복막투석에서 장기 기술 생존: 단일 임상기관 연구
Technique survival in peritoneal dialysis: A single-center experience
Article information
Abstract
목적:
지난 20년간 복막투석용 도관의 연결시스템이 발달함에 따라 기술 생존율이 향상을 보인다는 국내외 여러 기관의 보고가 있었다. 이에 대해 본 저자들은 복막 기술 생존율과 기술 실패의 원인을 분석하고자 하였다.
방법:
1994년 이후 본원에서 복막투석을 시행한 환자들의 자료를 후향적으로 수집하였다. 복막투석 시작 당시 15세 미만이거나, 관찰 기간이 1개월 미만인 경우, 그리고 기록이 잘 보존되지 않은 환자의 경우는 제외하였다. 총 608명의 환자를 대상으로 복막투석의 기술 생존율과 탈락의 원인을 분석하였다.
결과:
608명 중 남자가 342명(56.3%), 여자가 266명(43.7%)이었다. 생존 분석은 Kaplan-Meier 방법과 log-rank test를 이용하여 분석하였다. 복막투석 시작 당시의 평균연령은 50.7±15.1세였고, 평균 복막투석 지속기간은 50.2±41.5개월이었다. 만성신부전의 원인 질환으로는 당뇨병이 241명(39.6%)으로 가장 많았고, 만성 사구체 신염이 226명(37.2%), 고혈압이 79명(13.0%)이었다. 기술 생존율은 각각 1년째 97.3%, 3년째 91.7%, 5년째 82.3%, 10년째가 67.5%였다. 당뇨병 유무는 기술 생존율에 영향을 미치지 않았다(p=0.26). 60세 이전에 투석을 시작한 군에서 60세 이후에 투석을 시작한 군보다 기술 생존율이 높았다(p=0.005). 복막 투석 중단의 원인 중 기술적 원인으로는 복막염이 68명(71.6%)으로 가장 많았고, 도관 기능 부전이 10명(10.5%), 한외여과 실패 7명(7.4%) 및 부적절한 투석이 6명(6.3%), 도관 감염이 4명(4.2%)이었다.
결론:
복막염은 여전히 복막투석 중단의 가장 큰 원인이었으며, 복막투석의 기술 생존율을 높이기 위해서는 복막염을 최소화하는 것이 중요한 것 같다.
Trans Abstract
Background/Aims:
Continuous ambulatory peritoneal dialysis (CAPD) is an established treatment in patients with end-stagerenal disease (ESRD), and innovations in the connection system have improved the survival of peritoneal dialysis patients over thelast two decades. We investigated the outcome of CAPD over a 15-year period at our institution.
Methods:
Patients who underwent peritoneal dialysis since 1994 were recruited retrospectively. Patients younger than 15 years atthe initiation of CAPD and those who had less than 1 month of follow-up or missing data were excluded. The technique survivalrate and causes of technique failure were evaluated.
Results:
In all, 608 CAPD patients (342 males, 56.3%) were analyzed using the Kaplan-Meier method and log-rank test. Themean age at the start of CAPD was 50.7±15.1 years and the mean duration of CAPD was 50.2±41.5 months. The most commonprimary renal disease was diabetes (39.6%), followed by chronic glomerulonephritis (37.2%) and hypertension (13.0%). The 1-, 3-,5-, and 10-year death-censored technique survival rates were 97.3, 91.7, 82.8, and 67.5%, respectively. Sex or diabetic status did notaffect the technique survival rate. Patients younger than 60 years at the start of CAPD had a better technique survival than olderpatients (p=0.005). The main cause of technique failure was peritonitis (71.6%), followed by mechanical malfunction (10.5%),ultrafiltration failure (7.4%), and inadequate dialysis (6.3%).
Conclusions:
Complicating peritonitis was the most common cause of CAPD technique failure at our center. To reduce thetechnique failure in high-risk groups, more intensive management is needed. (Korean J Med 79:258-262, 2010)
서 론
1980년대 초 국내에 복막투석이 도입된 이후 복막투석 환자 및 복막투석을 시행하는 의료기관의 수는 점점 증가하고 있다. 2008년 대한신장학회 말기신부전 환자 등록사업 보고에 의하면 국내에서 신대체 요법을 시행 받은 환자는 51,989명에 달하며 그 중 혈액투석 환자의 수가 33,427명, 복막투석 환자 수가 7,840명으로 신대체 요법에서 복막투석이 차지하는 비율은 해마다 증가하다 2007년 이후 처음으로 다소 감소하는 양상을 보였다1). 환자 군의 고령화로 당뇨 유병률 및 심혈관계 합병증이 증가했음에도 불구하고1), 지난 20년간 복막투석의 5년 기술 생존율은 10~20% 향상을 보이고 있다2-5). 이는 Y-set 및 twin bag 시스템의 도입 등 복막투석용도관의 연결시스템이 발달하면서 복막염의 빈도가 감소한 것이 가장 큰 원인이라고 생각된다6). 전 세계적으로 기술 생존율이 증가하는 추세이지만, 그 정도는 각 기관마다 차이를 보인다. 이에 저자들은 본원에서의 복막투석 기술 생존율과 복막투석 중단 원인에 대해 분석하고자 하였다.
대상 및 방법
1994년 1월부터 2009년 6월까지 경북대학교 병원에서 복막투석을 시행한 836명 환자들을 대상으로 후향적 연구를 진행하였다. 복막투석 시작 당시 15세 미만이거나, 관찰 기간이 1개월 미만인 경우, 그리고 기록이 잘 보존되지 않은 환자의 경우는 제외하여 총 608명의 환자들을 분석하였다. 각 환자의 나이나 성별, 원인 신질환, 당뇨병 동반유무, 복막투석의 시작시점과 중단시점, 중단 시의 원인에 대한 자료를 수집하였고, 2000년 이후의 경우에는 전산 관리된 Multicenter Clinical Data (MCD, Copyright © 2000-2009 MEDINTEL Co., Ltd.)의 자료를 활용하였다. MCD는 복막투석 시작 당시 투석 환자의 자료를 생성하고 환자가 외래를 방문할 경우 기록을 입력하여 관리하는 웹 기반 데이터베이스 관리시스템이다. 기술 및 환자 생존율과 관련된 자료는 매월 말 복막투석 간호사에 의하여 원인에 관한 통계자료를 작성하였고, 담당 의사에 의하여 검토되었다. 수술 당일 예방적 항생제로 세파졸린 1 g이 투여되었고, 복막 투석용 도관삽입은 외과의에 의해 이루어졌다. 신이식을 시행했거나, 타 기관으로의 전원, 복막염 및 복막투석과 연관되지 않은 사망 및 추적 탈락된 경우는 기술 생존분석에서 중도절단(censoring)으로 처리를 하였다. 기술 생존율 분석에 있어서는 복막염, 한외여과 실패(UF failure), 부적절한 투석(inadequate dialysis), 도관 및 출구감염, 도관폐쇄에 의한 경우를 실패의 원인으로 분류하였다. 생존율은 Kaplan-Meier 방법을 통하여 분석하였고, 각 변수별 생존율의 차이를 분석하기 위해서 log-rank test를 이용하였다. 모든 자료는 p 값이 0.05 미만일 때 유의하다고 판정하였다.
결 과
1. 환자 특성
총 608명의 환자가 분석되었고, 남자가 342명(56.3%), 여자가 266명(43.7%)이었다. 복막투석을 시작할 당시 대상 환자의 평균연령은 50.7±15.1세였고, 15~30세가 71명(11.7%), 31~45세가 149명(24.5%), 46~60세가 203명(33.4%), 60세 이상인 환자가 185명(30.4%)이었다. 복막투석지속 평균 기간은 50.2±41.5개월이었다. 만성신부전의 원인 질환으로는 당뇨병이 241명(39.6%)으로 가장 많았고, 만성 사구체신염이 226명(37.2%), 고혈압이 79명(13.0%)이었다(표 1). 2000년 이후부터 twin-bag 시스템이 도입되었다.
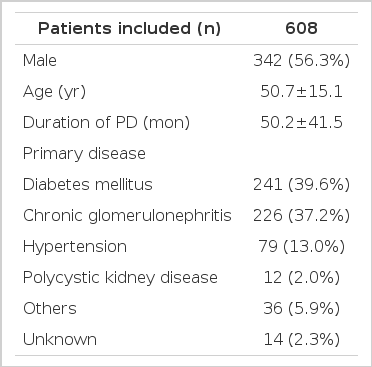
Patient characteristics
2. 복막 투석의 중단 원인
복막 투석의 중단 원인으로는 심장질환이나 뇌혈관질환, 암, 복막염을 제외한 감염 등 복막투석과 관련되지 않은 사망이 229명(51.9%)으로 가장 많았고, 신이식이 69명(15.6%), 복막염이 68명(15.4%), 도관 기능부전이 10명(2.3%), 한외여과 실패가 7명(1.6%), 부적절한 투석이 6명(1.4%), 도관 감염이 4명(0.9%)이었다. 그 외 기타 원인으로는 타원으로의 전원 혹은 추적탈락, 신기능이 회복되어 투석을 중단했거나, 환자의 선호도에 따라 혈액투석으로 전환한 경우 등이 있었다(표 2). 복막염에 의한 패혈증으로 사망했을 시는 중단 원인 분석 시 복막염으로 포함하여 분석하였다. 기술 생존율은 각각 1년째 97.3%, 3년째 91.7%, 5년째 82.3%, 10년째 67.5%였다(그림 1). 각 변수별 차이에 의한 생존율을 분석한 결과, 당뇨병의 유무는 기술 생존율에 차이가 없었다(p=0.26, 그림 2). 60세 이전에 복막투석을 시작한 환자군에서 60세 이후에 시작한 환자군에 비해 더 높은 기술 생존율을 보였다(p=0.005, 그림 3). 성별 역시 기술 생존율에 유의한 영향을 끼치지는 않았다. 기술 실패의 원인을 빈도별로 분석하면, 복막염이 68명(71.6%)으로 가장 많았고, 한외여과 실패 및 부적절한 투석이 13명(13.7%), 도관 기능부전이 10명(10.5%), 도관 감염이 4명(4.2%)을 차지했다(표 3).
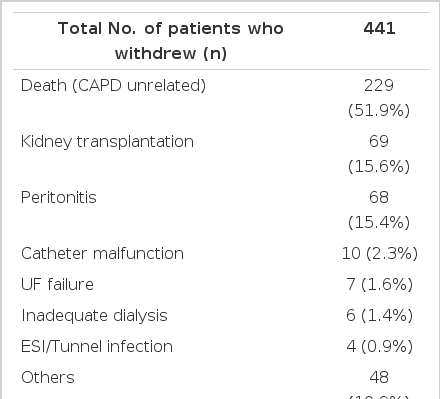
Cause of withdrawl from peritoneal dialysis
Kaplan-Meier technique survival curves. The 1-, 3-, 5-, and 10-year death-censored technique survival rates were 97.3, 91.7, 82.3, and 67.5%, respectively.
Kaplan-Meier technique survival curves of the diabetic and nondiabetic groups. No significant difference in technique failure was observed between the two groups (p=.267).
Kaplan-Meier technique survival curves according to age at the start of peritoneal dialysis. Patients younger than 60 years at the start of CAPD had better technique survival rates than older patients (p=0.005).
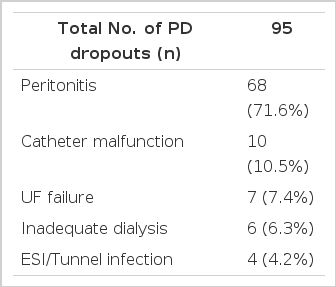
Cause of technique failure
고 찰
Troidle 등7)의 연구에 의하면 신장실을 운영하는 임상의에게 있어 복막투석의 기술적 생존율이 복막투석을 선택하는데 있어 가장 큰 장애물 혹은 관심사라는 보고도 있다. 하지만 국내외 여러 기관의 보고에 따르면 최근 20년간 복막투석과 관련되지 않은 사망을 제외한 5년 기술 생존율(death censored)은 10~20% 증가를 보이고 있다. 시간의 변화에 따른 기술 생존율의 향상은 몇몇 대규모 코호트 연구에서도 나타난다2-5). 2008년 1,600명 이상을 분석한 연세대학교 병원의 보고에 따르면, 1981~1992년의 기술 생존율이 64.4%인데 비해 1993~2005년은 74.7%로 증가하였다2). USRDS에서도 유사한 경향이 보고되었는데, 1996~1998년에 비해 1999~2001, 2002~2004년의 기술 실패율의 위험(hazard ratio)이 각각 0.9, 0.62로 감소하였다3). 네덜란드의 RENINE 연구에서도 1994~1996년에 복막투석을 시작한 환자에 비해 1997~1999년에 시작한 환자들에서 더 우수한 기술 생존율을 보였으며, 위험비율도 약 0.82로 감소하였다4). 그 외 캐나다의 연구에서도 1981~1989년에 비해 1997~1999년에 시작한 환자들의 위험비율이 약 0.8이었다5). 이와 같은 기술 생존율의 향상에는 복막투석에서의 감염의 감소가 기여한 바가 크다고 생각 된다. 종래의 spike 시스템과 비교한 Y-set 및 twin-bag 시스템의 복막염 위험률에 대한 무작위 대조군 연구에서 Y-set 및 twin-bag을 도입하면서 복막염의 빈도가 감소 하였다6). 비용(nasal) 항생제 연고를 사용하게 되면서 출구 감염 및 터널감염의 빈도가 감소한 것과도 연관이 있다 할 수 있다8,9). 비용 뮤피로신 연고를 사용함으로써 출구 감염의 위험 비율이 0.58로 감소하였다는 보고도 있다9). 본원 분석 결과에서 복막염은 여전히 복막투석 중단의 기술적 원인 중 가장 큰 부분을 차지하고 있었다. 복막투석 중단의 원인은 각 기관마다 차이가 있다. CANUSA, CHOICE 등 전향적 연구에 따르면 복막투석의 중단 원인 중 복막염이 30~36%이며, 부적절한 투석, 한외여과 실패가 그 뒤를 따르고 있다10-12,14,15). 국내의 보고에서도 복막염에 의한 원인은 감소를 보이고 있지만, 현재까지 복막염이 가장 큰 비중을 차지하는 것은 마찬가지이다2,13). 당뇨병은 복막투석의 생존율에 중요한 영향을 끼친다. 여러 보고에서 당뇨병이 있는 군에서 기술 생존 실패의 위험이 높다고 하였다2,10,11). USRDS 등의 보고에 따르면 여자에서 복막염의 위험률이 낮고 기술 생존율도 성별에 따라서 차이를 보인다3,16). 하지만 본원 분석 결과 당뇨병의 유무는 기술 생존율에 유의한 영향을 끼치지 못했으며, 여자에서 기술 생존율이 더 나은 경향을 보였으나 통계적 유의성은 없었다. 서구인에 비해 아시아인에서 기술적 실패의 위험이 낮다는 보고도 있다3,17). 그 외에도 기술 생존율에 영향을 끼치는 요소로는 임상기관의 규모3-5,18), 비만14,19), 복막투석 시작 당시의 잔여 신기능 등이 있다20,21). 생체적합성 투석액의 사용과 기술 생존율의 관계에 대한 2건의 국내 보고에서는 복막투석액의 생체적합성 향상과 함께 기술 생존율이 향상된다는 증거는 없었다22).
요약하면 복막투석의 기술 탈락의 가장 큰 원인은 복막염이었으며 기술 생존율에 있어서는 국내외 기관의 기존 보고와 유사하거나 다소 높은 경향을 보였다. 당뇨병의 유무 및 성별에 따른 기술 생존율의 차이는 없었으나 복막투석 시작 시점의 나이가 젊은 경우 기술 생존율이 좋았다. 이러한 점을 고려하여 복막투석의 기술 생존율을 높이기 위해서는 복막염의 위험을 최소화하는 것이 중요하다 하겠다.