식도와 위기능 장애가 동반된 만성 가성 장폐쇄증 1예
A Case of Chronic Intestinal Pseudo-Obstruction with Esophageal and Gastric Dysfunction
Article information
Abstract
반복적인 복통과 구토를 주소로 내원하여 임상증상과 병력, 고해상도 식도내압검사와 위배출 시간 검사를 통하여 식도와 위기능 장애가 동반된 소장의 만성 특발성 가성 장폐쇄증으로 진단되었고, 보존적 치료로 호전된 비교적 경한 증상의 증례이다.
Trans Abstract
Chronic intestinal pseudo-obstruction (CIPO) is a rare digestive syndrome characterized by symptoms and signs of intestinal obstruction in the absence of mechanical obstruction. A 48-year-old female presented at our facility with severe abdominal pain and vomiting. Simple abdominal radiography revealed small bowel gas and ileus. Computed tomography also revealed a dilated small bowel, but there was no evidence of mechanical obstruction. Esophageal function was decreased based on high-resolution manometry and the gastric emptying time was prolonged on a gastric emptying scan. The patient recovered with conservative treatment. We report a case of chronic intestinal pseudo-obstruction with esophageal and gastric dysfunction. (Korean J Med 2011;81:223-228)
서 론
만성 가성 장폐쇄증(chronic intestinal pseudo obstruction syndrome)은 기계적 폐쇄없이 복부팽만과 복통과 같은 임상적 증상이 반복적으로 나타나면서 방사선 소견에서는 장폐쇄 소견을 보이는 드문 증후군이다[1,2]. 이 질환은 원인 여부에 따라 특발성과 이차성으로 나뉘며 특발성은 내장 근병형(visceral myopathy)과 내장 신경병형(visceral neuropathy)로 구분되고, 대부분이 이차성으로 특발성은 아주 드문 것으로 알려져 있다[3]. 현재까지 국내 문헌에 의하면 만성 특발성 가성 장폐쇄증은 3예[4-6]가 보고되었다. 저자들은 반복적인 복통과 구토를 주소로 내원하여 식도와 위기능 장애가 동반된 소장의 만성 특발성 가성 장폐쇄증으로 진단된 증례를 경험하였기에 보고하는 바이다.
증 례
48세 여자 환자가 내원 일주일 전부터 악화된 복통과 오심, 구토를 주소로 내원하였다. 환자는 20년 전부터 간헐적으로 식후 악화되는 복통이 반복되었으나 보존적 치료 후 증상이 호전되어 특별한 검사나 치료는 받지 않았다. 한달에 한 두 번 증상이 발생하였고, 여러 병원을 다니며 대증치료를 받으면서 악화와 호전을 반복해 왔다. 일주일 전부터 다시 오심과 구토를 동반한 심한 통증이 있어 타병원을 방문하여 대증치료를 하였으나 이번에는 증상이 호전되지 않고 더 악화되어 본원 응급실에 내원하였다. 과거력에서 20여 년 전 제왕절개 수술력이 있고, 가족력에서는 특이소견 없었으며, 흡연과 음주력은 없었다.
내원 당시 혈압은 130/70 mmHg, 맥박 72회/분, 호흡수 20회/분, 체온 36.4℃였다. 흉부 청진에서 심음과 폐음은 정상이었고, 복부진찰에 복부는 부드러웠으나 팽창되어 있었고, 장음은 감소되어 있었다. 종괴는 촉지되지 않았고, 약간의 압통은 있었으나 반사통은 보이지 않았다.
검사실 소견은 말초혈액 검사에서 백혈구 6,600/mm3, 혈색소 12.2 g/dL, 혈소판 244,000/mm3, 생화학검사에서 공복혈당 88 mg/dL, BUN 5 mg/dL, Cr 0.6 mg/dL, total protein 6.8 g/dL, albumin 4.2 mg/dL, AST 20 IU/L, ALT 14 IU/L, alkaline phosphatase 37 IU/L, γ-GTP 29 mg/dL, total bilirubin 1.0 mg/dL, LDH 282 IU/L, sodium 139 mEq/L, potassium 3.3 mEq/L, CEA 0.52 ng/mL, CA19-9 6.31 U/mL이었다. 갑상선 기능검사에서는 TSH 0.389 μIU/mL, freeT4 1.21 ng/dL, T3 108.02 ng/dL로 정상이었다. 자가면역 항체 검사에서 ANA negative, P-ANCA negative, C-ANCA negative, cryoglobulin negative, rheumatoid factor 1 IU/mL, ASLO 43.9 IU/mL였다.
심전도는 정상이었으며, 흉부 X-선 검사에서 심장음영은 정상이었으나 우상부 폐야에 작은 석회화가 관찰되었고, 비특이적 소견으로 판단되었다. 내원 당시의 단순 복부 촬영상 소장이 공기로 확장된 저명한 장폐색 소견이 보였다(Fig. 1). 내원 당일 검사한 복부 전산화 단층 촬영에서는 가스로 확장된 소장이 보였으나, 장폐색을 일으킬만한 병변은 보이지 않았다(Fig. 2). 내원 3일째 시행한 상부 위장관 내시경 및 대장 내시경과 내원 7일째 시행한 소장 조영술에서 특이소견 없었다.
The simple abdomen X-ray showed a large amount of small bowel gas and an ileus pattern.

Computed tomography showed gas filling the small bowel loops and fecal stasis without evidence of mechanical obstruction.
환자는 금식, 비위관 삽입과 수액공급 등의 보존적 치료 후 증상이 호전되었고, 내원 4일째부터 식이를 시작하였다. 식후 더부룩한 느낌은 있으나 통증은 없었고, 단순 복부 촬영상 더 이상 장폐쇄의 소견은 보이지 않았다. 환자의 병력과 검사소견들을 기초하여 비교적 경한 만성 특발성 가성 장폐쇄로 진단하였고, 실제로 위장관 기능의 저하가 있는지 확인하기 위하여 추가검사를 시행하기로 하고 내원 10일째 퇴원하였다.
고해상도 식도내압검사를 시행한 후 퇴원하였고, 검사결과에서 연동실패(failed peristalsis)가 67%로 경한 연동운동 저하(mild peristaltic dysfunction)를 보였고, 4 sec Integrated relaxation pressure (IRP)가 18.9 mmHg로 증가되어 있고, contractile front velocity (CFV)는 2.3 cm/sec, distal contractile integral (DCI)는 2,205.7 mmHg/cm.sec이고 maximal intrabolus pressure (IBP)는 13.6 mmHg로써 하부식도괄약근 이완 기능저하(LES relaxation dysfunction)를 보이고, Chicago 분류[7]에 의하여 기능적 위식도접합부폐색(functional esophagogastric junction obstruction)으로 진단하였다(Fig. 3). 퇴원 후 5일째 위배출 시간(gastric emptying time) 검사에서 위 배출 반감기(half gastric emptying time, t1/2)가 128분으로 지연되어 있었다(Fig. 4). 환자는 현재 외래에서 경과관찰 중이다.
High-resolution esophageal manometry showed frequent peristaltic failure after swallowing.
The gastric emptying time was prolonged; the 50% emptying time was about 128 min.
고 찰
만성 가성 장폐쇄 증후군은 만성적인 복부 팽만과 구토 등 장폐쇄의 증상을 보이나 기계적인 원인을 찾을 수 없는 매우 드문 질환군이다. 이 용어는 임상에서 흔히 사용하지 않으므로 사용할 때 그 정의가 정확하지 않으면 그 의미가 잘 전달되지 않으므로 진단기준을 정리해야 할 필요가 있다. 먼저 분명한 장폐쇄의 증상이 있어야 하고, 방사선 검사에서 수평기류 소견이나 장폐쇄의 소견이 반드시 있어야 한다[1]. 만성 가성 장폐쇄의 경우 만성이란 선천적인 경우에는 생후 2개월 이상 병변이 지속될 때, 후천성인 경우에는 6개월 이상 병변이 지속될 때를 말한다[8]. 이 질환은 원인에 따라 특발성과 이차성으로 나뉘며 대부분은 가성 장패쇄를 유발하는 전신질환이 존재하는 이차성이다. 이차성을 유발할 수 있는 질환들은 표 1에 나타내었다[1]. 특발성은 뚜렷한 연관 질환이 없는 경우로, 병리 형태에 따라 근육층의 위축이나 변성, 섬유화를 보이는 내장 근병증(viceral myopathy)과 신경절 세포의 수가 감소 또는 증가되거나 형태의 이상을 보이는 내장 신경병증(visceral neuropathy)으로 분류한다[9,10]. 현재까지 국내에 보고된 만성 특발성 가성 장폐쇄증은 3예와 본 예의 임상상을 표 2에 요약하였다. 앞의 3예는 모두 수술을 통하여 진단하였으나 본 예에서는 병력과 검사결과만을 통하여 진단하였다. 이차성을 배제하기 위하여 시행한 갑상선 기능검사와 자가면역항체 검사는 모두 정상이었다. 과거력상 20여 년 전 제왕절개를 한 병력이 있어 그로 인한 장의 유착 가능성을 완전히 배제할 수는 없으나 환자는 통증이 그 전부터 있어 왔다고 하며, 실제로 고해상도 식도내압 검사와 위배출 시간 검사에서 식도와 위의 기능이 떨어져 있어 이상의 소견들로 수술을 하지 않고 특발성 가성 장폐쇄로 진단할 수 있었다. 그러나 이는 환자의 기억에 의존한 병력이므로 실제로 제왕절개로 인한 증상일 가능성이 있으며, 환자가 의료진에게 항우울제와 같은 약물 복용력을 말하지 않았을 가능성이 있다.
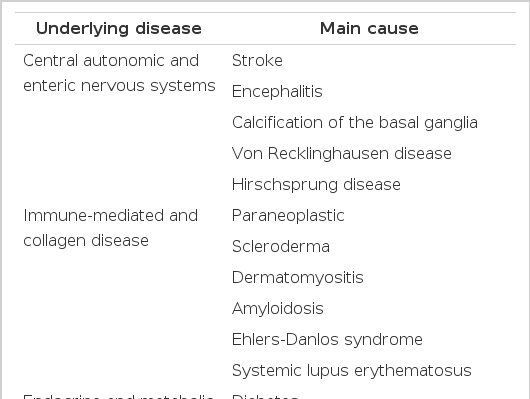
Causes of secondary chronic pseudo-obstruction
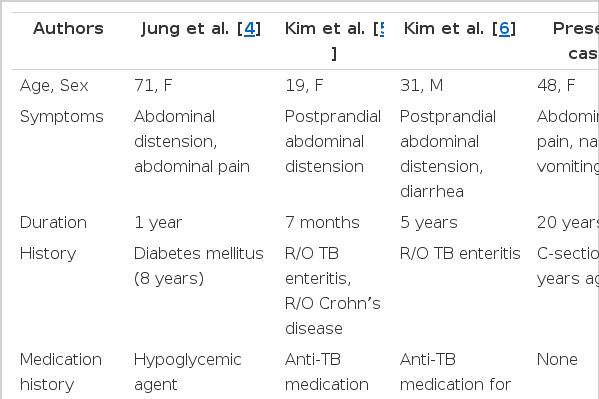
Summary of patients with chronic idiopathic intestinal pseudo-obstruction syndrome reported in Korea
만성 가성 장폐쇄증의 가장 흔한 증상은 복통(80%), 구토(75%), 변비(40%), 설사(20%)순으로 나타난다[11]. 이 질환은 위장관의 어떤 부위도 침범할 수 있고 침범부위에 따라 다른 증상이 나타나는데, 소장이 침범된 경우는 구역이나 구토를 호소하는 경우가 많고, 위장의 기능이상을 동반하는 경우도 있다. 소장의 세균증식이 이차적으로 발생하는 경우에는 설사를 호소하는 경우도 있으나 주로 변비를 호소한다. 식사를 하면 복부가 더 팽만되므로 환자들은 음식을 거부하게 되고 영양 결핍 상태가 되어 있는 경우가 많고, 드물지만 장의 천공이 일어나 열이 나는 증상을 주소로 내원할 수 있다[12]. 이러한 증상들은 흔한 다른 질병들의 증상과 비슷하므로 종종 다른 질환으로 오진될 수 있어 환자들은 처음에 정확한 진단을 받지 못하고 진단까지 상당한 기간이 소요되는 경우가 있다. 본 증례의 환자도 20여 년의 오랜 기간동안 증상이 있어 왔으나 비교적 증상이 경미하고 비특이적이며 보존적 치료로 호전되는 경과를 보여 진단이 늦어졌다.
만성 가성 장폐쇄 환자의 치료는 매우 어려운 경우가 많다. 이차적으로 발생한 경우는 근본 질환을 치료하면서 호전되는 경우가 많으나 특발성인 경우는 치료가 쉽지 않다. 금식을 하고 경정맥 영양공급을 하면서 경과관찰을 할 수 있는데 영양부족이나 전해질 불균형에 빠지지 않도록 해야 한다. 약물치료에 사용되는 약제는 크게 장운동을 활성화시키는 prokinetics, 소장세균증식증(SIBO, small bowel bacterial overgrowth)이 있을 경우에 사용되는 항생제, 염증성 신경병증(inflammatory neuropathy)에서 사용되는 약제로 분류할 수 있다. 먼저 prokinetics로는 cisapride나 tegasterod 같은 5-HT receptor agonist, erythromycin과 같은 motilin receptor agonist, somatostatin analogues 등이 있다[13]. 특히 neostingmine과 같은 cholinesterase inhibitor가 만성 가성 장폐쇄증에서 가장 좋은 약물로 보고되고 있는데, 국내에서도 보존적 치료에 반응하지 않는 환자에서 neostigmine을 투여하여 뛰어난 효과를 보인 경우가 보고되어 있다[14]. Erythromycin과 somatostatine analogues 병합요법으로 장운동을 항진시키고 구역질과 복통을 감소시켰다는 보고도 있다[15]. SIBO가 의심되는 경우 흡수되지 않는 항생제인 rifaximin이 효과가 있는 것으로 보고되어 있으며[16] 경구투여가 힘들 경우 quinoline 또는 metronidazole을 주사로 투여하는 것이 권장된다. 염증성 신경병증(inflammatory neuropathy or myenteric ganglionitis)이라는 드문 질환일 경우 면역억제제나 스테로이드제제의 치료를 시도할 수 있다[17]. 약물치료에 반응이 없는 경우 수술적 방법에 의하여 확장된 장을 제거하거나 우회시키는 방법이 도움이 될 수 있다. 장 천공이나 장의 괴사가 의심되는 경우에는 바로 수술적 치료를 고려하는 것이 환자의 생명을 구하는 방법이 될 수 있다. 수술은 늘어난 장의 감압을 위하여 회장루(ileostomy)를 만들고 이후 증세가 호전되면 다시 연결을 하는 경우도 있으며, 대장만 침범한 경우 전 대장 절제술을 시행할 수도 있다[18]. 그러나 수술로 일시적인 호전이 되더라도 다시 악화될 경우 수술 후 유착에 의한 장폐쇄로 생각되어 재수술하는 경우가 많고, 또한 이 유착을 제거해도 장폐쇄의 증상이 계속 남을 수 있으므로 신중하게 선택해야 한다. 최근에는 장 이식이 시도되고 있으나 소장의 경우 다른 장기에 비하여 성공률이 매우 낮으며 아직 경험이 부족하므로 국내에서는 시행되지 않고 있다[19]. 본 환자의 경우 보존적 치료로 호전이 잘 되어 항생제나 neostigmine과 같은 약제를 투여하지는 않았고, 식이를 시작하면서 aclatonium napadisilate와 mosapride를 처방하였다.
성인에서의 만성 가성장폐쇄증의 임상경과에 대해 시행한 전향적 연구에 따르면 환자의 88%에서 수술, 1%에서는 이식을 시행하였고, 11%만이 약물치료로 호전되어 이 병의 예후가 비교적 좋지 않음을 알 수 있다. 특히 수술을 시행한 환자들에서 한 환자당 평균 2.96번의 수술을 받은 것으로 나타나 수술로도 치료가 잘 되지 않고 오히려 반복적 수술을 야기할 수 있음을 알 수 있었다[20]. 이번 환자의 경우에도 지금까지는 보존적 치료로 호전되어 왔으나 이번에는 앞서 보다 증상이 심했던 것으로 보아 앞으로 더 심해질 가능성이 있다. 그러나 이번 증례의 환자는 비교적 증상이 경한 상태에서 조기 진단하였으므로 향후 심한 장폐쇄가 있더라도 진단적 수술을 하는 등의 불필요한 수술을 피할 수 있다. 오히려 약물치료를 통하여 환자의 장 기능을 최대한 보존하여 환자의 삶의 질을 향상시킬 수 있을 것으로 기대된다.
만성 가성장폐쇄는 비교적 예후가 좋지 않고 심한 경우 사망에 이르는 심각한 질환이지만, 진단에 상당한 기간이 소요되면서 적절한 치료가 이루어지지 못하는 경우가 많다. 그러므로 이 질환의 조기진단은 불필요한 수술을 피하고 환자의 영양 유지, 장운동 회복 등에 초점을 맞추는 장기적인 치료 계획을 세우는 데 중요할 것으로 생각되어 본 증례를 보고하는 바이다.