Complicated Pleural Effusion의 진단과 치료
Diagnosis and Treatment of Complicated Pleural Effusion
Article information
Trans Abstract
Parapneumonic effusion is pleural effusion that arises in the pleural space, complicated with bacterial pneumonia. This occurs in at least forty percent of bacterial pneumonia. The usual parapneumonic effusion resolves well with antibiotic therapy. However, if bacteria invade the pleural space, a complicated parapneumonic effusion or empyema may result. In addition to appropriate antibiotic therapy, some parapneumonic effusions and empyemas need additional treatment, such as drainage procedures. The necessity of drainage for treatment of parapneumonic effusions depends on the several types or stages of parapneumonic effusion. Empyemas may need additional intervention beyond simple chest tube drainage, including placement of additional drainage tubes under fluoroscopy, video-assisted thoracoscopy with lysis of adhesions, and decortication. Patients with persistent air leaks often require surgical or endoscopic repair procedures. (Korean J Med 2011;81:143-149)
서 론
부폐렴성 늑막삼출액은 세균성폐렴이 발생한 폐에 근접한 늑막에 발생하는 늑막삼출액으로서 세균성폐렴의 40%에서도 발생한다고 알려져 있다[1]. 일반적인 부폐렴성 늑막삼출액은 소량이며 적절한 항생제 치료에 잘 반응한다. 그러나 세균이 늑막강까지 감염시키는 경우에는 complicated parapneumonic effusion 또는 농흉(empyema)이 발생한다. 이런 경우에는 항생제 치료 외에도 다른 부가적인 치료를 요하게 된다.
본 론
Complicated pleural effusion의 진단
임상양상
Parapneumonic effusion 또는 empyema의 임상양상은 환자가 어떤 단계에서 내원하였는지와 환자의 면역상태에 따라 달리 나타나며, 원인 균에 따라서도 달라질 수 있다. 폐렴의 초기단계에서 발견되는 경우에는 별다른 합병증 없이 진단되지만, 제대로 치료되지 못한 폐렴으로 인하여 흉막강내에 세균이 감염되면 농흉으로 처음부터 진단될 수 있다. 상당기간 동안 천천히 반복적으로 진행된 흡인성 폐렴으로 독성이 강하지 않은 혐기성세균에 의한 폐렴이 진행되는 경우에는 농흉으로 진행된 상태로 진단되는 경우가 많다. 그러나 심한 면역기능 장애 또는 면역억제 상태에서는 폐렴의 초기단계부터 농흉으로 빠르게 진행될 수도 있다.
흔한 임상양상은 기침, 발열, 흉막통, 호흡곤란, 객담 등이며, 초기증상이나 발열, 흉막통의 기간 등은 폐렴과 부폐렴 흉막삼출액 또는 농흉을 구별하는 데 결정적인 도움을 주지는 못하는 경우가 많지만, 단순폐렴보다는 합병증이 동반된 부폐렴 흉막삼출액이나 농흉에서 증상이 심하고, 증상지속시간이 긴 경우가 많다.
흉부진찰에서 폐렴에서 나타나는 수포음, 염소울음소리 (egophony), 흉막진동감(pleural fremitus) 증가 등의 소견이 아닌 감소된 호흡음 및 감소된 흉막진동감, 둔탁한 타진음 등이 진단에 도움이 될 수 있으나 상기 소견들이 불명확한 경우가 있으므로 방사선학적 검사가 중요하다.
영상의학 검사
흉부 X-선 촬영과 초음파 검사가 진단과 치료에 중요한 역할을 한다[2]. 단순 흉부PA 및 측면촬영소견에서 흉막삼출액의 양이 75 mL 이상일 경우에 posterior costophrenic sulcus가 소실되며, 175 mL 이상이 고인 경우에 lateral costophrenic sulcus가 소실된다. 500 mL 이상인 경우에 diaphragmatic contour가 소실되며, 4번 늑골까지 흉수가 차있는 경우에는 1,000 mL 정도에 해당한다. 측와위 촬영소견에서는 10 mL 이하의 흉막액도 진단이 가능하며, 측와위 촬영소견에서 소량의 늑막액은 1.5 cm 이하의 두께, 중등도는 1.5-4.5 cm 두께로 보이고, 대량의 흉막액은 4.5 cm 이상의 두께로 보인다[3]. 와위(supine) 흉부 X-선 사진에서는 175 mL 이상의 흉막액이 있어야 진단이 가능하며, 흉막액이 고여있는 폐측이 반대쪽 폐에 비해 뿌옇게 보이며, 환자의 상체를 거상하여 촬영하면 사라지는 경우에 의심할 수 있다[4]. 흉부 단순 촬영에서 complicated parapneumonic effusion 또는 empyema가 의심되는 소견은 늑막에 있는 음영으로서 전형적인 흉막삼출액과 다른 윤곽을 보이고 측와위 촬영소견에서 흐르지 않고 고정되어 있는 경우로서, 이런 소견이 보이면 초음파 검사 또는 CT 등의 추가 검사가 필요하다. 초음파 검사를 통하여 쉽게 소방성 흉막액을 확인할 수 있으며, 종괴와의 감별이 가능하다. 또한 흉막액의 양이 적거나 소방을 형성한 경우 흉수천자를 시행할 부위를 정하는데 도움이 된다. 일반적으로 empyema나 소방성 흉막액의 진단에는 흉부CT가 필요하며, 좀 더 많은 정보를 얻기 위해서는 조영제 투여 촬영이 좀 더 도움이 된다. 벽측 흉막의 비후 시에는 농흉이 의심되며, 작은 공기주머니음영들이 흉막삼출액 부위에 포함되어 있어 소방성 흉막액이 의심되는 경우에는 흉관배액(chest tube drainage) 또는 경피도관배액(percutaneous catheter drainage) 등의 치료에도 잘 반응하지 않을 것으로 예상할 수 있다. 추가적으로 폐 실질의 병변이나 기도의 병변들도 진단될 수 있는 장점이 있다[5-7].
흉수천자(thoracentesis)
흉수천자는 기본적인 진단검사로서 흉수의 성상을 확인하고 배양검사 및 항생제 감수성 검사를 시행하기 위하여 반드시 필요하다. 부폐렴 흉막삼출액에서 흉수천자가 필요한 일반적인 경우는 다음과 같다[8]. 첫째, 측와위 촬영소견상 10 mm 이상의 흉수가 보일 때 둘째, 흉수가 loculation 되어 있을 때 셋째, contrast enhanced CT 에서 벽측 흉막의 비후가 관찰되어 농흉이 의심될 때 넷째, 초음파 소견에서 흉막액이 확인된 경우 등이 있다. 초음파로 흉막천자 부위를 정하는 것이 일반적으로 도움이 되며, loculation이 되어 있는 경우에는 초음파나 CT를 이용하는 것이 보다 안전하고 효과적으로 흉수천자를 시행할 수 있다.
흉막액 분석
흉수천자로 얻은 흉막액을 이용한 여러 검사가 complicated pleural effusion 및 농흉의 진단에 도움이 된다. 미생물 검사, 세포진검사, 생화학적 검사 및 pH검사 등이 반드시 의뢰되어야 하며, 흉막액의 pH는 blood gas analyzer를 이용하여 검사하여야 하지만 불가능한 경우에는 흉막액의 glucose 농도 측정으로 대치하여 사용할 수도 있다[9]. 일반적으로 흉막액의 pH < 7.20 또는 glucose < 60 mg/dL일 경우에는 자연적인 소실을 기대하기 어려우므로 배액이 필요하지만 이 기준은 임상적으로 확실히 증명된 것은 아니므로 너무 이 기준을 엄격하게 적용하는 것은 권장되지는 않는다[9]. American College of Chest Physicians (ACCP) consensus guideline에서는 pH < 7.20인 경우에 배액술을 권장하고 있다[8]. 그러나 이런 경우에는 pleural fluid acidosis나 low glucose 수치를 나타낼 수 있는 악성종양, 결핵, 류마티스성 늑막염 또는 lupus 늑막염 등을 감별하여야 한다[10]. 감염성 질환의 biomarker들인 C-reactive protein (CRP), procalcitonin, STREM-1 등이 농흉의 진단에 도움이 되는지를 확인하는 연구들이 있었지만 기존의 생화학검사들에 비해 우월한 유용성이 증명되지는 않았다[11,12].
미생물학적 검사
수많은 세균이 parapneumonic effusion이나 empyema의 원인이지만 특히 혐기성 균의 증명은 어려운 경우가 많다. 부패성 냄새(putrid odor)가 있으면 혐기성 세균에 의한 농흉의 가능성이 많으며, 그람 염색이 도움이 된다. 혐기성세균은 농흉의 36-76%에서만 증명되며, Fusobacterium nucleatum, Prevotella sp, Peptostreptococcus, Bacteroides fragilis group이 주된 원인 균으로 알려져 있다[13,14]. 그러므로 농흉의 경우에 혐기성 세균이 확인되지 않았다고 하더라도 혐기성세균에도 효과적인 항생제를 사용하는 것이 도움이 된다[15].
그 외에도 농흉에서 흔히 발견되는 세균은 Streptococcus milleri, Staphylococcus aureus, Enterobacteriaceae 등이며, 당뇨환자에서는 Klebsiella pneumonia 감염에 의해서도 농흉이 흔히 발생한다[16].
인플루엔자 감염 합병증으로 발생하는 농흉에서는 S. aureus, S. pneumoniae, S. pyogenes 등이 주된 원인균이다[17]. 항생제 치료에 반응하지 않아서 video-assisted thoracoscopic drainage를 시행한 234명의 complicated parapneumonic effusion 환자들에서 발견된 원인균은 Streptococcus pneumoniae (20%), Staphylococcus aureus (21%), coagulase negative staphylococcus (17%), Pseudomonas (14%), Klebsiella (10%)였다[18].
Complicated pleural effusion의 치료
흉강천자 등을 통해 합병부폐렴삼출이나 농흉으로 진단되면, 적절한 항생제 치료가 중요하며, 잘 치료되지 않는 경우에는 흉관배액(chest tube drainage) 또는 경피도관배액(percutaneous catheter drainage)이 필요하게 되고, 섬유소용해물질(fibrinolytic agent)이 선택적으로 사용된다. 이러한 치료에도 불구하고 적절한 배액이 이루어지지 않을 경우 흉강경수술(video-assisted thoracoscopic surgery, VATS), 겉질제거(decortication) 등의 외과적 수술이 시행되기도 한다. 최근에는 항생제의 개선과 섬유소용해물질 사용의 보편화 등으로 치료성적의 향상이 있었으나 농흉의 경우는 아직도 20% 이상의 높은 사망률을 보인다[19].
항생제 선택
가장 중요한 원칙의 원인질환인 폐렴의 가장 가능성이 높은 원인 균에 대한 적절한 항생제를 경험적으로 또는 미생물 검사 결과를 바탕으로 치료하는 것이다. 대부분의 항생제는 늑막강내로 잘 침투하지만, pH가 낮은 흉막삼출액 내에서는 aminoglycoside 계통의 항생제는 효과가 없을 수 있음을 염두에 두어야 한다[20]. 혐기성 세균이 complicated pleural effusion 또는 농흉의 원인균인 경우가 많으며 증명되지 않는 경우가 많으므로 혐기성세균도 치료할 수 있는 경험적 항생제 치료가 권장되며, 일반적으로 clindamycin, beta-lactam plus beta-lactamase inhibitors (amoxicillin-clavulanate, ampicillin-sulbactam, piperacillin-tazobactam), carbapenems (imipenem, meropenem, or ertapenem) 등이 사용되지만, penicillin 또는 metronidazole 등의 단독요법은 권장되지 않는다. Complicated parapneumonic effusion (category 3 in the ACCP consensus guidelines) (Table 1)은 항생제 치료에 반응하지 않는 경우가 많다[8]. 그러므로 조기에 모든 소방성 흉막삼출액을 흉관배액 하는 것이 치료효과를 높이고 입원기간을 줄이는 방법으로 여겨지고 있지만[21], 아직까지 전향적 연구로 확인되지는 않았다. 또한 다수의 loculated pleural effusion에서는 필요한 경우 여러 개의 흉관 튜브를 삽입하여 신속하게 배액하는 것이 필요할 수 있다. 흉관배액술로 호전되지 않는 경우에는 항생제 치료가 부적절하였거나 흉관배액술 치료 중에 합병되는 소방성 농흉을 의심하여야 한다. 추적 CT 검사나 영상검사에서 흉막삼출액의 배액이 불충분한 경우에는 video-assisted thoracoscopic surgery (VATS)를 통하여 죽은조직제거술(debridement)과 배액을 추가로 시행하는 것이 필요하다.
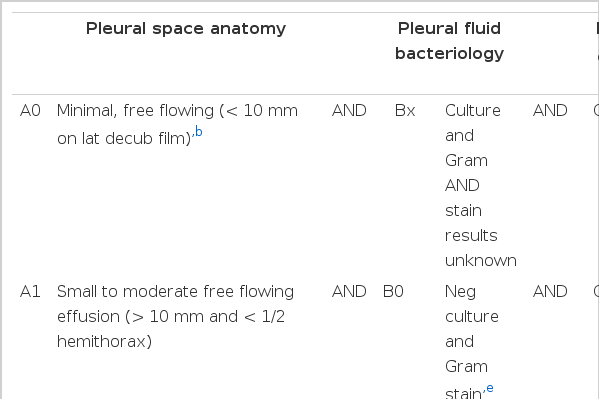
Categorizing risk for poor outcome in patients with parapneumonic effusions
농흉의 치료
농흉(category 4 in the ACCP consensus guidelines)은[8], 필요하다면 조기에 적절한 또는 개흉 죽은 조직제거술(open thoracotomy ebridement)과 배액을 고려하여야 한다[22]. 적절한 농흉의 치료과정은 우선 최소한 4-6주 이상의 적합한 항생제 치료를 시행하여 농흉내의 세균감염을 치료하고, 흉관 배액량이 최소한으로 될 때까지 기다리고 CT로 더 이상의 농흉이 남아 있지 않음을 확인하며, 농흉강이 없어져서 폐가 완전히 펴질 때까지 치료하는 것이다.
농흉의 배액
농흉의 배액방법은 tube thoracostomy, video-assisted thoracoscopic surgery (VATS), open decortication과 open thoracostomy가 사용될 수 있다.
흉관배액(tube thoracostomy drainage)은 농흉액의 배액에서 가장 덜 침습적인 방법이다. 이 방법은 단일소방 농흉에서 주로 효과적인 치료방법이지만 다방성 농흉에서도 흔히 시도되는 치료방법이다. 흉관의 삽입위치는 CT나 초음파검사를 이용하여 결정하는 것이 안전하고 효과적이다. 다방성 농흉에서는 주로 소구경의 여러 개의 흉관을 삽입하여 각각의 소방성 농흉을 배액하는 것이 좋다. 일반적으로 단일소방 농흉에서는 구경이 큰 흉관을 삽입하는 것이 효과적인 것으로 여겨져 왔지만, Multi-center Intrapleural Streptokinase Trial (MIST1)에서 대구경(15-20F), 중간구경(10-14F), 또는 소구경 흉관(< 10F) 사용여부에 따른 치료 성공률이나 사망률의 차이가 없었으나, 흉관배액술 시에 소구경 흉관을 사용하는 경우 통증 및 합병증의 빈도는 유의하게 낮았다[23,24].
소구경흉관을 사용하는 경우 튜브가 막힐 가능성이 높다는 점이 우려되었으나 주기적으로 흉관내강을 생리식염수로 세정(30 mL of sterile saline every 6 hours via a three way valve)해주는 방법이 British Thoracic Society guideline에서는 권장되고 있다[25]. 농흉의 배농을 위한 흉관 삽입 후 24시간 이내에 CT를 촬영하여 흉관의 위치가 적절한지 여부를 확인하는 것이 도움이 되며, 배농되는 양이 50 mL/day 이하로 감소하고 농흉강이 폐쇄될 때까지 유지한다.
섬유소용해제 요법
흉강 내 섬유소용해제 요법(streptokinase, urokinase, tissue plasminogen activator [TPA])은 loculated parapneumonic effusion과 농흉의 배액을 위해 사용되어 왔으나 여러 연구들에서 효과에 대한 주장이 상반되고 있다. 그러나 현재까지 섬유소 용해 치료는 흉관배액이 잘 안되고 흉수가 많이 차 있는 증상이 있는 환자에서는 효과가 있을 수 있으며, 새로운 약제인 deoxyribonuclease를 사용하면 농흉의 점성이 감소하여 배액이 잘 되기 때문에 섬유소용해제와 병합투여할 수 있다. 특히 외과적인 배액을 하기 어렵고 지속적인 패혈증이 있는 환자에서도 사용해 볼 수 있다[26]. 기존의 연구들의 연구방법과 약제의 투여방법에 문제가 있어서 아직은 섬유소 용해요법의 효과에 대한 결론을 내리기 힘들며, 현재 TPA를 사용하는 대규모 임상연구가 진행 중이다.
흉강경하 죽은조직제거술(thoracoscopic debridement)
Video-assisted thoracoscopic surgery (VATS)를 이용하여 complicated pleural effusion 특히 uni-or multi-loculated empyema를 치료할 수 있다[27]. 농흉의 VATS 치료 시도 중에 치료가 어려울 경우에는 개흉술로 바로 전환하여 적절한 조치를 취할수 있다는 것이 장점이다. VATS 시도하였으나 결국은 개흉술이 필요한 경우는 44%에서 3% 정도까지 다양하다[28,29]. 개흉 decortication이 필요하게 되는 위험인자는 치료가 지연되었을 경우와 그람음성균에 감염된 농흉인 경우이다.
겉질제거(decortications)
흉막의 비후는 흉막염이 치료되고 나면 점진적으로 호전되지만, 장측흉막의 비후가 호전되지 않으면서 폐가 다시 펴지지 않으면 농흉강이 형성된 경우가 많다. 이런 경우에는 겉질제거가 필요하게 된다[30]. 흉강경하 겉질제거의 치료성적은 개흉 겉질제거의 성적과 비슷하다[31]. 흉막유착이 심하고, 장측흉막의 비후가 심하고, 농흉의 크기가 큰 경우에는 개흉 겉질제거를 선호하는 경향이 많다[32].
Open thoracostomy
Open thoracostomy는 농흉강의 하부에서 배액이 되도록 늑골의 일부를 절제하고 흉강에 계속적인 배농이 되도록 입구를 만들어 놓는 수술로서 우선은 흉관을 삽입한 채로 유지하다가 60-90일 정도 지나면 입구가 안정되게 남아 있게 된다. Open thoracotomy는 겉질제거보다는 덜 침습적인 수술로서 환자의 상태가 좋지 않을 때 선택할 수 있는 치료법이다.
일차치료에 반응하지 않는 증상이 있는 비악성 흉막삼출액의 치료
흉막삼출액은 원인에 대한 치료가 가장 중요하며, 대개 호전되지만 악성흉수가 아님에도 불구하고 일부에서는 치료에 반응하지 않고 계속 흉막삼출액이 지속되는 경우가 있다. 이런 경우 증상이 있는 경우라면 일반적으로 반복적인 흉막천자 또는 흉막유합(pleurodesis)이 필요할 수 있다. 그 외에 다른 치료방법으로 간헐적인 흉막배액을 위한 indwelling pleural catheter를 삽입하거나, pleurectomy 또는 pleural-peritoneal shunt 등의 특수한 치료가 필요할 수도 있다.
치료대상
일차치료에 반응하지 않는 흉막삼출액으로서 호흡곤란 등의 증상이 있는 경우에 치료대상이 될 수 있다. 일차치료 외에 좀더 침습적인 치료를 고려하기 전에 우선 흉막삼출액의 원인을 다시 확인하고, 폐의 허탈로 인해 흉막삼출액이 소실되지 않는 지를 먼저 확인하여야 한다. 증상이 없는 경우에는 아래와 같은 침습적인 치료들을 시도할 필요가 없다.
치료방법
반복적인 흉수천자
반복적인 흉수천자는 흉수의 증가속도가 느려서, 한번 흉수천자를 시행하고 상당기간이 지나서야 다시 흉수천자가 필요한 경우에 적절하다. 자주 흉수천자가 필요하여 반복적 시술의 위험성이 증가하거나 환자의 불편함이 증가한다면 다른 치료방법을 시도하는 것이 좋다. 대개 한 달에 1번 정도의 흉수천자로 잘 조절이 되는 경우라면 시도해 볼 수 있는 치료방법이다. 대개 한번 시술 시 1-1.5 L의 흉수를 천천히 배액하는 것이 적절하다. 흉수배액이 너무 빨리 되면, reexpansion pulmonary edema가 합병증으로 발생할 수 있는데, 이런 합병증은 매우 드물며, 배액 중에 환자가 흉통을 호소하거나 흉막압이 -20 cmH2O로 떨어지면 배액을 중단하는 것만으로도 방지할 수 있다[33]. 합병증을 방지하기 위해 권장되는 배액속도는 아직까지 알려진 바 없으며, 시술 중에 환자를 관찰하는 것이 가장 좋은 방법이다[33]. 그 외에 발생할 수 있는 합병증은 배액 중에 발생하는 기흉으로서 배액 중에 폐가 다시 펴지지 않는 경우에 발생할 수 있다[34].
흉막유합(Pleurodesis)
흉막유합은 흉막액을 배액 한 후에 흉막강을 폐쇄시켜 더 이상의 반복적인 흉막액 저류를 방지하기 위한 시술로서 talc가 가장 많이 사용되는 약제이다. 다른 약제로는 tetracycline, minocycline, doxycycline, silver nitrate, iodopovidone, bleomycin, Corynebacterium parvum with parenteral methylprednisolone acetate, erythromycin, fluorouracil, interferon beta, mitomycin C, cisplatin, cytarabine, doxorubicin, etoposide 등이 시도되고 있다. 그러나 약제의 생산중단 및 talc의 경우 발암물질로서의 위험성 등으로 인해 제한 점이 있는 점 등을 고려하여 적절한 약제를 선택하여 시술한다[35-40].
흉막유합은 증상이 있으며 반복적인 흉수천자에도 불구하고 수일내지 일주일 이내에 다시 흉수저류가 발생하는 환자에서 권장되며, 대개 치료성적은 50-70% 정도의 성공률을 보이는 것으로 알려져 있다[41-44].
흉막유합은 폐가 다시 펴지지 않는 경우에는 시술할 수 없으며, 흉막내 감염증으로 인한 반복적인 흉막삼출액에서도 사용할 수 없다.
흉막유합의 드문 합병증은 호흡부전, 심혈관계 합병증, 전신염증반응, 농흉, 폐 용적의 감소와 흉막유합에 사용된 약제에 의한 전신반응 등이 있으며, 대부분의 합병증은 악성흉막삼출증에서 보고되었지만 비악성흉막삼출증에서도 일어날 수 있으므로 주의를 요한다. 그 외에도 talc를 사용한 경우에 급성호흡부전 및 오랜 시간이 경과 후 발생할 있는 늑막석회화 및 악성종양의 가능성에 대한 우려도 보고되고 있다[45,46].