노인 환자의 항생제 치료 원칙
Principles of antimicrobial therapy in elderly patients
Article information
Trans Abstract
Older persons generally have greater susceptibility to infections than younger adults, probably because of the increased frequency of comorbidities and physiologic changes. There are many factors, both patient-related and treatment-related, which contribute to unique aspects of antimicrobial use in elderly persons that make prescribing complicated. Physiologic and pharmacokinetic changes associated with aging results in a higher risk of an adverse drug event and a harmful drug interaction, making antimicrobial dosing difficult. The risk of polypharmacy and more frequent adverse drug reactions in the elderly population justify a thorough consideration of the patient’s true need for antimicrobial therapy. Given the increase in the elderly population and in the incidence of adverse drug reaction among elderly persons, further efforts should be made to optimize approach to management of infectious diseases in elderly persons. (Korean J Med 79:362-365, 2010)
서 론
인간의 기대 수명이 점차 증가함에 따라 노인 인구가 해마다 증가하고 있으며, 노인 환자들에 대한 적절한 의료 서비스를 제공하는 것이 21세기 의학의 중요한 이슈가 되었다. 젊은 연령층의 환자들에 비해서 노인 환자들은 더 흔하고 심하게 질병을 앓는 경향이 있으며 이는 감염 질환에서도 마찬가지이다. 폐렴, 독감, 요로감염에 의한 균혈증 등이 흔하게 발생하고 중증으로 발생하여 높은 사망률을 나타낸다1). 따라서 노인 환자들은 항생제 처방을 받는 경우가 흔하다. 노인 환자에서 항생제를 투여할 때 연령의 증가에 따른 생리학적인 변화, 약력학/약동학적인 변화, 부작용의 증가 가능성, 기존에 투여받고 있던 약물과의 상호작용 등을 면밀하게 고려하는 것이 필요하다2).
노인 환자들의 생리학적인 변화에 따른 약력학적 변화
연령이 증가함에 따라 생리학적인 변화가 발생하고 이에 따라 약물의 약력학적인 지표에 변화가 발생한다. 항생제의 경우도 마찬가지이며 이러한 변화의 정도는 개인차가 있다. 노인 환자에서 흔하게 발생하는 생리학적인 변화와 약력학적인 변화를 표 1에 기술하였다2).
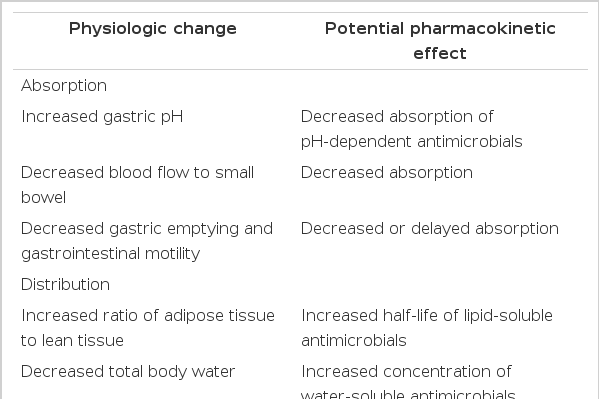
Physiologic and pharmacokinetic changes in elderly patients
약물 흡수
약물의 흡수 자체는 나이가 들어도 감소하지 않는다. 하지만 연령이 증가함에 따라 위산 분비가 감소하며, 이에 따라 약물 흡수가 영향을 받을 수 있다. 위 내 pH 증가에 따라 약물 흡수가 감소되는 대표적인약물은 itraconazole, ketoconazole, sulfonamide, dapsone, pyrimethamine, atazanavir 등이 있다. 내장혈관의 혈류가 감소하고 위장관 운동이 감소하게 되어 ciprofloxacin 같은 약물의 흡수가 감소될 수 있다3).
약물 분포
연령이 증가함에 따라 체내에 지방조직이 차지하는 비율이 증가하고 수분량이 감소하며 알부민 수치가 감소한다4). 수용성 약물의 분포용적은 줄고, 지용성 약물의 분포용적은 늘어남으로써, 지용성 약물의 효과가 늦게 나타나고 부작용도 여러 차례 투여한 이후에야 나타나는 경우가 있다. 알부민이 감소하면서 알부민에 결합하는 약물들의 자유형(free form)이 증가한다. 자유형 약물의 혈중 농도가 높아지면서 약물 독성이 나타날 가능성이 높아진다. 간, 신장으로 가는 혈류가 감소하여 약물의 간 대사 및 신장 배설이 감소하며 이에 따라 aminoglycoside, β-lactams, vancomycin, daptomycin, amphotericin B 등의 약물의 부작용이 증가할 수 있다.
신장을 통한 약물 배설
사구체 여과율이 신장 기능의 중요한 지표로 사용된다. 노인 환자들의 사구체 여과율은 젊은 환자들에 비해 절반 가량 감소되어 있는 것으로 보고되며, 연령이 증가함에 따라 사구체 여과율이 더욱 감소한다5). 젊은 연령층의 환자에서는 혈청 크레아티닌 수치가 신기능을 비교적 정확하게 반영할 수 있지만 노인 환자들에서는 혈청 크레아티닌 수치의 해석에 주의를 요한다. 약물을 투여하기 전 여러 가지 다른 방법을 이용해서 노인 환자들의 신기능을 정확하게 파악하는 것이 중요하다.
약물 투여 방법
노인 환자에서 정맥으로 약물을 투여하는 것은 경구투여에 비해 여러 가지 어려움이 있으므로 가급적 경구투여를 하는 것이 좋다. 노인 환자에서는 적절한 정맥 투여 혈관을 찾는데 어려움이 있으며 카테터 관련 감염이 흔하게 발생한다. 치매나 섬망이 있는 경우가 흔하여 정맥 주사를 유지하는 데에 어려움이 따르고, 정맥 주사가 거치되어 있는 경우 섬망 발생이 증가한다6). 항생제를 정맥으로 투여 시작한 경우라도 가능한 경우 조기에 경구 항생제로 변경하도록 한다. 경구 항생제를 투여하는 경우 용법과 용량을 잘 지키는지 여부와 약물 순응도를 확인할 필요가 있다.
약물 상호작용
노인 환자들은 여러 가지 기저 질환을 가지고 있는 경우가 흔하고 이로 인해 장기간 약물 치료를 받고 있는 경우가 흔하다7). 한 보고에 따르면 지역 사회의 노인 환자들 중 39%가 다섯 가지 이상의 약물을 투여받고 있었다8). 따라서 감염 질환에 대해 항생제 치료를 시행하는 경우 기존에 사용 중인 약제와의 상호작용을 염두에 두어야 한다. 약물 상호작용으로 인해 약물 부작용이 더욱 흔하게 발생할 수 있다.
약물 부작용
노인 환자에서 약물 부작용이 더욱 흔하게, 그리고 더욱 중증으로 발생하는 것으로 알려져 있으며 항생제가 중요하고 흔한 원인 약제이다9). 항생제는 구역, 구토 같은 위장 장애를 흔하게 유발하며, 항생제 관련 설사를 흔하게 일으킨다. 젊은 연령층 환자들에 비해 노인 환자에서 더 흔하게 발생하는 중요한 약물 부작용을 표 2에 기술하였다2,10).

Common antibiotic adverse drug reaction in elderly patients
노인 환자에서 약물 부작용이 더 흔하게 발생하는 이유로는 여러 가지 약물을 동시에 복용, 약물 상호 작용, 기저 질환의 존재, 약물 순응도 감소, 생리학적인 변화, 약력학/약동학적인 변화 등을 생각할 수 있다. 신기능을 부적절하게 예측하여 약물 용량 및 투여 간격이 적절하게 조정되지 못하는 경우도 흔하며, 이에 따라 부작용이 증가할 수 있다. 최근 개발된 신약의 경우, 임상 시험 대상에서 노인 연령층의 환자들이 제외되는 경우가 흔하므로 실제 진료 현장에서 사용되는 경우 노인 환자에서 예기치 못한 부작용이 발생하는 경우가 흔하다11). 결핵 치료의 경우 노인 환자에서 간독성이 발생하는 경우가 젊은 환자에 비해 더 흔하며12), 증가된 연령이 aminoglycoside 신독성 발생의 위험인자로 알려져 있다13). Aminoglycoside 이독성의 경우 비가역적이므로 노인 환자들에서 특히 문제가 될 수 있다14).
노인 환자에서 항생제 사용의 일반적인 원칙
노인 환자에서 항생제 부작용이 흔하게 그리고 심하게 발생할 수 있음을 염두에 두고 항생제 치료를 시작해야 할 때는 과연 항생제 치료가 반드시 필요한 상황인지를 다시 한번 고민해 보아야 하며, 치료를 시작한 경우에도 가능한 한 투여 기간을 최소화하려는 노력이 필요하다. 불필요한 항생제 투여는 부작용 발생을 증가시킴과 함께 항생제 내성균 발생을 촉진시킨다. 경험적으로 투여된 광범위 항생제는 원인균이 확인된 이후 적절하게 조절되어야 한다. 노인 환자에서 항생제 치료를 고려할 때는 연령 증가에 따른 생리적인 변화, 동반된 기저 질환, 면역 저하 상태로 인하여 항생제 치료 효과가 떨어질 수 있음을 인지해야 하고, 또한 적절한 투여 용량이 변할 수 있음을 고려해야 한다2,15). 경구 치료는 보다 편리하고 치료에 따른 비용과 독성을 줄일 수 있으므로 적극적으로 고려되어야 한다. Aminoglycoside, amphotericin B, vancomycin 등과 같은 좁은 치료 농도를 갖는 항생제는 가능한 피하는 것이 좋다.
결 론
환자 또는 항생제 관련 여러 인자들이 노인 환자에서의 항생제 치료에 영향을 줄 수 있다. 연령 증가에 따른 생리학적인 변화들로 인해 항생제의 약력학적인 인자들이 변함으로써 치료 효과가 감소되고 약물 부작용이 증가될 수 있다. 또한 노인 환자에서 적절한 항생제 투여 용량이 젊은 환자와 달라질 수 있다. 동반된 기저 질환으로 인해 다른 약물을 함께 투여받는 경우가 흔하므로 약물 상호작용에 주의하여야 한다. 하지만 아무리 주의를 기울인다고 하더라도 항생제 부작용은 발생할 수 있기 때문에 가장 중요한 것은 불필요한 항생제 투여가 이루어지지 않도록 하는 것이다. 점점 증가하고 있는 고령 인구를 고려해 볼 때, 노인 환자들을 진료하는 임상의들은 노인 환자들에서 발생하는 감염 질환의 독특한 측면과 항생제 사용의 일반적인 원칙에 익숙해지는 것이 필요하겠다.