중탄산염 수액요법과 N-acetylcysteine의 조영제 신독성 예방효과
Intravenous Sodium Bicarbonate and Oral N-acetylcysteinefor the Prevention of Contrast-Induced Nephropathy
Article information
Abstract
목적:
조영제 신독성의 표준 예방법은 식염수(NaCl) 수액요법이지만, 최근 중탄산염 (NaHCO3) 수액요법의 우월성이 보고된 바 있다. 그러나 이에 대한 논란이 있고, N-acetylcysteine(NAC)의 예방효과에 대해서도 분명하게 알려지지 않았다. 본 연구는 중탄산염 단독주입 혹은 NAC와 병합투여가 기존의 식염수 수액요법에 비해 조영제 신독성 예방에 더 효과적인지 조사하고자 하였다.
방법:
예정된 관상동맥조영술을 시행 받는 환자 중 단백뇨, 질소혈증 혹은 당뇨병이 동반된 경우를 대상으로 식염수 투여군, 식염수 + NAC 투여군, 중탄산염 투여군 및 중탄산염+ NAC 투여군으로 무작위 배정하였다. 식염수와 중탄산염 용액은 각각 80 mEq/L 농도로 사용하였고, 조영제 노출 12시간 전부터 조영제 노출 12시간 후까지 투여하였다. 사용한 조영제는 등장성 제제인 Iodixanol였고, 조영제 노출 후 48시간 동안 혈청 크레아티닌 농도가 25% 이상 상승한 경우를 조영제 신독성으로 정의하였다.
결과:
환자는 모두 100명(남자 57명, 여자 43명)이었고, 그중 97명이 당뇨병 환자였으며, 16명에서 조영제 노출 전에 질소혈증이 있었다. 식염수 투여군 24명, 식염수 + NAC 투여군 20명, 중탄산염 투여군 25명 및 중탄산염 + NAC 투여군 31명이었고, 4군의 기저 혈청 크레아티닌은 각각 0.96 ± 0.35 (평균 ± 표준편차) mg/dL, 1.28 ± 0.68 mg/dL, 1.00 ± 0.29 mg/dL, 1.18 ± 0.68 mg/dL로 유의한 차이가 없었다. 조영제 노출 후 48시간 동안 발생한 신독성은 4군에서 각각 4명, 5명, 5명, 6명으로 군 간에 유의한 차이가 없었고, NAC 사용여부에 관계없이 식염수 주입군과 중탄산염 주입군을 비교할 때도 각각 9명, 11명으로서 유의한 차이가 없었다. 기저 혈청 크레아티닌이 높았던(2.11 ± 0.63 mg/dL) 16명 중 3명(19%)에서 신독성이 발생하였고, 기저 혈청 크레아티닌이 정상이었던(0.91 ± 0.21 mg/dL) 84명 중 17명(20%)에서 신독성이 발생하여 경도의 질소혈증 여부에 따른 조영제 신독성 빈도 역시 차이가 없었다.
결론:
중탄산염 수액요법은 식염수 수액요법과 유사한 수준의 조영제 신독성 예방효과를 갖는 것으로 생각된다. 등장성 조영제를 사용할 경우 신독성의 위험도는 기존의 질소혈증 여부에 의해 별로 영향을 받지 않는 것으로 보인다.
Trans Abstract
Background/Aims:
The value of hydration with sodium bicarbonate and N-acetylcysteine(NAC) in the prevention of radiocontrast-induced nephropathy is questionable. This study investigated whether sodium bicarbonate hydration with or without NAC has a more protective role in the prevention of radiocontrast-induced nephropathy than saline hydration with or without NAC.
Methods:
We prospectively studied 100 patients with significant proteinuria (≥ 500 mg/d), azotemia (serum creatinine ≥ 1.5 mg/dL), or diabetes mellitus who were undergoing coronary angiography using iodixanol, a nonionic iso-osmolar contrast agent. Patients were assigned randomly to receive saline infusion (S, n = 24), saline infusion plus NAC (S + NAC, n = 20), sodium bicarbonate infusion (B, n = 25), and sodium bicarbonate plus NAC (B + NAC, n = 31). Contrast-induced nephropathy was defined as an increase of 25% or more in the serum creatinine within 48 hours of contrast exposure.
Results:
There were no significant group differences in age, sex, and basal serum creatinine. Contrast-induced nephropathy occurred in 20 patients (20%) and its incidence was not significantly different among the groups; four from group S, five from group S + NAC, five from group B, and six from group B + NAC. The incidences were not significantly different when compared between S and B, irrespective of the use of NAC (21 vs. 20%), and when compared according to the presence of pre-existing azotemia (19 vs. 20%).
Conclusions:
The efficacy of sodium bicarbonate hydration in the prevention of contrast-induced nephropathy seems comparable to that of saline hydration, and it was not improved by the addition of NAC. (Korean J Med 2011;80:537-545)
서 론
조영제 신독성(contrast-induced nephropathy)은 방사선 영상을 위해 사용하는 조영제에 노출된 후 발생하는 급성신손상(acute kidney injury)이다. 이는 입원 환자에서 발생하는 급성신부전의 10% 이상을 차지하고, 입원기간 장기화, 투석 필요 혹은 사망의 요인이 될 수 있다[1]. 조영제 노출 후 신독성이 발생하는 빈도는 대상 환자, 방법 또는 진단기준에 따라 차이가 많지만 일반인에서 2%, 고위험군에서는 50%까지 보고되고 있다[2-4]. 고위험군에는 신부전, 체액결핍, 당뇨병, 울혈성 심부전, 빈혈, 고령 환자 등이 속하고, 투여된 조영제 양이 많거나 조영제를 72시간 이내 반복 사용하는 경우에 조영제 신독성의 빈도가 증가한다고 알려졌다[5].
조영제 신독성의 발생기전으로서 신세관 독성, 허혈 손상, 허혈 후 활성산소(reactive oxygen species), 산화스트레스 (oxidative stress) 혹은 유리기(free radical)에 의한 재관류 손상이 중요하게 작용한다[5-8]. 따라서 이러한 기전을 차단하는 방법을 조영제 신독성 예방에 적용할 수 있으나, 이제까지 그 효과가 정립된 것은 식염수(NaCl) 수액요법뿐이다[6-8]. 항산화제인 N-acetylcysteine(NAC)이 활성산소를 제거시킴으로써 조영제 신독성을 예방할 수 있다는 보고가 있지만[9-11] 표준요법으로 사용하는 데는 논란이 있다[12]. 또한 유사한 근거로서, 중탄산염(NaHCO3) 수액요법이 유리기 생성을 억제하여 조영제 신독성 예방 효과가 있다는 보고가 있지만 아직 분명하지 않다[13-17]. 저자들은 중탄산염 수액 단독주입 혹은 NAC와 병합투여가 기존의 식염수 수액요법과 비교하여 조영제 신독성 예방에 더 효과적인지 알아보고자 하였다.
대상 및 방법
대상
2005년 4월부터 12월까지 한양대학교병원에 입원하여 관상동맥조영술이 예정된 환자 중에서 1) 단백뇨 500 mg/d 이상, 2) 혈청 크레아티닌 1.5 mg/dL 이상, 혹은 3) 인슐린이나 경구혈당강하제를 투여 중인 당뇨병 환자를 대상으로 하였다. 최근 24시간 동안 혈청 크레아티닌이 0.5 mg/dL 이상 증가한 급성신부전 혹은 진행된 만성 신부전(혈청 크레아티닌 > 8.0 mg/dL) 환자, 혈액투석 혹은 복막투석 중인 환자, 응급 심도자술을 시행 받은 경우, 최근 2일 이내 조영제에 노출된 경우, 조영제 알레르기가 있는 환자, 임신한 경우 등은 대상에서 제외하였다. 본 연구는 한양대학교병원 임상연구심의위원회의 심의를 거치고, 환자들로부터 동의를 구한 후 시행되었다.
방법
대상 환자들을 식염수 투여군(n = 24), 식염수 + NAC 투여군(n = 20), 중탄산염 투여군(n = 25) 및 중탄산염 + NAC 투여군(n = 31)으로 난수표를 이용하여 무작위 배정하였다. 식염수 주입은 5% 포도당 용액 1 L에 NaCl 80 mEq를 혼합하여 1 mL/kg/hr 속도로 조영제 노출 12시간 전부터 조영제 노출 12시간 후까지 정맥주사 하였다. 중탄산염 주입은 5% 포도당 용액 1 L에 NaHCO3- 80 mEq를 혼합하여 1 mL/kg/hr 속도로 조영제 노출 12시간 전부터 조영제 노출 12시간 후까지 정맥주사 하였다. NAC는 Muteran® (한화제약, 서울, 대한민국) 600 mg을 조영제 노출 전후 2일에 걸쳐 1일 2회 경구 투여하였다. 이뇨제를 처방 받던 환자들에서는 검사 전날부터 그 투여를 중단하였다.
대상 환자에서 연구기간 동안 혈청 크레아티닌의 변화를 추적하였고, 조영제 노출 후 48시간 내에 혈청 크레아티닌이 기저치에 비해 25% 이상 상승한 경우를 조영제 신독성으로 정의하였다[13]. 질소혈증은 혈청 크레아티닌 농도 1.5 mg/dL 이상을 기준으로 삼았고, 사구체여과율 추정치(estimated glomerular filtration rate, eGFR)는 MDRD-2 공식(estimated GFR = 186 × serum creatinine-1.154 × age-0.203 [×0.742, if female])을 이용하여 계산하였다. 한편, 조영제 신독성의 위험도 점수(contrast-induced nephropathy risk score)를 Mehran 등이 소개한 A모델에 따라 산정하였다[2]. 즉, 심장성 쇼크 5점, 대동맥내 풍선펌프 삽입 5점, 울혈성 심부전 5점, 혈청 크레아티닌 >1.5 mg/dL 4점, 연령 >75세 4점, 빈혈 3점, 당뇨병 3점, 조영제 용량 100 mL당 1점으로 계산하였고, 합산하여 5점 이하이면 저위험군, 6내지 10점이면 중등도 위험군, 11내지 15점이면 고위험군, 16점 이상이면 최고위험군으로 분류하였다[2].
심도자술에 사용한 조영제는 비이온 등장성 이량체(nonionic iso-osmolar dimer)인 iodixanol (Visipaque®, GE Healthcare, Princeton, United Kingdom)였다. Briguori 등[18]의 보고에 따라 조영제 주입의 고부하 기준을 140 mL로 하였다.
통계 분석
모든 연속 자료는 평균 ± 표준편차로 기술하였다. 식염수 투여군, 식염수 + NAC 투여군, 중탄산염 투여군 및 중탄산염 + NAC 투여군 사이의 비교는 Kruskal-Wallis test를 이용하여 검정하였고, 두 군 사이의 비교를 위하여 Mann-Whitney U test를 이용하였다. 카테고리 자료의 경우는 chi-square test를 이용하여 두 변수 사이의 연관성 혹은 군 간의 차이를 조사하였다. 통계 분석을 위하여 Statview 5.0 (Abacus Concepts Inc., Berkeley, USA)을 사용하였고, p 값 0.05 미만일 때 통계적으로 유의하다고 판정하였다.
결 과
환자의 일반적 특성
전체 환자 100명의 평균 연령은 65 ± 11세(41-85세)였고, 여자 43명과 남자 57명이었다. 그중 97명이 당뇨병 환자였고, 16명에서 조영제 노출 전에 질소혈증이 있었다.
표 1에 대상 환자의 일반적인 기초 특성들이 요약되어 있다. 환자의 연령, 성별, 주요 동반질환, 복용 약제 및 조영제 신독성 위험점수[2] 사이에 유의한 차이는 없었다. 헤마토크릿과 빈혈(남자, 헤마토크릿 < 39%; 여자, 헤마토크릿 < 36%) [2]의 빈도 차이는 각 군 사이에 유의하지 않았으나, 헤모글로빈이 중탄산염 + NAC 투여군에 비해 중탄산염 투여군에서 높았고 헤모글로빈 A1c는 식염수 투여군에 비해 중탄산염 + NAC 투여군에서 높았다. 경피적 관상동맥중재술(percutaneous coronary intervention, PCI)을 시행 받은 환자의 수와 시술 중 사용한 스텐트의 개수, 심박출계수(ejection fraction) 등 심장관련 지표들 사이에 유의한 차이는 없었다. 조영제 사용량이 군 간 차이를 나타내어 식염수 투여군에 비해 중탄산염 + NAC 투여군에서 유의하게 많았다(170 ± 81 vs. 263 ± 115 mL, p< 0.05). NAC 사용여부와 관계없이 두 수액 주입군을 비교했을 때 역시 식염수 주입군에 비해 중탄산염 주입군에서 조영제 사용량이 유의하게 많았다(189 ± 98 vs. 243 ± 121 mL, p< 0.05).
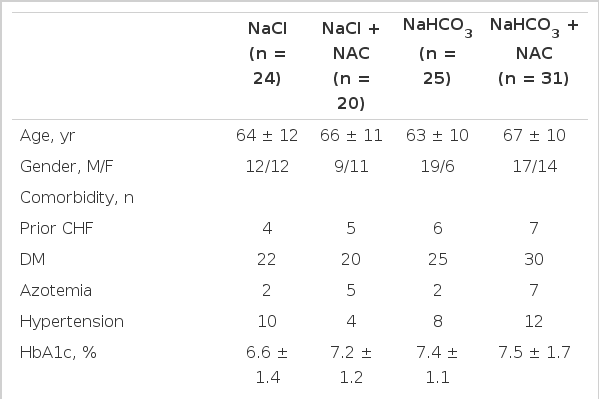
The basal characteristics of each group of patients
조영제 신독성의 발생
조영제 노출 후 48시간 내에 혈청 크레아티닌 농도가 25% 이상 증가하여 신독성이 발생한 환자는 모두 20명으로서 그 빈도가 20%였다. 각 군별로 식염수 투여군 4명(17%), 식염수 + NAC 투여군 5명(25%), 중탄산염 투여군 5명(20%), 중탄산염 + NAC 투여군 6명(19%)으로서, 각 군 사이에 유의한 빈도 차이가 없었다. 또한 조영제 신독성의 기준을 여러 가지로 달리하여 조사하였다(Table 2). 조영제 노출 후 48시간 내 사구체여과율 추정치 25% 이상 감소한 경우, 혈청 크레아티닌 농도 0.5 mg/dL 이상 증가한 경우, 그리고 혈청 크레아티닌 농도 0.5 mg/dL 이상 증가하거나 25% 이상 증가한 경우 등 세 가지 다른 기준에서도 각 군 사이에 유의한 차이가 없었다.

Occurrence of contrast-induced nephropathy according to different criteria
표 3에 조영제 노출 전후 각 군의 혈청 크레아티닌 변화가 제시되어 있다. 기저 혈청 크레아티닌과 조영제 노출 24시간 및 48시간 후 혈청 크레아티닌 농도는 네 군 사이에 유의한 차이가 없었다. NAC 사용 여부에 관계없이 식염수 주입군과 중탄산염 주입군을 비교했을 때 조영제 신독성 발생 환자는 각각 9명(21%), 11명(20%)으로 그 빈도에 차이가 없었다. 또한 주입한 수액의 종류에 관계없이 NAC 사용 여부에 따라 두 군으로 나누어 비교했을 때 조영제 신독성 발생이 각각 11명(22%)과 9명(18%)으로 역시 유의한 차이가 없었다.
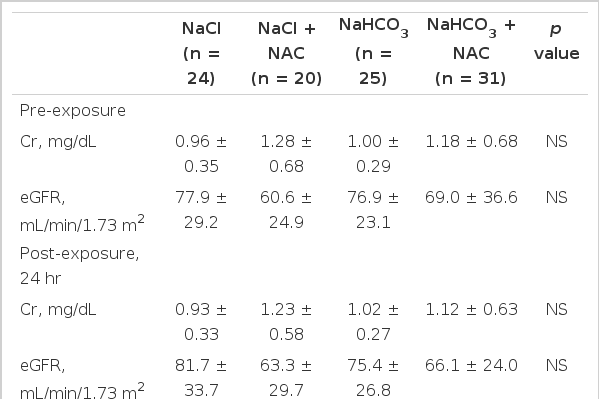
Pre- and post-exposure serum creatinine concentrations and eGFR from each group of patients
조영제 신독성 발생의 위험인자로서 기저 질소혈증 여부와 조영제 사용량에 따라 조사하였다. 조영제 노출 전부터 질소혈증이 있었던 환자는 모두 16명이었고, 기저 혈청 크레아티닌 농도는 2.11 ± 0.63 mg/dL였으며, 그 중 3명(19%)에서 조영제 신독성이 발생하였다. 이에 비해, 조영제 노출 전 질소혈증이 없었던 환자 84명의 기저 혈청 크레아티닌은 0.91 ± 0.21 mg/dL였고, 그중 17명(20%)에서 조영제 신독성이 발생하여 경도의 질소혈증 여부에 따른 조영제 신독성 빈도 차이는 없었다. 표 4에 조영제 신독성이 발생한 환자의 혈청 크레아티닌 경과가 제시되어 있다. 조영제 주입량의 중앙값을 기준으로 조영제 주입량에 따른 조영제 신독성의 빈도를 비교하였다. 조영제 양이 200 mL 이하였던 55명 환자 중 14명(25.5%)과 200 mL를 초과한 45명 환자 중 6명(13.3%)에서 각각 조영제 신독성이 발생하였으나 그 차이는 통계적으로 유의하지 않았다.

Pre- and post-exposure serum creatinine concentrations and eGFR from patients with CIN in each group
고 찰
조영제 신독성을 예방하기 위한 식염수 수액요법은 체액을 증가시켜 바소프레신 분비를 억제하고 혈관확장물질인 프로스타글란딘 합성을 증가시키며, nitric oxide 소실을 줄여 신혈관 수축으로 인한 허혈성 손상을 차단하는 효과가 있다[19,20]. 그러나 식염수 수액요법의 이상적인 투여방법, 기간 및 속도에 대해서는 아직 분명하게 알려지지 않았다. 항산화제인 NAC는 nitric oxide와 결합하여 더 안정되고 강력한 혈관확장효과가 있는 S-mitrosothiol을 형성할 뿐 아니라, nitric oxide 합성을 증가시켜 신장혈류를 개선시킨다[21]. 그러나 NAC의 조영제 신독성 예방효과에 대한 여러 연구 결과는 일관되지 않아서 그 신독성 예방효과가 분명하지 않다[9-12]. 본 연구에서도 NAC 사용 여부에 따른 조영제 신독성 예방효과는 유의한 차이가 없었다.
중탄산염은 신세관의 pH를 올려서 유리기 산소의 생산을 억제하고, nitric oxide와 관련하여 생산되는 oxidant perixynitrate를 제거함으로써 조영제 신독성 예방효과를 기대할 수 있다[13]. 이는 처음에 신부전 동물모델에서 소개되었고[22,23], 임상 연구에서도 식염수 수액요법에 비해 중탄산염 수액요법이 우수하다는 결과가 보고되었다[13-17]. 그러나 본 연구에서는 두 수액요법의 예방효과에 유의한 차이가 없었다.
표 5에 최근까지 출판된 중탄산염 수액요법의 조영제 신독성 예방효과에 대한 임상시험이 요약되어 있다. 이들은 서로 상반된 결과로서 일치하지 않는다[13-17,24-26]. 중탄산염 수액요법의 예방효과에 대해 부정적인 결과를 보고한 연구들은 상대적으로 기저 혈청 크레아티닌이 낮고, 응급 심혈관조영술 환자가 포함되지 않았으며, 등장성 조영제를 사용하거나 조영제 사용량이 상대적으로 적은 특징이 있다[24-26]. 본 연구 결과도 이에 부합한다. 즉, 신기능장애가 뚜렷하지 않은 환자에서 비이온성 등장성 조영제를 사용할 경우에는 중탄산염 수액요법과 식염수 수액요법이 서로 유사한 조영제 신독성 예방효과를 나타낼 것이다.

Studies reporting the use of sodium bicarbonate to prevent contrast-induced nephropathy
최근에는 완전한 논문으로 출판된 결과 외에 초록으로 발표된 경우까지 모두 포함하여 조사한 메타분석들이 보고되고 있다[27-35]. Hoste 등은 만성신부전 환자 혹은 응급 심혈관조영술의 경우에 중탄산염 수액요법의 예방효과가 선택적으로 우수하다고 하였고[27], Brar 등은 중탄산염 수액요법이 우월하다고 보고한 경우는 대부분 규모가 작은 연구라고 하였으나[28], 대부분의 메타분석에서 중탄산염 수액요법의 조영제 신독성 예방효과를 긍정적으로 결론지었다[27,29-35]. 메타분석의 경우 출판에 의한 편향(publication bias)을 보완할 수 있으나, 출판되지 않은 연구까지 포함하는 과정에서 대상과 방법의 이질성이 더욱 커지는 문제가 있다.
조영제 신독성의 위험인자로서 기저 신부전, 체액결핍, 당뇨병, 울혈성 심부전, 빈혈, 고령 환자 및 다량 혹은 반복적인 조영제 노출 등이 알려졌다[5]. 본 연구에서도 당뇨병이나 질소혈증 환자 등 고위험군을 대상으로 하였고, 따라서 조영제 신독성의 빈도가 비교적 높았다. 대상 환자의 대부분이 당뇨병이었던 것은 관상동맥 질환 유병과 관련 있을 것으로 생각한다. 기저 질소혈증 여부에 따른 조영제 신독성 발생 차이가 유의하지 않은 것은 기저 질소혈증의 정도가 심하지 않은 대상 환자의 특성과 관련 있을 것이다[27]. 또한, 조영제 사용량에 따른 조영제 신독성 빈도 역시 유의한 차이가 없었다. 이는 본 연구에서 조영제 신독성 발생 가능성이 비교적 작은 비이온성 등장성 조영제를 사용하였고, 신기능이 비교적 양호한 환자들이 대상에 포함되었기 때문으로 생각한다[36,37].
본 연구는 무작위 실험이었으나, 조영제 사용량이 환자군 사이에 유의한 차이를 보였다. 중탄산염 투여군에서 조영제 사용량이 많았음에도 불구하고, 신독성 발생 빈도가 증가하지 않은 것은 중탄산염 수액요법이 적어도 식염수 수액요법과 동등한 수준의 조영제 신독성 예방효과를 갖는다는 사실을 시사한다. 대상 환자 수가 많지 않았던 것이 이 연구의 제한 점이지만, 유의수준(α-error) 0.05로서 양측검정을 시행하였을 때 본 연구의 네 군 환자 수 및 각각의 조영제 신독성 빈도는 통계적 검정력(power) 0.788로 산출되어 비교적 유의하였다고 판단된다. 향후 더 많은 환자를 대상으로 만성신부전 등 위험인자가 있을 때 그 효과를 검증할 필요가 있다. 특히, 중탄산염 수액의 농도, 주입속도 및 투여시기에 대하여 정립되어야 한다.