항혈소판제제를 포함한 약물상호작용에 미치는 프로톤펌프억제제의 영향: Safe 측면
Drug Interaction between Proton Pump Inhibitors and Clopidogrel: Safe Perspective
Article information
Trans Abstract
Clopidogrel prevent atherothrombotic complications following acute coronary syndromes by inhibiting platelet aggregation. However, in case of concomitant use of clopidogrel and proton pump inhibitor (PPI) for prophylaxis of gastrointestinal (GI) bleeding, the anti-clotting of clopidogrel will be decreased because PPI inhibit competitively cytochrome P450 enzymes, especially CYP2C19. Through several pharmacodynomic studies, omeprazole, but not other PPIs, worsens surrogate markers (e.g., platelet reactivity index) of clopidogrel efficacy. And many observational studies show concomitant use of clopidogrel and PPI have increased the risks of cardiovascular (CV) events (hazard/odds ratios = 1.25-1.5). However, only one prospective randomized trial (COGENT trial) of omeprazole vs. placebo in clopidogrel users show no difference in CV events (hazard ratio = 1.02) and decrease the risk of GI bleeding (hazard ratio = 0.13). Further well designed research will need to determine whether a pharmacodynamic effect of clopidogrel affected by PPI will be changed clinical CV events. Clinical decisions about concomitant use of PPI and clopidogrel must be balance overall risks and benefits, considering both CV and GI complications.(Korean J Med 2011;81:26-33)
서 론
프로톤펌프억제제(proton pump inhibitor)는 소화성궤양과 궤양출혈, 역류성식도염, 기능성소화불량증, 비스테로이드성 항염증제에 의한 위장관 손상 등에서 광범위하게 처방되는 위산분비 억제제로 효과가 강력하고 비교적 안전한 약제로 평가되었다. 그러나 이 약제를 사용한 임상경험이 20여 년이 넘어가면서 부작용에 대한 연구가 점점 많이 보고되고, 몇몇 약제와의 상호작용이 논란의 중심에 있다. 최근 가장 이슈가 되는 것이 클로피도그렐(clopidogrel)과 프로톤펌프억제제의 상호작용이다. 이에 대해서는 미국 식약청(U.S. Food and Drung Administration)에서 2009년 11월 처음 경고 메시지를 띄웠는데, 클로피도그렐과 오메프라졸(omeprazole)을 함께 투여했을 때, 클로피도그렐의 효과가 감소한다는 연구를 반영한 것이었다[1]. 그 이후 여러 약물역동학적 접근에 따른 연구들과 실제 임상에서 심혈관계 환자에서의 클로피도그렐과 프로톤펌프억제제의 상호작용에 대한 여러 연구가 발표되고 있다. 어떤 약제든 부작용이나 상호작용이 없을 수는 없다. 그러나 이러한 관계를 잘 이해하고, 그 약제의 효과와 위험성을 잘 견주어 평가하는 것이 중요할 것이다.
본 장에서는 프로톤펌프억제제와 클로피도그렐의 상호작용이 가능한 원리와 그와 관련된 약물역동학적 연구, 클로피도그렐 사용자에서 진행된 프로톤펌프억제제의 영향에 대한 임상 연구 등을 소개하고, 임상에서의 적용 방법에 대해서 고찰하겠다.
프로톤펌프억제제와 클로피도그렐의 상호작용은 왜 일어나는가?
프로톤펌프억제제는 prodrug로서 간의 cytochrome P450 (CYP)에 의해 대사되어 비활성화되는데, 이 중 CYP2C19가 주된 효소이다. 또한 이 약제 자체가 CYP2C19 효소의 대사를 경쟁적으로 억제하는데, 기존의 오메프라졸(omeprazole)과 란소프라졸(lansoprazole)이 가장 억제 능력이 크고, 에소메프라졸(esomeprazole)이나 판토프라졸(pantoprazole)이 억제 능력이 다소 적다. 따라서 프로톤펌프억제제의 종류에 따라 CYP2C19에 대한 억제 능력의 차이가 있는데[2], 오메프라졸이 클로피도그렐과 상호작용이 가장 많은 이유가 여기에 있다.
클로피도그렐은 혈소판의 응집을 억제하는 약제로 심혈관계 환자에서 혈전 방지 효과가 우수하다. 이 약제는 비활성화된 prodrug 형태로 투여되어 체내에서 CYP 효소에 의해 활성화되어 혈소판의 P2Y12 receptor를 비가역적으로 억제하여 혈소판의 응집을 방해한다[3]. CYP 효소 중 특히, CYP2C19가 클로피도그렐의 활성화에 가장 중요한 역할을 하는 효소인데, 이 CYP2C19 유전자에 유전적 결함에 의해 그 기능이 떨어지면 클로피도그렐의 혈소판 응집 억제 능력이 저하되어 이런 환자에서는 클로피도그렐을 복용하더라도 심혈관계 위험성이 증가한다는 것을 알게 되었다[4,5]. CYP2C19 유전자의 다형성에 따른 대사저하군(poor metabolizer)에서는 클로피도그렐의 효과가 떨어지는데, 여기에 프로톤펌프억제제의 CYP2C19 효소에 대한 경쟁적 억제가 가중되면, 클로피도그렐의 효과가 더욱 떨어진다고 하겠다. 특히, CYP2C19 효소의 대사저하군은 서양인보다 아시아인에서 더욱 비율이 높은데(1-4% 서양인 vs. 12-23% 아시아인) [6], 따라서 향후 아시아에서 진행되는 연구의 필요성이 중요할 것이다.
이상의 배경으로 프로톤펌프억제제, 특히 오메프라졸은 클로피도그렐의 활성화를 유도하는 CYP2C19을 경쟁적으로 억제하여 그 효과를 감소시킬수 있다. 이러한 CYP2C19 효소의 억제 역할을 할 수 있는 약제는 cimetidine, fluconazole (Diflucan), ketokonazole (Nizoral), voriconazole (VFEND), etravirine (Intelence), felbamate (Felbatol), fluoxetine (Prozac, Serafem, Symbyax), fluvoxamine (Luvox), ticlopine (Ticlid) 등이 있다. 여러 프로톤펌프억제제의 종류에 따라 CYP2C19 효소의 억제 능력이 차이가 있다고 추정하지만, 아직 그 근거가 명확하지 않고, 다른 H2 수용체 억제제인 ranitidine (Zantac), famotidine (Pepcid), nizatidine (Axid) 등은 아직 클로피도그렐과의 상호작용에 대한 근거가 없다. 따라서 클로피도그렐과 오메프라졸 및 앞에 언급된 약제들을 동시에 투여하지 않도록 권유하고 있다[1].
프로톤펌프억제제가 클로피도그렐의 약물역동학적 효과에 영향을 미치는가?
프로톤펌프억제제가 클로피도그렐의 효과를 떨어뜨린다는 첫 약물역동학적 연구는 Gilard 등[7]이 발표하였다. 이 연구자들은 먼저 코호트 연구를 통하여 오메프라졸을 복용하는 환자들에서 PRI (platelet reactivity index)가 50% 이상으로 클로피도그렐의 효과가 떨어지는 것을 확인하였다. 여기서 PRI가 높을수록 혈전이 잘 생기는 것을 의미한다. 이를 배경으로 이중맹검으로 124명의 심혈관 스텐트를 삽입한 환자를 대상으로 아스피린과 클로피도그렐을 복용시키면서, 무작위로 오메프라졸(20 mg/day)과 위약을 투여하였다. 투약 첫날에는 양군의 PRI는 차이가 없었지만, 7일째에는 각각 51.4%, 39.8% (p< 0.0001)로 오메프라졸 군에서 PRI가 높았다[8]. 이 연구가 OCLA (Omeprazole CLopidogrel Aspirin) trial로 처음으로 프로톤펌프억제제가 클로피도그렐의 효과를 감소시킨다는 것을 증명한 것으로 이 두 약제의 상호작용이 논란이 시작된 계기가 되었다.
그 이후 이와 유사한 약물역동학적 효과의 변화를 연구한 논문들이 발표되었는데(Table 1), 모두 두 약제를 사용한 뒤 초기 1-2주(week)의 변화를 관찰한 것으로 장기간 사용했을 때의 결과를 알 수 없다는 제한점이 있다고 생각한다. 또한 Gilard 등의 연구[7,8]와는 달리 약물역동학적 효과의 저하가 없어 판토프라졸이나 란소프라졸, 에소메프라졸 등의 억제 영향이 크지 않았지만[9-11], 오메프라졸에서는 위약군보다 응집력이 증가하였다[11]. 그리고, CYP2C19의 유전자 이상으로 기능이 떨어진(reduced-function CYP2C19 allele) 환자군에서는 프로톤펌프억제제를 사용한 경우에 혈소판 응집력이 유의하게 떨어졌으나, 임상적으로 심혈관 질환의 위험률이 증가하지는 않았다[12].

Studies assessing effect of PPI on pharmacodynamic outcomes in clopidogrel users
따라서 약물역동학적 연구에 의하면, 클로피도그렐과 프로톤펌프억제제를 동시에 사용하면, 항혈소판 작용이 감소하고 이는 오메프라졸에서 가장 뚜렷하였다. 그러나 이러한 PRI 등의 역물역동학적 표지자가 임상적인 의미가 있는지는 아직 정립되지 않았다.
클로피도그렐은 위장관 출혈을 증가시키는가?
클로피도그렐의 사용이 위장관 출혈을 증가시키는지는 아직 명확하지 않고 근거가 부족하다. 그러나 환자-대조 연구에 의하면, 클로피도그렐이나 ticlopine을 사용하는 경우에 약 2.8배의 상대적 위험성이 있고, 아스피린을 같이 복용하면 3.7배로 증가하였다[13]. 또 다른 무작위 연구에서는 클로프도그렐과 아스피린을 같이 사용하는 경우에 아스피린 단독사용군에서보다 위장관 출혈의 상대적 위험도가 80-95%까지 증가하였다[14,15].
프로톤펌프억제제가 클로피도그렐에 의한 위장관 출혈을 감소시킬 수 있는가?
클로피도그렐이 위장관 출혈의 위험성이 있는 약제이므로 프로톤펌프억제제가 출혈을 감소시킬수 있는지에 대한 연구가 진행되었다. 환자-대조군 연구로서, 클로피도그렐 혹은 ticlopidine을 투여 중에 위장관 출혈 환자를 대상으로 최근 프로톤펌프억제제를 투여받았던 군과 그렇지 않은 군을 비교하였을 때, 프로톤펌프억제제 투약군에서 출혈의 위험도가 0.19로 크게 감소하였다[16]. 또한 이러한 출혈 예방은 H2수용체 억제제보다 프로톤펌프억제제가 더 강력하다[17,18].
최근 2010년 발표된 프로톤펌프억제제와 클로피도그렐을 비롯한 thienopyridine 사용에 대한 합의도출에서는 클로피도그렐과 아스피린 동시 사용군에서 아스피린 단독사용군보다 중요 심혈관계 부작용이 감소하지만, 출혈 위험성 때문에 이전에 허혈성 뇌경색이 있었던 환자에게는 두 약제를 동시에 사용하는 것을 권유하지 않는다. 그리고 이전의 궤양력이 있거나, 항혈소판제제가 필요한 환자에서 위장 출혈의 위험성이 높은 경우(고령, 항응고제, 스테로이드 혹은 비스테로이드성 항염증제, 아스피린을 같이 사용하거나 Helicobacter pylori 감염군)에는 프로톤펌프억제제를 사용할 것을 권유하였다[18].
프로톤펌프억제제가 클로피도그렐의 효과를 감소시켜 실제 임상상에 반영되는가?
프로톤펌프억제제를 클로피도그렐과 함께 사용할 때, 약물역동학적 효과의 감소가 실제 임상에서 심혈관 환자의 혈전 예방의 효과 감소로 다시 급성심근경색이나 뇌경색 등 심혈관계 질환의 발생과 위장관 출혈 등을 관찰하는 임상 연구가 계속 보고되고 있다(Table 2). 표에는 연구 디자인이나, 연구의 일차 목표, 결과 및 평가를 요약하였다. 일견 두 약제를 동시에 사용하는 것이 심혈관계 부작용이 유의하지 않다는 연구와[5,12,19,24,25,28] 심혈관계 부작용이 증가한다는 연구가 서로 상충하고 있다[20-23,26,27,29].
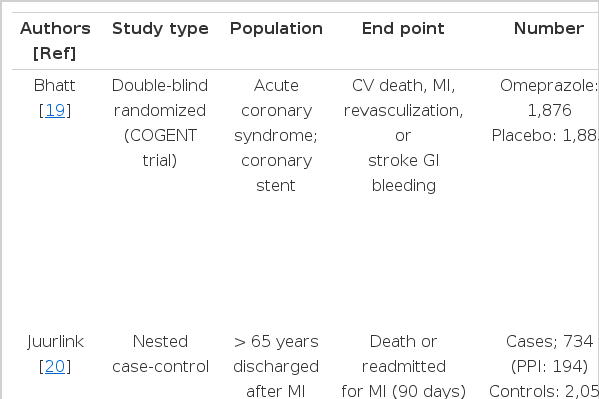
Studies assessing effect on PPI on clinical outcomes in clopidogrel users
최근에 보고된 클로피도그렐과 프로톤펌프억제제 사용에 대한 체계적 문헌고찰에서도 지적하듯이 대부분의 연구 디자인에 문제가 있어 기울기(bias)의 위험성이 많아 향후 잘 고안된 연구가 필요하다고 지적하였다[30]. 이 중 유일하게 이중맹검에 의해 전향적으로 진행된 연구가 COGENT trial이다[19]. 그러나 연구 도중, 기획 회사의 파산으로 5,000명 중 3,873명을 모으는데 그치면서 조기 종료되었다. 오메프라졸과 위약군에서 심혈관계 합병증의 빈도의 차이는 없었고(omeprazole HR=0.99), 오히려 오메프라졸 사용 군에서 위장관 출혈의 발생이 감소(HR 0.13, 95% CI 0.03-0.56)하여 프로톤펌프억제제의 출혈 예방의 장점이 부각되었다. 그러나 조기 중단된 연구라는 점, 연구자의 94%가 백인으로 CYP2C19 유전자의 reduced-function CYP2C19 allele를 보이는 경우가 2-3% 정도로 매우 낮다는 제한점이 있고, 오메프라졸 단독만 사용한 점이 아쉽다.
국내에서도 협심증과 심근경색증으로 내원한 환자 중 clopidogrel 투약을 시작한 환자를 대상으로프로톤펌프억제제를 함께 투여한 실험군과 clopidogrel만 단독으로 투여한 대조군으로 하여 의무기록 분석을 통한 후향적 연구가 최근 보고되었다[29]. 흉통으로 인한 재입원이나 사망률은 실험군에서 42.4%, 대조군에서 24.2%로 유의하게 차이가 있었으며, 다변량 분석에서 프로톤펌프억제제의 병용투여는 clopidogrel을 사용하는 허혈성 심장환자에서 프로톤펌프억제제를 투여하지 않는 환자에 비해 재입원이나 사망의 위험을 높이는 것으로 나타났다(adjusted HR 2.51, 95% CI 1.43-4.40, p= 0.001). 약제별 하위집단 분석에서는 lansoprazole의 병용투여가 그렇지 않은 환자에 비해 2.66배의 위험도를 나타내었다(adjusted HR 2.66, 95% CI 1.45-4.89, p= 0.002). 약제 사용 기간이나 용량은 재입원이나 사망의 위험도에 영향을 주지 않았고, H. pylori의 감염 유무에 따른 primary outcome의 차이는 없었다. 따라서 이 연구에서는 프로톤펌프억제제를 함께 투여하는 경우에는 심혈관계 합병증이 증가하므로 동시 투여에 주의해야 한다고 하였다.
COGENT trial과 무작위 혹은 관찰 연구 25개를 대상으로 한 메타분석에서는 프로톤펌프억제제와 클로피도그렐의 병용이 심혈관 질환을 1.26배 증가시키지만 사망률에는 영향이 없다고 하였다[31].
이상 요약하면, 대부분 여러 제한점이 많은 관찰연구와 1개의 무작위 전향 연구의 결과로 본다면, 두 약제의 동시 사용이 심혈관계 합병증을 증가시키는지는 아직 일관된 결과를 보이지 않고, 상대적 위험도도 높지 않다. 그러나 동시 투여군에서는 위장관 출혈은 의미 있게 감소한다고 생각된다. 그리고 상대적으로 아시아 인구에 많은 CYP 유전자의 대사 저하군(poor metabolizer)에서의 임상적 영향이 어떨지 앞으로의 연구가 필요한 부분이다.
클로피도그렐과 프로톤펌프억제제를 동시 사용할 때의 권고사항
오메프라졸 이외의 프로톤펌프억제제를 사용
미국 FDA는 COGENT trial이 나왔지만, 여전히 클로피도그렐과 프로톤펌프억제제에 대한 경계를 늦추지 않았는데, Plavix (clopidogrel)와 오메프라졸은 함께 사용하지 않도록 권고하였다. 그러나 이러한 조치는 다른 프로톤펌프억제제에 모두 해당되는 것은 아니며, 오메프라졸의 대안적 투여는 판토프라졸을 권고하였는데, 그 이유는 판토프라졸이 CYP2C19 억제 능력이 가장 적기 때문이다[32].
투여 시간의 조절
프로톤펌프억제제나 클로피도그렐 모두 혈청에서 짧은 시간 존재하므로 투약시간을 조절하여 이론적으로 프로톤펌프억제제는 아침 식전, 클로피도그렐은 취침 시에 혹은 각각 저녁식전, 점심때 투여할 것을 권유하였지만[33], 연구 결과가 입증된 권고사항은 아니다. 그러나 클로피도그렐과 오메프라졸을 투약시간을 조절하여 투여하더라도 이 두 약제의 상호관계는 감소하지 않았다.
Prasugrel 사용
Prasugrel은 새로운 강력한 혈소판 P2Y12 수용체를 억제하는 약제로 아직 프로톤펌프억제제와의 상호 작용은 잘 알려져 있지 않지만, 약물역동학적 연구에서 프로톤펌프억제제에 의해 PRI의 증가가 관찰되지 않았고[9], CYP2C19 reduced- function gene variant를 가진 환자에서 ADP-유발 형소판 응집이 감소하지 않았다[34]. 그러나 prasugrel은 클로피도그렐보다 출혈의 합병증이 높아 급성 관상동맥 증후군의 중등도 혹은 중증에서 선별하여 사용할 것을 권고하고 있다.
H2수용체 억제제의 대체 사용
출혈 예방 효과가 프로톤펌프억제제보다 못하지만, H2수용체 억제제가 프로톤펌프억제제의 대안이 될 수 있지만, cimetidine을 제외한 ranitidine (Zantac), famotidine (Pepcid), nizatidine (Axid)은 클로피도그렐과의 상호작용이 아직까지 보고되지 않았다.
클로피도그렐과 아스피린을 같이 투여하는 경우에는 이전의 궤양력이나 위장관 출혈이 있거나 비스테로이드성 항염증제, 항응고제 등을 사용하는 경우에는 위장관 점막 보호 치료제를 사용해야 한다[33].
결 론
클로피도그렐은 혈소판의 응집을 억제하는 약제로, 활성화되는데는 CYP 효소 중 특히, CYP2C19가 중요하다. 문제는 프로톤펌프억제제가 CYP2C19을 경쟁적 억제하여 클로피도그렐의 혈소판 응집효과를 저하시킬 수 있다. 약물역동학적 연구에 의하면, 클로피도그렐과 프로톤펌프억제제를 동시에 사용하면, 항혈소판 작용이 감소하고 이는 오메프라졸에서 가장 뚜렷하였다. 그러나 이러한 PRI 등의 역물역동학적 표지자가 임상적인 의미가 있는지는 아직 정립되지 않았다.
두 약제의 사용이 실제 심혈관계 합병증을 증가시킬 것인가에 대한 임상 연구들의 결과에 의하면, 두 약제의 동시 사용이 심혈관계 합병증을 증가시키는지는 아직 일관된 결과를 보이지 않지만 상대적 위험도도 높지 않다. 그러나 동시 투여군에서는 위장관 출혈은 의미 있게 감소한다고 생각된다. 그리고 상대적으로 아시아 인구에 많은 CYP 유전자의 대사 저하군(poor metabolizer)에서의 임상적 영향이 어떨지 앞으로의 연구가 필요한 부분이다.
클로피도그렐을 사용하는 환자에서 프로톤펌프억제제를 동시에 사용하는 경우에 대한 권고사항은 오메프라졸은 더 이상 사용하지 않고, 다른 프로톤펌프억제제를 고려하거나, H2수용체 억제제를 사용한다. 혹은 두 약제의 투여 시간을 분리하는 것도 하나의 방법이다. 그리고 클로피도그렐과 아스피린 동시 사용군에서 아스피린 단독사용군보다 중요 심혈관계 부작용이 감소하지만, 출혈 위험성 때문에 이전에 허혈성 뇌경색이 있었던 환자에게는 두 약제를 동시에 사용하는 것을 권유하지 않는다. 그리고 이전의 궤양력이 있거나, 항혈소판제제가 필요한 환자에서 위장 출혈의 위험성이 높은 경우(고령, 항응고제, 스테로이드 혹은 비스테로이드성 항염증제, 아스피린을 같이 사용하거나 Helicobacter pylori 감염군)에는 프로톤펌프억제제를 외장관 출혈을 예방하기 위해 같이 사용한다. 이 두 약제를 같이 사용할 때는 임상적인 심혈관계, 위장관계 부작용을 고려하여 득실을 평가하여 사용하여야 할 것이다.