제2형 당뇨병의 병합요법
Combination Therapy in Type 2 Diabetes
Article information
Trans Abstract
Managing type 2 diabetes has become more complex as pharmacotherapy has expanded. Therapies for type 2 diabetes can be divided into drugs facilitating supply of endogenous insulin or those enhancing insulin actions. Successful treatment of type 2 diabetes combines approaches to lifestyle modification frequently in conjunction with use of pharmacologic therapy. The dual aspects of type 2 diabetes, insulin resistance and insulin deficiency, are important factors in therapy selection and the subsequent reponse to therapy. Most patients have gradually increasing needs for additional therapy. Some patients require combination pharmacologic therapy at the time of initial treatment, especially if they have a markedly elevated HbA1c. We describes combination pharmacologic therapy in type 2 diabetes, recent evidence and opinions on sequences for type 2 diabetes. (Korean J Med 2011;80:643-648)
철저한 혈당조절이 당뇨병의 합병증을 예방할 수 있다는 사실은 Diabetes Control and Complications Trial (DCCT)와 United Kingdom Prospective Study (UKPDS) 등 여러 연구에서 확인되었다. 또한 고혈당에 노출되는 기간과 당뇨병 합병증 발생 간의 상관관계를 고려할 때 조기에 적극적인 혈당조절이 요구되고 있다. 경구혈당강하제 병합요법의 목표는 작용기전이 서로 다른 약제를 함께 사용하여 혈당조절을 더욱 효과적으로 하는 데 있다. 각각의 혈당강하제는 서로 다른 작용기전에 의하여 혈당조절 효과를 나타내며 부작용 면에서도 서로 다르다. 서로 다른 기전의 경구혈당강하제를 병합할 때 혈당조절의 효과가 더욱 상승될 수 있으며, 각각의 용량을 줄일 수 있고, 최고용량에 의한 부작용을 최소화 할 수 있다. 이에 저자는 제2형 당뇨병 환자에서 경구혈당강하제의 병합에 대하여 대한당뇨병학회의 당뇨병 진료지침 및 임상연구 결과를 바탕으로 다음과 같이 정리하고자 한다.
대한당뇨병학회 당뇨병 진료지침
2007년 대한당뇨병학회는 당뇨병 진료지침을 통하여 경구혈당강하게 병합요법에 대하여 다음과 같이 권고하였다(Table 1).
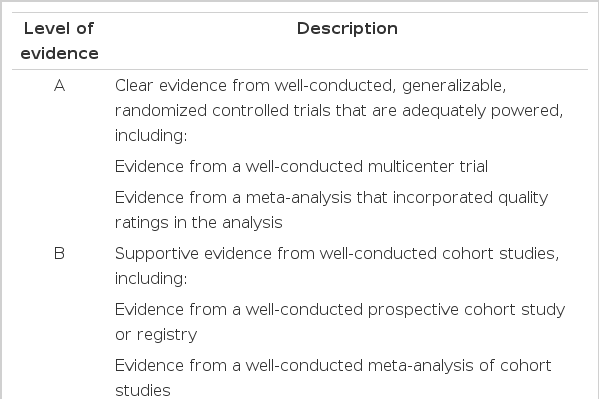
Level of evidence
1) 경구혈당강하제 단독요법의 실패는 2-4개월 이내에 당화혈색소의 목표치에 도달하지 못한 경우로 정의하고 이때는 적극적인 병합요법을 권고한다[B].
2) 단독요법 실패 시 병합요법을 시행한다[A].
3) 단독요법 실패 이전에도 조기 병합요법을 고려할 수 있다[B].
4) 환자에 따라 처음부터 병합요법도 고려할 수 있다[B].
5) 약제의 선택은 환자의 임상적 특성에 따라 개별화한다[B].
6) 병합요법 실패 시 인슐린 치료가 추천되나 환자의 특성과 상황에 따라 약제변경, 3제 복합요법도 고려할 수 있다[C].
조기 병합요법
일반적으로 초기에는 경구혈당강하제 단독요법으로 혈당조절을 시작하나, 단독요법만으로 목표혈당치에 도달하기 어려운 경우 서로 다른 기전의 약제를 병합하는 병합요법이 초기에도 필요할 수 있다. 최근에는 점점 초기 치료로서 병합요법의 유용성이 보고되고 있으며 특히 기저 혈당치가 높은 경우(당화혈색소 9.5% 이상) 처음부터 강력한 병합요법이 장기간의 혈당조절 및 합병증 감소에 효과적이라는 연구결과들이 있다. 대한당뇨병학회의 당뇨병 진료지침에서는 표 2 및 다음과 같이 기저 당화혈색소치가 높은 경우 조기 병합요법을 권고하고 있다.

Treatment guideline of Korean Diabetes Association
1) 당화혈색소치가 7.5-8.5% 일 경우 조기 병합요법을 시작한다.
-
2) 선택할 수 있는 조합
(1) 인슐린 분비촉진제(sulfonylurea, meglitinide) + metformin
(2) 인슐린 분비촉진제(sulfonylurea, meglitinide) + thiazolidinedione
(3) 인슐린 분비촉진제(sulfonylurea, meglitinide) + α-glucosidase inhibitor
(4) thiazolidinedione + metformin
(5) 인슐린 분비촉진제(sulfonylurea, meglitinide) + metformin + thiazolidinedione
-
(6) 고정용량(fixed dose) 복합제
thiazolidinedione (rosiglitazone) + metformin
thiazolidinedione (rosiglitazone) + sulfonylurea (glimepiride)
sulfonylurea (glimepiride, glibenclamide) + metformin
병합요법의 약제선택
어느 약제의 병합이 가장 최선인지에 대해서는 현재까지는 증명된 바가 없다. 환자의 나이, 당화혈색소치, 공복 시 고혈당 정도, 식후 고혈당 정도, 비만여부, 대사증후군 여부, 인슐린 분비능, 간기능 및 신장기능 이상 여부 등 임상적 요소를 고려하여 환자 개개인에 맞는 개별화된 약제가 선택되어야 할 것이다. 그러나 일반적으로 제2형 당뇨병의 발병기전인 인슐린 저항성과 인슐린 분비장애를 고려하여, 인슐린 분비촉진제와 인슐린 감수성 개선제의 병합 및 서로 다른 인슐린 감수성 개선제의 병합이 널리 이용되고 있다. 각 약제들의 병합 시 혈당조절의 효과는 표 3과 같다.
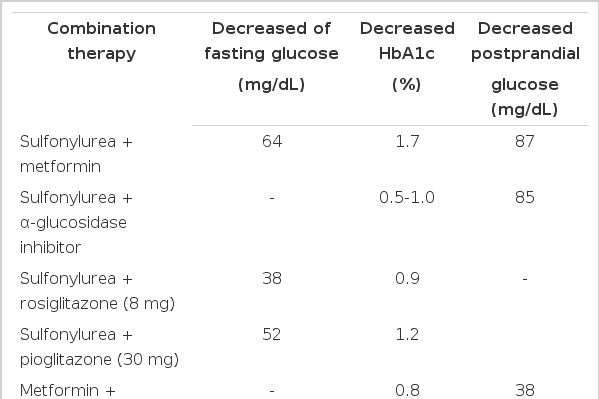
The effect of combination therapy
Sulfonylurea와 metformin 병합요법
가장 많이 사용되는 병합방법으로 그 효과와 안정성이 많이 검토되어 있는 방법이다. 서로 다른 두 가지 약제의 작용기전을 고려할 때 이 두 약제의 조합은 혈당조절에 부가적인 효과를 가져올 수 있으리라 생각한다. Deferonzo 등의 연구에서 glyburide 투여로 혈당조절이 잘 되지 않던 422명의 환자를 대상으로 metformin과 위약을 병합하여 혈당조절 상태를 확인한 결과 위약군에서는 29주 후 공복혈당이 14 mg/dL 증가되고 당화혈색소가 0.2% 증가된 반면 metformin을 추가한 군에서는 공복혈당이 63 mg/dL 감소되고 당화혈색소도 1.7% 감소되었다. 최근에는 제2형 당뇨병 환자의 최초 처방약제로 sulfonylurea와 metformin의 복합정제를 사용하여 우수한 혈당강하 효과를 보였다. 이러한 복합정제의 사용은 편리하며 환자의 순응도면에서도 효과적이다. 기존에 sulfonylurea를 사용하던 환자에서는 기존의 용량을 유지하면서 새로운 약물을 시작용량부터 시작하여 혈당조절 정도에 따라 약제의 용량을 조정한다.
Sulfonylurea와 thiazolidinedione 병합요법
Thiazolidinedione은 인슐린 저항성 개선에 유용한 약제로, 그 효과를 고려할 때 혈당이 잘 조절되지 않는 환자군에서 병합요법에 유용할 수 있다.
Sulfonylurea에 rosiglitazone을 8 mg/일 추가하여 6개월간 치료 시 공복혈당이 38 mg/dL, 당화혈색소는 0.9% 감소되었고, pioglitazone을 30 mg/일 사용한 경우에는 공복혈당이 52 mg/dL, 당화혈색소가 1.2% 감소하였다는 보고가 있다. 이러한 병합 시에는 환자의 체중증가 및 경제적 부담이 고려되어야 한다.
Metformin과 thiazolidinedione 병합요법
인슐린 분비촉진제의 저혈당 발생 가능성은 적극적인 혈당조절의 문제점이 될 수 있어 최근에는 초기 치료약제가 인슐린 분비촉진제에서 인슐린 감수성 개선제로 전환되어 가고 있는 실정이다. 이 두 약제는 상호보완적으로 추가적인 상승효과를 기대할 수 있다. 즉 metformin은 간의 포도당합성을 동시에 억제할 수 있고 여기에 thiazolidinedione을 병용하면 말초조직의 인슐린 저항성을 감소시키므로 효과적이다. 또한 심각한 저혈당을 거의 초래하지 않는다는 것이 가장 큰 장점이며 각각의 약제용량을 줄일 수 있어 위장관계 부작용이나 체중증가, 부종 같은 부작용 발생률이 낮으면서도 서로 약물 상호작용이 없어 유리하다.
16주간 시행된 이중맹검연구에서 metformin과 pioglitazone을 병합한 군에서 대조군보다 당화혈색소를 0.83% 더 감소시킬 수 있었고, 72주간 pioglitazone 45 mg/day을 사용한 연구에서도 당화혈색소를 기저치보다 1.36% 감소시키는 결과를 얻을 수 있었다.
Meglitinide 병합요법
인슐린 분비촉진제인 meglitinide는 작용시간이 빠르고 식후 혈당의 증가를 감소시킬 수 있으며 공복 시에는 저혈당의 위험이 적다는 장점이 있다. Repaglinide는 metformin 단독투여로 혈당조절이 불량한 제2형 당뇨병 환자에서 병합 시 당화혈색소를 1.4% 감소시키는 것으로 보고되었으며, pioglitazone 30 mg/day와 병합하여 사용한 24주의 연구에서도 당화혈색소를 유의하게 감소시키는 것으로 보고되었다. Nateglinide 또한 metformin이나 thiazolidinedione과 병합하였을 때 좋은 효과를 얻을 수 있었다. Nateglinide와 metformin을 병합한 24주 연구에서 병합요법군은 단독요법군에 비하여 공복혈당, 식후혈당, 그리고 당화혈색소 모두 개선된 효과를 보여주었다.
α-glucosidase inhibitor 병합요법
UKPDS연구에서 기존의 약제에 acarbose를 최고용량으로 하루 300 mg 추가하였을 때 대조군에 비하여 당화혈색소가 0.5% 감소하는 것을 알 수 있었다. surfonylurea 단독치료에 실패한 환자를 대상으로 시행된 연구에서도 acarbose 추가 투여는 혈당개선의 결과를 가져왔다.
Acarbose와 thiazolidinedione의 병합요법에 대한 임상연구는 다른 병합요법에 비해 적은 편이다. α-glucosidase inhibitor를 사용하거나 sulfonylurea를 병합하고도 혈당조절이 불량한 제2형 당뇨병 환자에서 pioglitazone을 추가하여 16주간 관찰한 연구에서 혈당조절은 매우 효과적인 것으로 보고되었으며 약간의 부종과 저혈당 외에 큰 부작용은 관찰되지 않았다.
Dipeptidyl peptidase 4 (DPP-4) inhibitor 병합요법
최근 인크레틴에 기반한 여러 약제들이 소개되었고 이 중 dipeptidyl peptidase 4 (DPP-4) 억제제는 DPP-4에 의한 인크레틴의 분해를 차단함으로써 활성형 GLP-1의 혈중농도를 높이고 작용시간을 증가시켜 혈당강하 효과를 나타낸다. 임상에서 사용되고 있는 DPP-4 억제제로 sitagliptin (Januvia)과 vidagliptin (Galvus)이 있으며, 당뇨병 환자의 약제 병용요법에서 이들의 역할이 기대되고 있다. 그러나 DPP-4 억제제와 다른 경구혈당강하제 간의 병용요법의 효과에 관한 연구결과는 많지 않으며, 어느 약제 간의 병용이 가장 효과적인가에 관해서도 현재 불확실하다.
Hermansen 등이 glimepiride로 혈당조절이 되지 않는 환자를 대상으로 24주간 시행한 연구에서 glimepiride에 sitagliptin 100 mg을 병용한 군이 위약을 병용한 군에 비하여 당화혈색소가 0.74% (p < 0.001)감소되었고, 공복혈당은 20.1 mg/dL (p < 0.001)감소되었으며, HOMA 모델을 이용한 베타세포 기능은 12% (p < 0.05) 상승되었다. 그러나 부작용으로 저혈당 발생빈도 및 체중증가는 위약군에 비하여 높았다. Garber 등은 glimepiride로 혈당조절이 되지 않는 환자들에서 vildagliptin 50 mg, 100 mg, 위약을 병용하여 24주간 관찰하였다. 그 결과 vildagliptin 50 mg, 100 mg 병용군에서 위약을 병용한 군에 비하여 당화혈색소가 0.6% , 0.7% 감소하였으나, vildagliptin 50 mg 병용군과 100 mg 병용군 간에는 유의한 차이가 없었다. 동시에 vildagliptin 투여군에서 베타세포기능 및 식후 혈당 개선을 보였다. 흥미로운 사실은 고령이나 당화혈색소가 9% 이상인 경우 혈당강하 효과가 큰 것으로 나타났다. 저혈당 발생빈도는 vildagliptin 병용군이 위약군에 비하여 높았고, 100 mg 투여군이 50 mg 투여군에 비하여 높았다. 체중변화는 vildagliptin 50 mg 병용군과 위약군은 미미한 감소를 보인반면 100 mg 병용군은 위약군에 비하여 유의한 증가를 보였다. 또한 metformin 단독요법으로 혈당조절이 되지 않는 환자들을 대상으로 vildagliptin 50 mg을 병합하였을 때 대조군에 비하여 52주에 당화혈색소가 1.0 ± 0.2% 유의하게 감소되었다.
DPP-4 억제제의 병합요법에 관한 연구 결과가 부족하여 정확한 진료지침을 정하기는 어려우나 DPP-4 억제제가 혈당조절 및 베타세포기능에 도움이 된다는 사실을 감안할 때 병합요법에서 중요한 역할을 할 수 있을 것으로 기대되며 이에 대한 추가적인 연구가 필요할 것으로 생각한다.
3제 병합요법
제2형 당뇨병의 병인에 각각 작용하는 서로 다른 기전의 세 가지 약제를 병합하는 3제 병합요법은 일반적으로 인정된 치료법은 아니지만 또한 금기도 아니다. 세 가지 약제의 조합은 이론적으로 서로 다른 작용기전을 가지고 있으므로 효과가 있을 것으로 생각되고 실제로 흔히 외래에서 이용하고 있는 방법이기도 하다. 그러나 그 효과 면에서는 아직까지 논란의 여지가 있고 비용면에서도 불리하므로 인슐린 치료가 불가능하거나 거부하는 환자에게 주로 권장하고 있다. 향후 그 효능과 실용성에 대한 연구가 더 필요할 것으로 보인다.
제2형 당뇨병의 발병기전을 고려할 때 약제의 병합은 혈당조절에 있어서 많은 이익을 가져올 것으로 예상된다. 최근 조기 혈당조절의 중요성이 부각되면서, 조기 병합요법의 중요성 또한 대두되고 있다. 물론 이러한 조기병합요법에 전혀 문제가 없는 것은 아니며, 약물상호간의 문제점 및 저혈당 발생에 관한 문제 등은 여전히 숙제로 남아있다.
제2형 당뇨병 환자의 특성에 따른 병합요법의 적응증이나 효과에 대한 많은 연구가 필요하며 병합요법별 비교에 관한 더 많은 임상연구가 요구된다. 또한 각각의 약제의 특성을 고려한 환자 개개인에 맞춘 개별화 전략이 필요할 것으로 생각한다.