring criteria for the diagnosis of AIH
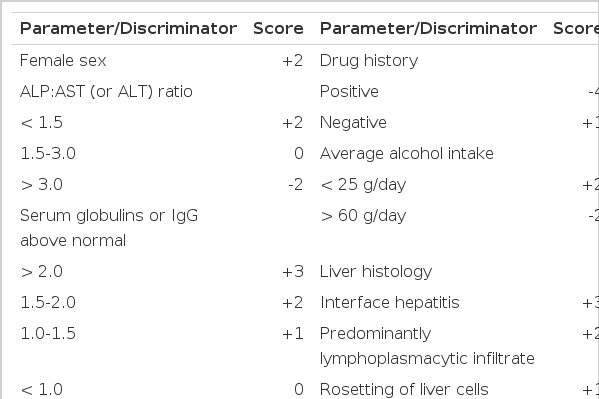
이를 보완하기 위해 2008년 Hennes 등[19]은 자가항체 소견, 면역글로불린 G (Immunoglobulin G, IgG), 간 조직검사 소견, 바이러스성 간염 여부의 네 가지 기준만으로 구성된 simplified scoring criteria을 제시하였다(Table 2). 당시 저자들은 의증(probable)의 경우 진단의 민감도와 특이도를 각각 88%와 97%로, 확진(definite)일 경우 81%와 99%로 보고하였다.

Simplified scoring criteria (2008)
자가면역 간염은 인종에 따라 발현양상이 매우 다양하나[20,21] 우리나라의 경우 2004년 172명의 환자를 대상으로 한 현황보고 외에는 대규모 연구가 시행된 바 없어 서구에서 제시된 진단 체계를 한국인에게 그대로 적용 가능한지 알 수 없는 상태이다. 이에 본 연구에서는 simplified scoring criteria를 한국인에게 적용시켰을 때 진단적 가치 및 유용성을 평가, 비교하고 진단 체계의 간소화에 의해 발생할 수 있는 문제점을 확인하고자 하였다.
대상 및 방법
연구 대상
환자군
2002년 2월부터 2010년 5월까지 순천향대학교 부천병원에서 간 조직 검사를 시행 받은 제1형 자가면역 간염 22예와 자가면역 간염/원발성담즙 간경변증(autoimmune hepatitis/primary biliary cirrhosis, AIH/PBC)이 함께 존재하는 중복 증후군(overlap syndrome) 5예를 후향적으로 분석 하였다. 제1형 자가면역 간염의 경우 치료 전 original revised scoring criteria를 적용하여 진단하였고, AIH/PBC 중복 증후군은 PBC의 세 가지 진단 기준인 1) ALP가 정상 상한치의 2배 이상이거나 gamma-glutamyl transpeptidase (GGT)가 정상 상한치의 5배 이상인 경우, 2) 항미토 콘드리아항체(antimitochondrial antibody, AMA) 양성, 3) 전형적인 간 조직검사 소견(florid bile duct lesion) 중 두 가지를 만족하고, 자가면역성 간염의 세 가지 진단 기준인 1) ALT가 정상 상한치의 5배 이상, 2) IgG가 정상 상한치의 2배 이상이거나 항평활근항체(antibody to smooth muscle, SMA) 양성, 3) 전형적인 간 조직검사 소견(계면간염 등) 중 두 가지 이상을 만족한 경우로 진단하였다[22].
연구 방법
모든 환자군과 대조군의 성별, 나이, 알코올의 남용력, 동반된 자가면역질환, 약물 복용력은 의무기록의 후향적 검토를 통해 확인하였다. 그 외 점수 체계에 필요한 변수인 병리소견과 항핵항체(antinuclear antibody, ANA), SMA, AMA, IgG, ALP, 총 빌리루빈(bilirubin), AST, alanineamino-transferase (ALT), HBsAg, anti-HCV를 조사하였고, 이를 바탕으로 original revised scoring criteria (Table 1)와 simplified scoring criteria (Table 2)를 이용하여 집합 점수를 산출하였다. 항핵항체와 항평활근 항체, 항미토콘드리아항체 경우 역가 1:40 이상을 양성으로 하였다.
통계 분석
측정된 모든 자료는 평균과 범위로 표시하였고, 통계 분석은 SPSS version 12.0 프로그램을 이용하였다. 기술통계와 교차분석을 통하여 결과를 도출하였으며, 연속 변수에 대한 군간의 비교는 Kruskal-Wallis test를 사용하였고, 비연속 변수의 군간 비교는 chi-sqaure test 및 Fisher's exact test를 사용하였다. 이때 p 값이 0.05 미만인 경우를 의미 있는 것으로 판단하였다.
결 과
대상 환자의 임상적 특성
총 106명의 환자 중 남자가 30명(28.3%), 여자가 76명(71.7%)이었고, 평균 연령은 46.1세(18-73세)였다. 모든 환자는 바이러스성 간염이 배재된 상태였고, 하루 60 g 이상의 음주력이 있는 환자는 독성간염을 진단받은 2명에서 관찰되었고, 25 g 이상, 60 g 미만의 음주력은 독성간염을 포함해서 2명이 확인되었다. 독성 간염을 제외한 환자군에서 간독성이 있을 것으로 생각되는 약물 복용력은 자가면역 간염 환자 중 3명(13.6%) 외에 없었다. 자가면역성 간염 환자군의 진단 당시 평균 연령은 45.8세(28-66세)였고 남녀 비는 1:21였다. IgG는 자가면역성 간염군에서 2,478 mL/dL로 다른 질환군에 비해 유의하게(p< 0.01) 높았고, ANA는 자가면역성 간염 환자의 90.5%, AIH/PBC 중복 증후군의 100%에서 양성이었으며 PBC 72.7%, NAFLD 36.8%, 독성간염 30%에서 양성을 보였다(p< 0.01, Table 3).

Baseline characteristics and scores by the original revised scoring and simplified scoring criteria of the patients
Simplified scoring criteria의 sensitivity와 specificity
Original revised scoring criteria에 의해 AIH가 진단된 22명의 환자 중 simplified scoring criteria을 적용하였을 때, 2명(9.1%)이 6점 미만으로 진단에서 제외되었다. 대조군 중 PBC에서 1명(9.1%)이 확진으로, 2명(18.2%)이 의증으로 진단되었고, 그 외 독성간염과 NAFLD 환자는 모두 simplified scoring criteria 적용 시 음성 소견을 유지하였다(Table 4). Original revised scoring criteria에 의해 AIH가 진단된 환자를 기준으로 산출한 simplified scoring criteria의 민감도(sensitivity)와 특이도(specificity)는 확진을 기준으로 할 때 77.3%와 98.7%였고, 의증 이상일 경우 각각 90.6%와 96.2%로 확인되었다(Table 5).
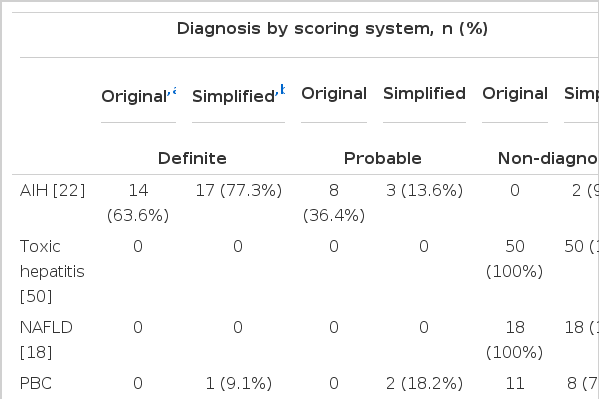
Comparison of scoring diagnoses using each system

Sensitivity and specificity of the simplified scoring criteria for the diagnosis of AIH (n = 22)
자가면역성 간염
자가면역성 간염 환자 중 simplified scoring criteria 적용 시 2명(9.1%)은 의증에서 음성으로, 2명(9.1%)은 확진에서 의증으로 진단이 하강하였으며 5명(22.7%)의 환자는 의증에서 확진으로 진단이 상승하였다. 통계적으로 유의하지는 않으나 두 군 중 진단이 하강한 군에서 ALP/AST 비가 2.6으로 진단이 상승된 군의 1.8보다 높은 경향을 보였고, ANA가 1:80 이상으로 증가된 환자가 50%, IgG가 정상 상한지 보다 1.1배 이상 증가된 환자가 25%로 진단이 상승된 군의 100%와 60%에 비해 낮은 경향을 보였다(Table 6).

Comparison of demographic, laboratory, and clinical variables between down- and up-graded patients by simplified scoring criteria
PBC
PBC 환자 중 simplified scoring criteria에서 위양성을 보인 군과 지속적으로 진단에서 배제된 군을 비교하였을 때 위양성 군은 모두 ANA가 양성이었고, 나머지 PBC 군은 62.5%에서 양성이었다(p= 0.491). IgG의 경우 정상 상한치보다 1.1배 이상으로 증가되어 있는 경우가 위양성 군은 100%였으나 지속적으로 음성을 보인 환자군에서는 관찰되지 않아 위양성군에서 유의하게 높았다(p= 0.006). 자가면역성 간염을 시사하는 조직학적 소견(p= 1.00)과 담관 변화 소견(p= 0.727)의 유무에는 통계학적으로 유의한 차이가 없었다(Table 7).

Comparison of demographic, laboratory, and clinical variables at presentation between false-positive and true-negative cases of PBC as ascribed by the simplified scoring criteria
AIH/PBC 중복증후군
AIH/PBC 중복증후군의 ALP/AST 비는 평균 3.4로 자가면역성 간염의 1.0보다 유의하게 높았다(p= 0.039). 중복증후군 환자는 5명(100%) 모두가 AMA 양성이었고, PBC에 합당한 조직학적 소견을 보이고 있었다. IgG가 정상 상한치의 1.1배 이상 증가되어 있는 경우는 중복증후군 2명(40%), 자가면역성 간염 13명(59.1%)에서 관찰되었으나 유의하지 않았고(p= 0.628), 자가면역성 간염을 시사하는 조직학적 소견은 각각 95.5%와 100%에서 관찰되고 있었다(Table 8).

Comparison of clinical and scoring diagnoses using the original revised scoring criteria and simplified scoring criteria
고 찰
2008년 자가면역성 간질환에 대한 새로운 진단 기준이 제시된 이후 Czaja 등은 검정과정을 통해 simplified scoring criteria가 95%의 민감도와 90%의 특이도를 가진다고 보고한 바 있다[22]. 이는 이전 진단 기준의 민감도인 95%보다는 다소 낮지만 특이도를 73%에서 90%까지 향상시킨 결과이다. 1999년 진단기준에 포함된 ALP/AST 비, IgG, ANA 수치, 조직검사 결과에 부여된 차등적인 점수 체계는 질환의 특성과 함께 정도가 반영되기 때문에 원인 미상의 간염이 자가면역성 간염으로 진단될 가능성이 있었다. 이러한 단점을 보완하기 위해 새로운 진단기준에서는 자가면역성 간질환에 특이적인 네 가지 검사 항목만을 포함하여 기준을 마련하였고 이러한 변화는 특이도를 향상시키는 결과를 보여 주었다. 그러나 simplified scoring criteria는 지나치게 기준이 간소화 되어 각각의 항목이 진단에서 차지하는 비중이 높아, 발병 양상이 비특이적일 경우 진단에서 누락될 가능성이 있다. 실제로 Alvarez 등[17]은 자가면역 간염 중 ANA, SMA, 항간신마이크로좀 1 항체(antibody against liver-kidney microsome 1, anti-LKM1)가 모두 음성인 경우를 약 20%까지 보고하였으며, Jung 등[25]의 연구에서도 제 1형 자가면역성 간염 환자 26명 중 80.8% 만이 자가 항체 양성이면서 고감마글로불린 혈증이 함께 있었다. 따라서 자가면역 간염 환자 중 자가항체가 음성이거나, 감마글로불린의 수치가 높지 않을 경우 simplified scoring criteria를 통해 진단이 불가능할 수 있다. 본 연구에서도 자가 면역성 간염 환자 22명 중 2명(9.1%)이 새로운 진단 기준에서 위음성을 보였고, 이전 진단기준에서 확진을 보였던 2명(9.1%)의 환자가 새로운 진단기준에서 의증으로 하향되었다. 새로운 진단기준 적용 시 의증에서 확진으로 변화된 환자 5명(22.7%)과 앞의 4명의 환자를 비교해 보았을 때 진단이 하향된 군에서 ANA가 1:80 이상인 경우가 50%로 진단이 상향된 군의 100%보다 낮았다. 또한 IgG가 정상상한치의 1.1 이상인 환자도 25%로 진단이 상향된 군의 60% 보다 낮은 비율을 보였다. 이러한 결과는 통계학적으로 유의하지는 않았으나 ANA와 IgG의 역가가 비교적 높지 않은 자가면역성 간염에서 simplified scoring criteria 적용 시 위음성이 증가할 수 있음을 예측할 수 있는 소견이다.
1993년 처음 발표된 IAIHG의 점수 체계는 97-100%의 민감도를 보였지만 의증 환자의 8-52%가 자가면역성 담관염과 같은 담즙정체간질환이었기 때문에 낮은 특이도를 보였다[18,26-28]. 이를 보완하기 위해 1999년 개정 시, ALP/AST 비를 추가하였고, 조직검사 소견에서 담관 변화를 보이는 경우 감점을 하였다. 그러나 ALP/AST 비는 대부분의 만성 간질환이 담즙울체형 간손상을 보이지 않기 때문에 자가면역성 간염을 PBC이나 원발경화 담관경화(primary sclerosing cholangitis, PSC)로부터 구별하는 데에는 도움이 되지만 자가면역양상을 동반한 담즙울체형 간질환과의 감별에 있어서는 취약하다[29]. 따라서 중복증후군의 경우 ALP/AST 비가 순수 자가면역성 간염에 비해 높고 조직검사에서도 담관변화를 동반하기 때문에 진단의 민감도가 50%로 감소하게 되었다[18]. 이를 반영하여 Hennes 등[19]은 중복증후군을 자가면역성 간질환으로 분류하여 simplified scoring system을 제시하였다[19]. 물론 일부 중복 증후군이 시간이 경과함에 따라 순수 자가면역성 간질환과는 전혀 다른 양상으로 진행할 수 있기 때문에[30] 이러한 분류에 논란이 없는 것은 아니다. 그러나 중복증후군이 활동성의 자가면역성 간염을 동반할 경우 PBC나 PSC 유무와 관계 없이 치료를 요한다는 점을 고려하여 진단체계를 구성하였고, 그 결과 본 연구에서도 5명의 AIH/PBC 중복증후군 환자가 1999년 진단체계에서는 모두 위음성이었으나 simplified scoring criteria을 적용하였을 때 자가면역성 간염으로 진단되고 있었다(Table 8). 중복증후군 환자는 순수 자가면역성 간염 환자에 비해 ALP/AST 비가 3.4 (p= 0.039)로 유의하게 높았고, 조직검사에서 담관변화를 보인 경우도 유의하게(100%, p= 0.01) 많았다. 또한 AMA도 모두에서 양성을 보여 순수 자가면역성 간염군(0%, p< 0.001)보다 유의하게 높았다. 그러나 ANA나 IgG, 자가면역성 간염을 시사하는 조직소견에서는 유의한 차이를 보이지 않았다. 이러한 결과를 통해 ALP/AST 비, 조직검사에서의 담관변화 및 AMA 항목이 1999년 진단 체계에서 중복증후군의 자가면역성 간염 진단의 민감도를 감소시킨 주 요인임을 확인할 수 있었다.
Simplified scoring criteria가 제시된 이후 발표된 검정결과 중 Czaja 등[22]은 새로운 진단 기준의 민감도와 특이도를 95%와 90%로 발표하였고, Yeoman 등[31]의 연구에서는 90%와 98%로 발표한 바 있다. 본 연구에서 측정된 simplified scoring criteria의 민감도는 90.9%였으며 특이도는 96.2%로 이전에 발표된 내용들에 준하는 결과를 보여 주었다. 이 중 민감도를 감소시킨 요인은 2명의 자가면역성 간질환이 위음성으로 진단되었기 때문이었고, 이들은 앞에서 설명한 바와 같이 ANA와 IgG가 낮은 비특이적인 양상의 환자들이었다. 특이도에는 PBC 환자 11명 중 위양성을 보인 3명(27.3%)이 영향을 주었다. 이들 중 2명은 의증이었고, 1명은 확진으로 분류 되었다. 전체 PBC 환자 11명 중 8명(72.2%)에서 ANA가 1:80 이상 증가되어 있었고, 3명(27.3%)에서 IgG가 정상 상한치의 1.1 이상 증가되어 있었다. 이 세 명의 환자는 모두 ANA가 80 이상이었고, 바이러스성 간염이 배제되어 simplified scoring criteria 적용 시 자가면역성 간염으로 진단되었다. 이러한 결과는 ANA와 IgG의 비특이성 때문이다. ANA의 경우 PBC, PSC, 약인성 간손상, 바이러스간염, 알코올, NAFLD 등 여러 간질환에서 검출되며, 정상 성인에서도 15%까지 양성으로 보고된다[32-34]. 또한 Jung 등[25]의 연구에 따르면 만성간질환의 50% 이상에서 IgG가 정상 상한치 이상으로 상승되어 있었고, 본 연구에서도 독성간염 환자 중 2명(4.0%), NAFLD 중 2명(11.1%)에서 같은 결과를 보였다. 이러한 비특이성은 simplified scoring criteria을 만든 의도와는 다르게 원인 미상의 간염을 자가면역성 간염으로 오진할 수 있는 원인이 될 수 있다. 그러나 PBC 일부가 위양성으로 진단된 데에는 검사의 비특이성과 함께 중복증후군의 가능성도 고려되어야 한다. 현재 중복 증후군은 아직까지 진단방법이 표준화 되어 있지 못하며, 흔히 사용되고 있는 Paris criteria [21]의 경우 Kuiper 등[35]에 의해 이루어진 후향적, 단일기관 연구를 통해 각각 92%와 97%의 민감도와 특이도가 보고 되었지만, 적절성을 입증하기 위한 더 많은 연구가 필요한 상태이다. 따라서 위양성을 보인 PBC 환자들이 비록 Paris criteria를 만족하지는 않았지만 중복증후군의 가능성이 완전히 배제된 것은 아니며, 이러한 양상을 보이는 환자에서는 지속적으로 자가항체와 면역글로불린 등에 대한 추적 검사가 필요할 것이다.
결과적으로 한국인에게 simplified scoring criteria는 자가면역성 간염을 진단하는 데 매우 유용하게 사용될 수 있으며, 특히 중복증후군의 진단에 많은 향상을 가져다 주었다. 그러나 진단 항목의 간소화는 비특이적 양상의 자가면역성 간염을 진단하지 못할 가능성이 있으며, 또 이 항목들이 자가면역성 간염에 대한 특이도가 낮기 때문에 위양성을 초래할 위험성이 있다. 특히 자가 항체나 면역글로불린이 의미 있게 상승한 경우 면밀한 추적관찰을 시행하고, 자가면역성 간질환의 다양한 임상경과를 이해하는 것이 중요할 것으로 생각한다. 본 연구에는 대조군에 비알코올성 간질환 중 가장 많은 비율을 차지하는 바이러스성 간염 환자가 포함되어 있지 않다는 점과 단일기관에서 시행되었다는 제한점이 있다. 따라서 한국인에서 simplified scoring criteria의 진단적 가치 및 유용성을 평가하기 위해 더 다양하고 많은 환자를 대상으로 한 대규모 연구가 필요할 것으로 생각한다.