고혈압의 최신진료지침과 약제선택
Current Guidelines for Hypertension Control and Choice of Antihypertensive Drugs
Article information
Trans Abstract
According to the mata-analysis on the management of hypertension and guidelines published in recent years concluded that the amount of blood pressure reduction, not the choice of antihypertensive drug is the major determinant of reduction in cardiovascular morbidity and mortality in the both younger and older partients with hypertension, However still remained the some patients having an indication for a specific drug or drugs that is helpful to those of the patients with diabetes, chronic kidney disease, ischemic heart disease, heart failure or atrial fibrillation. Thus, individualized, tailored drug therapy would be preferred to stepped care approach in the management of essential hypertension. (Korean J Med 2011;80:280-285)
서 론
현재까지의 많은 연구를 종합적으로 분석하면 고혈압과 관련되는 심혈관 사망, 전체사망, 심혈관사고 등의 예후에 가장 중요한 것은 강압의 정도이지 혈압약의 종류가 아니라는 의견이 지배적이다. 그렇지만 최근의 연구들에 의하면 다양한 심혈관 질환의 위험인자를 갖고 있는 위험군에서는 각 군 별로 다른 작용기전의 약제를 사용하는 것이 좋고 고위험군일수록 낮게 조절하는 것이 좋아서 고혈압의 정도와 위험인자를 파악하여 군별로 일차약제를 선택하는 것이 이상적이다고 할 수 있다(Table 1) [1-4].
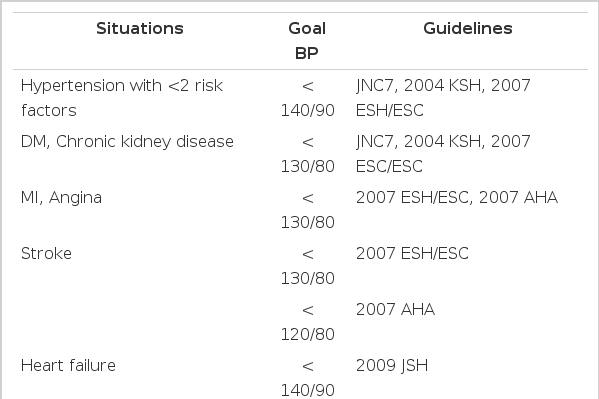
Goal blood pressure according to the guidelines in various situations
대표적인 고혈압치료 지침
대한고혈압학회 지침 2004: (JNC 2003)
미국의 합동위원회(JNC 7)의 권고를 따라서 제정하였으며 개원의들에게 단순화시킨 분류를 제공함으로써 고혈압의 관리율을 높이려는 목적이다. 혈압의 정도를 제1기와 2기로 나누고 임상질환, 표적장기 손상 등에 따라 특정군을 정하고 강제적응으로 일차 선택약제를 고르고, 강제적응이 아닌 일반환자에게는 더욱 간편하게 제1도 고혈압(≥ 140/90 mmHg)에서는 thiazide 이뇨제를 처음 선택하고 더 필요 시 다른 5 약제 중 한 가지의 병용을 권고하고 제2도 고혈압(≥ 160/100 mmHg)에서는 처음부터 이뇨제를 포함한 두 가지 약제를 사용하도록 권고하였다. 물론 고혈압 전단계에서도 당뇨병, 만성콩팥병이 있는 경우는 목표혈압을 130/90 mmHg 미만으로 하고 단백뇨가 1일 1 g 이상인 경우 125/75 mmHg 미만으로 권고하였다(Fig. 1) [1].
Algorithm for treatment of hypertension (JNC 7). CKD, chronic kidney disease; HT, hypertension.
주로 ALLHAT연구 결과를 근거로 하였으며 이는 대규모 관동맥 위험군 환자에서 네 가지의 약제를 서로 비교하였는데 이뇨제인 chlorthalidone, 칼슘차단제 amlodipine, ACE 차단제 lisinopril, 알파차단제 doxazosin으로, doxazosin은 심부전의 위험이 증가하여 조기에 중단하였으며, 4.9년을 추적하던 중 일차종결점인 치명적 관동맥 질환, 비치명적인 심근경색은 나머지 세군에서 비슷하였으나 심부전위험은 chlorthalidone이 amlodipine과 lisinopril에 비해서 낮았으며 복합 심혈관종결점도 lisinopril보다 현저히 낮았다[5,6]. 결국 chlorthalidone은 강압효과가 더 빠르고 좋았으며 이는 장기작용 때문으로 볼 수 있다. 그러나 실제로 국내에는 주로 단기작용의 dichlozid가 사용되기 때문에 같은 결과를 기대할 수는 없다. 또 ACCOMPLISH 연구에서는 dichlozid 사용군에서는 혈압이 더 낮게 조절되었지만 칼슘차단제(CCB) 사용군에 비해 더 나쁜 심혈관종결점을 보인것은 dichlozid의 부작용 때문이라고 볼 수 있겠다[7,8].
결국 강제적응이 없는 경우에 처음약으로 반드시 thiazide를 쓰라고 권고했던 JNC 7은 재고해야할 것으로 생각된다. 이뇨제를 사용한다면 강력하고 장기 작용인 소량의 chlorthalidone을 고려할 수 있는데 반드시 저칼륨혈증, 내당능저하, 고뇨산혈증 등을 조심해야 된다. 노인의 경우에는 목표혈압의 10 mmHg 이내 높은 경우는 소량의 dichlozid를 사용할 수도 있겠다. JNC 7에서 정한 강제적응은 표 2와 같다[1].

Compelling indications for individual drug class (JNC 7)
유럽 심장학회 고혈압학회 지침(ESH/ESC) 2007
혈압의 높은 정도와 심혈관계 위험인자 0, 1-2개, 3개 이상 혹은 대사증후군, 표적장기손상, 당뇨병, 또 심혈관계 및 신장질환의 동반에 따라서 평균, 저위험, 중위험, 고위험, 최고위험의 5단계로 나누어 고위험군에서부터 약물치료를 하는것으로 적용이 복잡하다. 즉, 높은 정상군도 당뇨병이 있으면 약물치료 대상이며 2도 고혈압도 위험인자 2 미만이면 생활요법을 권고하였다. 임상증세별 우선약제의 선택은 좋은 참고사항이다(Table 3).

Position statement: Antihypertensive treatment: Preferred drugs
초기 치료약제로는 다섯 가지의 약제군, 즉 이뇨제, 베타차단제, 칼슘차단제, ACE 차단제, ACE수용체 차단제 가운데 하나를 경도, 저위험군에서는 저용량으로 시작할 수 있으며 목표혈압이 안되면 전용량 또는 대체약제를 권고하며, 2도 고혈압이상 또는 고위험군일 경우는 처음부터 두 가지 약제의 저용량 병합요법을 시작하고 목표가 안되면 전용량 또는 세 번째 약을 저용량 추가하는 순서를 권고하였다(Figs. 2 and 3) [3].
Monotherapy versus combination therapy strategies (ESC 2007).
Possible combination between antihypertensive drugs, preferred combinations are represented as thick lines.
영국심장학회 지침(BHS) 2008
유색인종과 백인, 또 55세를 기준으로 고령과 유색인에서는 이뇨제 또는 칼슘차단제를 백인, 약년자에게는 ACE 차단제(ACE), ACE 수용체차단제(ARB)를 일차약으로 권고하고 제 2단계로 ACE나 ARB에 칼슘차단제 혹은 이뇨제를 병용하고 제3단계에서 A+C+D 3자 병용을 권고하였으며 제4단계에서 알파차단제나 베타차단제를 선택하도록 해서 당뇨병의 발생 을 증가시키는 베타차단제를 일차약에서 제외시켜서 많은 논란이 되고 있지만 새로운 베타차단제의 출현으로 장기 결과가 주목된다(Fig. 4) [9].
NICE/BHS Guideline, 2006. C, calcium channel blocker; D, thiazide diuretics; BB, beta blockers; NICE, national institute for health and clinical excellence; BHS, British hypertension society.
특정 약제별 적응증
ACE차단제
모든 심부전환자, 무증상성성 좌심실 기능부전, 와 ST상승 심근경색증, 비 ST상승 전벽경색증, 당뇨병, 수축기심부전, 단백뇨성 만성콩팥병 등이다. HOPE, EUROPA 연구 등이 바탕이 되었으며 물론 강압효과가 가장 중요하지만 여러 증거로 심장, 신장, 뇌 등의 장기보호 효과가 있다고 알려져 있다[10,11].
Angiotensin II 수용체 차단제(ARB)
상기의 ACE 차단제의 적응증과 비슷하지만, LIFE 연구에서 좌심실비대를 동반한 중증고혈압에서 효과적이었다. 물론 기존에 ACE차단제 사용자에서는 대체할 필요는 없지만 기침 등으로 인하여 부적응이 있을 때는 ARB로 대체해야 된다[12-14].
Thiazide 이뇨제
가장 이상적인 약제로 chlorthalidone 12.5~25 mg이다(클로르타리돈®, 하이그로톤®). 장기작용으로 dichlozid 효과의 두배가 되므로 25, 50 mg 두 가지 용량이 있어서 필요시 절반으로 사용해야 된다. 심부전환자나 만성 콩팥병에서 용적조절용으로 사용될 수 있으며 루프 이뇨제의 차선으로 사용될 수도 있다. 알도스테론 길항제는 신장기능이 유지되고 있는 진행성 심부전이나 저칼륨혈증이 있을 때 사용할 수 있다. 국내에서는 dichlozid 12.5 mg가 가장 많이 사용되며 일부 고정병합제제에 포함되어 있기 때문에 편리한 점도 있지만 용량조절에는 제한이 있다.
칼슘차단제(CCB)
장기작용형 dihydropyridine이 추천되며, non-dihydropyridine인 diltiazem, verapamil은 심방세동환자와 협심증에서 심박수조절 목적으로 사용될 수 있다. 또 폐쇄성 폐질환이 동반될때 사용할 수 있다[3,5,15].
베타차단제
급성심근경색증 후에 내인성 교감신경작용이 없는 약제를 사용 할 수 있다. 심부전과 무증상성 좌심부전에서는 극소량으로 사용해서 심기능의 악화를 예방해야 된다. 물론 심장세동, 협심증에서 맥박수 감소목적으로 사용된다. 위의 경우가 아닌 경우는 일차약으로 베타차단제는 금기인데, 특히 60세 이상에서 타약제와 비교시에 관동맥 질환, 뇌졸중, 심혈관사고를 증가시키며 사망률도 약간 증가시킨 보고가 있었다. 또 내당능을 감소시키고 새로운 당뇨병진단을 증가시킨다. 물론 혈관확장성 베타차단제인 carvediolol과 nebivolol은 예외다[16,17].
알파차단제
ALLHAT 연구 결과 심부전위험을 증가시켜 조기에 중단하였으며 초기 단독요법으로는 제외되었으나 노인에서 전립선비대가 있고 심혈관 위험이 높지 않을 때 사용할 수 있다[5].
이상적인 약제의 선택
초기 단독요법
단순 수축기 및 확장기 고혈압은 140/90 미만, 일부 고위험군에서는 130/80 미만을 목표로 하지만 노인성 수축기고혈압에서는 확장기압을 65 mmHg 미만으로 해서는 안된다. 또 일반적 원칙으로 목표보다 20/10 mmHg 이상인 경우는 처음부터 2제 병용요법이 좋다. 여러가지 메타분석을 결론해 보면 강압제 반정은 한정의 약 70~80%의 효과를 갖지만 부작용은 절반에 미치기 때문에 저용량 병용요법이 비용 효과적으로 좋다. ACE, ARB를 제외하고는 용량 증가시 부작용이 많았다. 따라서 chlorthalidone 12.5에서 25 mg으로 amlodipine 5 mg에서 10 mg으로 용량증가는 권고하지 않는다. 단일 약제에 반응이 없어 다음단계를 고려할 때 용량을 증가보다는 타약제로 대체하는것이 50%의 치료확률, 제3제로 대체시 약 60~80%의 치료확률을 증가시킬 수 있다.
약제의 선택
각각의 환자에 특별히 반응이 좋은 개인차가 있다. 강제적응증이 없는 경우 초기 단독요법제로 thiazide 이뇨제, 장기작용 CCB (dihydropyridine), ACE차단제 혹은 ARB가 있으며, 세 가지는 모두 강압효과가 비슷하다고 볼 수 있다. 베타차단제는 강제적응 외에는 사용하지 않는다 특히 노인에서 부작용이 많다. JNC 7 이후로 저용량의 thiazide가 널리 사용되고 있지만 그러나 작용이 짧고 효과가 약하기 때문에 chlorthalidone 저용량이 더 추천된다. 나이와 인종에 따른 차이를 보면 젋은 환자는 ACE나 ARB에 반응이 좋다. 흑인과 노인에서는 thiazide와 장기작용 CCB가 더 좋은데 아마도 혈장 PRA가 낮기 때문일 것이다. 그러나 노인에서도 심부전, 심근경색후, 단백뇨를 동반한 콩팥병에서는 ACE차단제나 ARB가 유용하게 사용될 수 있다(Figs. 2-4).
용량과 횟수
다음 용량 투여 전인 아침혈압이 가장 높을 수 있으며 아침에 합병증의 발생이 높기 때문에 장기 작용의 약제를 선택해야 하며 1일 2회 요법도 피크효과는 적지만 지속효과를 볼 수 있기 때문에 고려할 수 있다.
병합요법
일차요법으로 병합요법
처음부터 목표혈압의 20/10 mmHg 높은 경우에 고정용량 병합요법은 소량으로 효과적이며 부작용도 적다. 그러나 노인과 당뇨병이 있는 경우 기립성 저혈압 발생이 쉽기 때문에 조심해야 한다. ACCOMPLISH 연구결과를 볼때 ACE와 thiazide로 조절이 되는 환자도 장기작용형 CCB로 대체를 하는 것도 고려할 수 있겠다.
결 론
최근의 2007 ESH/ESC 지침, 2009년 메타분석 등의 결과를 보면 전체 연령군에서 심혈관 위험의 감소는 특정 약제가 아니고 강압의 정도 때문으로 보고있다. 물론 심혈관 위험이 높은 군에서도 마찬가지였다. 그러나 병용요법에서는 다르며 ACCOMPLISH 연구를 보면 평균혈압이 약간 높았던 ACE, CCB 군에서 더 효과가 좋은것을 보면 약제의 차이가 있음을 시사한다. 또 특정한 상태에서 맞는 약제가 있기 때문에 위에 열거한 어느 한 가지 지침보다는 환자 개개인의 특성에 따른 약제의 선택과 치료목표가 다르게 적용되어야 할 것이다.