중증 천식과 기침
Cough in Severe Asthma
Article information
Trans Abstract
Asthma is a heterogeneous clinical syndrome that presents with variable symptoms, including cough, breathlessness, chest discomfort, and wheezing. Cough, a primary symptom of asthma, has distinct regulatory mechanisms and was associated with asthma severity, poor asthma control, diminished quality of life, and an increased risk of frequent future exacerbations. However, current tools for measuring asthma control do not include separate items for cough or other specific symptoms, and the true impact and clinical relevance of cough in asthma remains poorly understood. Consequently, current stepwise treatment algorithms based on asthma control may be overly simplistic and might not adequately address the heterogeneity of asthma or the mechanisms underlying its symptoms. Furthermore, this approach carries the risk of overestimating asthma severity and subsequent overtreatment. The concept of treatable traits is fundamental to precision medicine, wherein each symptom, especially cough, may serve as a treatable trait in its own right. In this paper, we aim to present evidence supporting the concept of cough as a treatable trait in asthma, addressing its three major components, which are clinical relevance, measurability, and treatability.
서 론
천식이 다양한 표현형으로 나타날 수 있는 만성 기도 질환임을 인식하는 것은 2000년대에 제안되었고, 현재는 이러한 견해가 널리 인정받고 있다[1,2]. 대표적인 표현형 지표 중 하나는 발병 연령으로, 소아기에 발생하는 천식과 성인기에 발생하는 천식은 유전적 요인, 환경, 동반 질환 등이 연관된 정도가 서로 다르다[3]. 기도의 가역적 폐쇄는 개념적으로 천식의 공통된 병리학적 특성으로 간주되지만 실제로 일부 환자에서는 관찰되지 않기도 하며, 흡연력, 천식의 악화, 질병의 지속 기간 등에 따라 달라질 수 있다[4]. 한편 전통적인 관념과는 달리 아토피 없이 호산구 기도 염증이 존재하는 천식은 성인기에 흔하며, 일부 환자에서는 주요 증상으로 호중구 염증이 나타나기도 한다[5,6]. 이러한 점들 때문에 천식의 진단명이 주는 정보는 제한적이라고 볼 수 있다[7].
중증 천식은 일반적으로 고용량의 흡입 스테로이드 및 기관지확장제 등 표준 치료에도 증상이 지속되고 급성 악화가 반복되는 상황으로 정의된다[8]. 천식 표현형의 차이는 중증 천식 환자의 치료 계획과 결과에 더욱 중요한 영향을 미친다[1,2]. 이에 따라 최근에는 치료에 실제적인 영향을 줄 수 있는 치료 가능한 형질(treatable traits)을 찾고 검증하는 시도가 진행되고 있다. 치료 가능한 형질은 표현형 지표 중에서 임상적 연관성(clinical relevance), 측정 가능성(measurability), 치료 가능성(treatability)의 세 가지 조건을 충족하는 지표를 의미한다[7].
Global Initiative for Asthma (GINA) 가이드라인 서두에 “asthma is defined by the history of respiratory symptoms, such as wheeze, shortness of breath, chest tightness, and cough…”라고 기술되어 있듯이[9] 증상은 천식을 정의하는 주요 요소이다. 증상은 의사가 천식을 의심하는 중요한 첫 단서가 되며, 환자의 질병 경험, 삶의 질, 질병 부담 등에도 직접적인 영향을 미친다. 많은 천식 환자에서 이러한 증상들은 서로 연관되어 있으며, 일반적으로 함께 악화되고 치료제에 대한 반응도 함께 나타나는 경향이 있다. 따라서 이러한 증상들은 구분되지 않고 하나의 그룹으로 다루어져 왔다. Asthma control test나 asthma control questionnaire (ACQ)와 같이 흔히 사용되는 천식 조절도 측정 도구에서도 여러 증상들은 ‘증상’이라는 하나의 카테고리로 묶여 있다[10,11]. 그러나 최근의 기전 연구와 중개 연구를 통해 각 증상이 고유한 병태생리학적 특성을 가지고 있음이 밝혀지고 있고, 임상 연구를 통해 개별 증상과 type 2 (T2) 기도 염증, 기도 폐색 등 천식 지표 사이의 관련성과 독립성에 대해 알려지기 시작하였다[12-14].
증상을 구분하는 접근법은 향후 맞춤형 치료로 나아가는 데 있어 중요한 역할을 할 것으로 예상된다. 현재 GINA 가이드라인 등에서 제시하는 단계적 치료(stepwise treatment) 알고리즘에서 증상은 천식 조절도 평가의 중요한 지표 중 하나이다. 하지만 현재 가이드라인은 지난 10년 동안 규명되어 온 병태생리학적 다양성을 충분히 반영하고 있지 않다[9]. 특히 증상을 구별하지 않음으로써 과도한 치료로 이어질 위험이 있다. 이러한 가이드라인을 개선하기 위해서는 임상 근거를 마련하는 연구들이 적절히 수행되어야 한다. 본 논문에서는 이러한 배경을 바탕으로 천식 환자에서 치료 가능한 형질로서 기침에 대한 연구 결과와 흐름을 소개하고자 한다.
본 론
기침과 천식의 임상적 연관성
기침은 천식 환자에서 흔하고 중요한 증상이다. 천식 환자 가운데 만성 기침 유병률은 지역과 연구에 따라 다양하게 보고되어 있다. 덴마크 코펜하겐 지역사회 연구에서는 비율이 8%였으며, 호주의 Severe Asthma Network 환자 레지스트리 연구에서는 39%로 보고되었다[15,16]. 또한, 한국인 중증 천식 레지스트리(Korean severe asthma registry)에서는 이 비율이 약 15% 정도로 나타났다(unpublished data). 또한 천식은 만성 기침의 흔한 원인 또는 동반 질환이기도 하다[17].
천식 중증도가 증가함에 따라 기침의 양상과 정도에도 차이가 나타난다. 기침의 빈도와 정도는 천식 중증도와 연관되어 있다. 스웨덴의 지역사회 연구에 따르면, 조절이 제대로 되지 않는 천식 환자일수록 기침과 객담 유병률이 높았다[18]. 또한 환자군 연구에서도 천식의 중증도가 기침의 횟수 및 정도와 유의한 상관관계를 가지고 있음이 확인되었다[19,20]. 특히 중증 천식 환자들은 기침을 상대적으로 더 힘든 증상으로 여기며, 급성 악화 시에 기침과 호흡곤란을 가장 괴로운 증상으로 인식하는 것으로 나타났다[21,22].
기침의 정도는 천식 예후와도 밀접한 관련이 있다. 천식 진단 시 지속적인 기침 및 객담의 유무는 향후 천식의 중증도와 연관되어 있다. 만성 기침을 동반한 천식 환자들은 그렇지 않은 환자들보다 낮은 폐기능을 보이며, 더 높은 빈도의 천식 관련 병원 이용 및 급성 악화를 경험하는 경향이 있다[15,18,23]. 또한 기침 관련 삶의 질은 천식 조절도 및 천식 관련 삶의 질과 통계적으로 유의한 상관관계를 보였다[16,19]. 그러나 주목할 점은 기침의 정도와 폐기능, T2 염증 정도 사이에는 상관성이 낮다는 것이다[19]. 이는 기침의 병태생리가 독립적일 가능성을 시사한다.
기침 측정법
기침은 기침 조절 신경 회로에 의해 유발되는 폭발적인 반사 작용으로 정의된다. 이는 빠르고 강한 날숨과 닫힌 성문(glottis) 사이에서 발생하는 특징적인 소리로 나타난다. 이러한 소리의 특성을 기반으로 기침 횟수를 측정할 수 있다. 그러나 기침의 평가는 횟수뿐만 아니라 중등도(severity), 강도(intensity), 동반 증상, 삶의 질에 미치는 영향 등 여러 영역에서 이루어질 수 있다. 이러한 다양한 영역들은 서로 연관되어 있지만 독립적인 관계 특성을 갖고 있다[24]. 표준 천식 치료에 반응하지 않는 기침의 경우 기침반사 과민성(cough reflex hypersensitivity)이 중요한 역할을 할 가능성이 있으므로 이를 평가하는 것도 필요할 수 있다.
간단하면서도 진료실에서 활용 가능한 방법은 환자에게 기침의 중증도에 대해 묻는 것이다. 기침은 불편한 증상이지만, 동시에 몸을 보호하는 반사 작용이기도 하다. 따라서 환자가 느끼는 중증도는 임상적으로 중요한 의미를 가진다. 시각 아날로그 척도(visual analogue scale, VAS), 점수 척도 등은 사용이 간편하다는 장점이 있지만, 개인별 점수 편차가 큰 편이다. 이에 비해 patient global impression of severity와 같이 의미가 부여된 Likert 척도를 사용하는 도구는 직관성이 높아 최근 대안으로 제시되고 있다[25]. Leicester cough questionnaire와 같은 기침 관련 삶의 질 설문은 기침이 신체적, 정신적, 사회적으로 미치는 영향을 평가하는 검증된 도구로, 한국을 포함한 여러 국가에서 널리 사용되고 있다[26]. 그러나 설문 항목이 많은 편이기 때문에 임상 연구에 더욱 적합한 편이다.
기침 횟수는 객관적으로 측정이 가능하며, 임상 시험에서 중요한 결과 지표로 간주된다. 기침 횟수 측정법은 주관적인 설문 대비 환자의 신체적, 정신적 상태의 영향이 적고 개인별 편차도 적은 장점이 있다. 하지만 이러한 도구는 현재까지 사용이 다소 번거롭고 복잡하여 주로 연구 목적으로 활용 되고 있다. VitaloJak과 Leicester cough monitor는 대표적인 기침 횟수 측정 도구로, 이들은 천식 환자의 ACQ 점수 및 GINA 천식 조절도와 유의한 상관관계를 보인다[19]. 기침 횟수 측정 도구와 방법이 지속적으로 발전함에 따라 실제 진료에서의 활용도 역시 증가할 것으로 예상된다[27,28].
기침반사 과민성은 capsaicin, citric acid, 고장성 식염수 등 기침 유발 자극 물질을 흡입하며 측정할 수 있다. 천식 환자에서는 건강인에 비해 citric acid 기침반사가 증가해 있으며, capsaicin으로 측정한 기침반사는 특히 아토피가 없는 여성 천식 환자에서 민감한 것으로 알려져 있다[29,30]. 기침반사 정도는 천식의 중증도 및 ACQ 점수와 높은 상관관계를 보이며, 중증 천식 환자에서 기침반사가 증가해 있다는 연구 결과가 있다[31,32]. 중증 천식 환자 기도 상피에는 capsaicin 수용체인 transient receptor potential vanilloid 1 발현이 증가되어 있다는 연구도 있다[33]. 하지만 기침반사 측정 검사의 임상 진료에서의 용도와 유용성은 아직 확립되지 않았으며, 주로 기전 연구에 활용되고 있다.
기침은 목의 가려움, 따가움, 자극감, 이물감 등과 같은 비정상적인 감각이 선행하거나 동반되는 경우가 흔하다. 이러한 후두(목)의 비정상적인 감각이나 과민성은 기침과 관련된 삶의 질과 연관이 있다[34]. 자주 함께 나타나는 문제 중 하나는 후두기능 이상(laryngeal dysfunction)인데, 이는 주로 흡기 시 성문이나 성문상부(supraglottis)가 비정상적으로 좁아지거나 수축하는 현상으로 정의된다. 천식 환자 중 약 25%에서 이러한 문제가 나타나며, 특히 중증 천식 환자에서는 비율이 더 높은 것으로 추정된다[35,36]. 후두의 이러한 증상과 문제는 기침뿐만 아니라 호흡곤란, 천명 등 다른 증상으로 나타날 수 있기 때문에 이를 적절하게 평가하는 것은 감별 진단과 중증도 평가에 도움이 된다. 평가를 위해 설문지와 유발 후두 내시경 검사 등을 활용할 수 있다[37].
천식 환자에서의 기침 조절
천식 환자 다수에서 기침은 호흡곤란, 천명과 함께 나타난다. T2 염증과 기관지 수축이 기침반사 과민성을 촉진할 수 있기 때문에[38,39] T2 염증과 기관지 수축을 정상화시키는 약제가 기침 조절에 효과적일 수 있다. 그러나 T2 염증이나 기도 폐쇄가 잘 조절되고 있는 상황에서 기침이 심한 경우에는 다른 요인을 고려해야 한다. 알레르기 비염, 위식도 역류 질환 등 동반 질환이 천식 환자에서 빈번한 것은 사실이지만, 실제로 이들 동반 질환의 치료가 기침 자체에 미치는 영향은 크지 않을 수 있다[40,41].
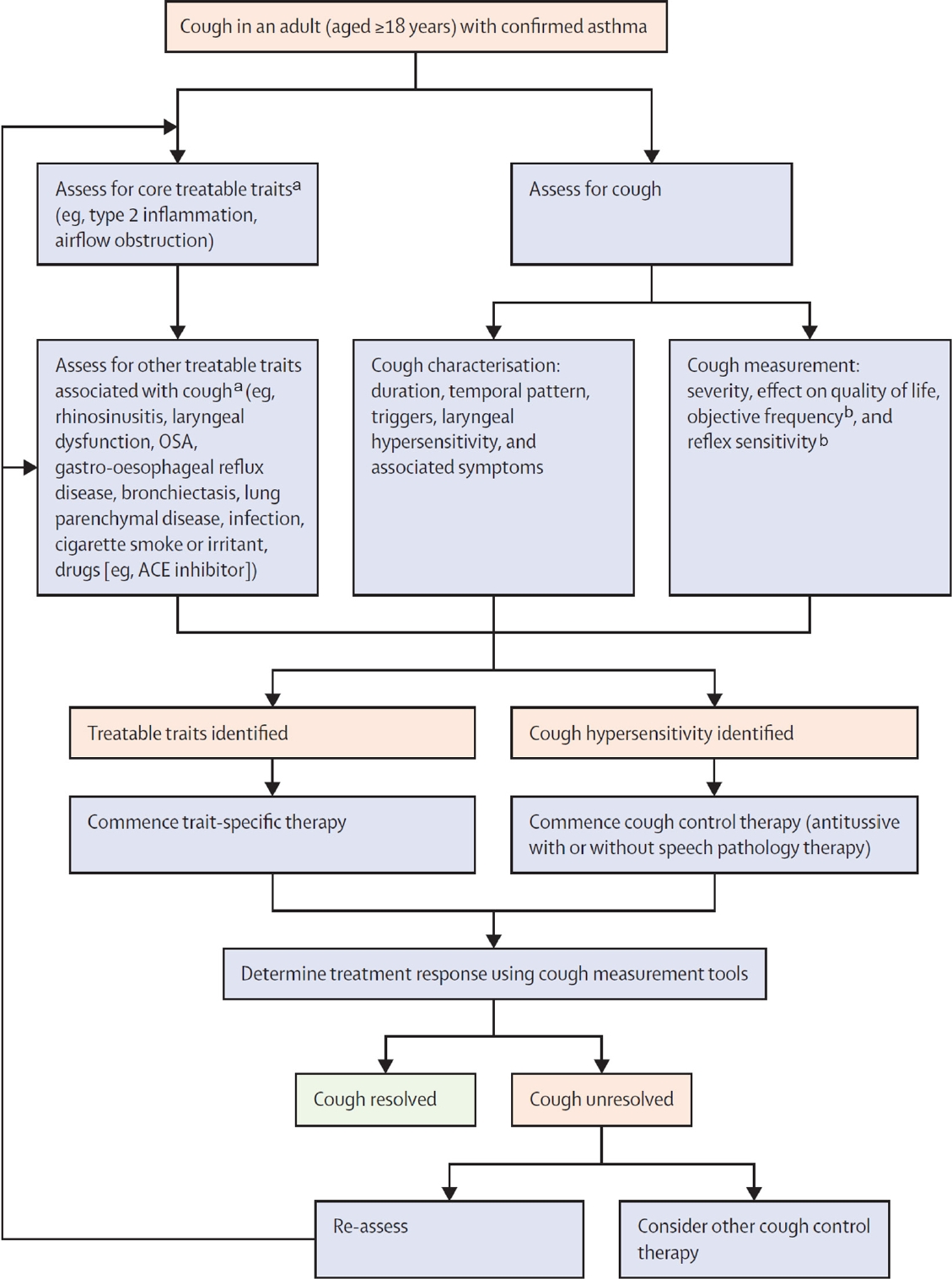
한편, 중증 호산구 천식 환자에서 항interleukin (IL)-5 단클론항체의 기침 조절 효과에 대해서는 연구 결과들이 일관적이지 않다. 이는 중증 천식의 기침 기전이 환자마다 다를 수 있다는 것을 시사한다. 예를 들어, 전향적 임상시험에서는 mepolizumab이 경구 스테로이드와는 달리 기침 VAS 점수 개선에 효과가 없었지만[12,42], 다른 후향적 연구에서는 항IL-5 단클론항체 사용 후 기침 관련 삶의 질과 capsaicin 기침 과민성이 유의하게 개선되었다는 보고가 있다[43]. 한 코호트 연구에 따르면 중증 천식 환자에서는 capsaicin 기침 과민성이 증가하고, 기침 과민성은 천식 악화, 조절도, 입원 등과 연관성을 보였다[44]. 이러한 관점에서 T2 염증과 기도 폐쇄, 동반 질환 등 치료에도 기침 조절이 되지 않는 중증 천식 환자에서는 기침반사 과민성에 대한 치료를 고려할 필요가 있다. 이를 판단하기 위해서는 기침 중증도, 지속 기간, 시간 양상, 후두 과민성 및 동반된 증상 등 기침의 특성에 대한 자세한 평가가 필요하다(Fig. 1) [17].
기침 반사 과민성에 대한 대표적인 치료로는 난치성 만성 기침에 사용되는 신경 조절 약물(neuromodulatory drug)과 비약물적 치료인 음성 병리 치료(speech pathology therapy)가 있다[17,45,46]. 비약물적 치료는 아직 국내에는 도입되지 않았으나 부작용이 없어 천식 환자에게도 적용할 수 있을 것으로 생각된다. 최근 난치성 만성 기침 치료를 위해 개발된 신약인 P2X3수용체길항제는 말초 신경 세포에 존재하는 adenosine triphosphate (ATP)수용체인 P2X3를 조절한다[47]. ATP는 알라민(alarmin)의 한 종류로, 흡입 시 천식 환자의 기도 수축을 유발할 수 있다[48,49]. 실험 연구에서 알레르겐에 노출된 천식 환자와 동물 모델의 기도에서 ATP가 증가하고, 퓨린수용체길항제 투여가 기도 저항 및 호산구성 기도 염증을 개선할 가능성이 제시된 바 있다[50]. 이런 점에서 기침이 조절되지 않는 중증 천식 환자에서 향후 P2X3수용체길항제를 포함한 신경회로 작용 약물들이 시도될 가능성이 있다.
결 론
천식 환자에서 기침은 임상적으로 중요할 뿐만 아니라, 측정 및 치료가 가능한 형질이다(Fig. 2). 기침은 천식의 중증도, 조절 상태, 삶의 질, 그리고 미래의 악화 위험성과 관련이 있다. 그러나 대다수의 기존 천식 임상 연구에서는 기침을 적절히 측정하거나 평가하지 않았기 때문에[51] 천식 치료제들의 기침 조절 효과는 아직 잘 알려져 있지 않다. 기침에 대한 자세한 평가 도구를 사용한다면 기침의 치료 가능한 형질을 평가하고 치료하는 데 도움이 될 수 있겠다. 최근 다양한 방법으로 기침을 측정할 수 있으며, 기침의 신경 과민성을 조절할 수 있는 새로운 약물들이 개발 중이다. 이러한 새로운 접근 방법은 향후 중증 천식 치료를 개인 맞춤형으로 발전시키는 데 기여할 수 있을 것으로 기대된다.
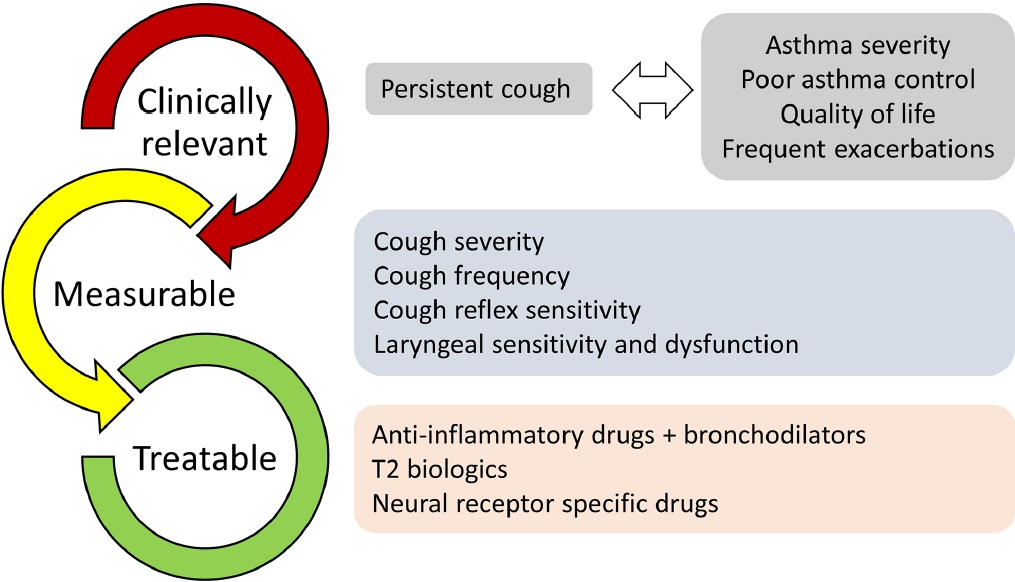
Cough as a treatable trait in asthma: a summary of current findings. T2, type 2.
Notes
CONFLICTS OF INTEREST
WJS declares grants from Merck Sharp & Dohme Corp. and AstraZeneca, consulting fees from Merck, Bellus, AstraZeneca, Shionogi, and GSK, and lecture fees from Merck, AstraZeneca, GSK, Sanofi, and Novartis. Other authors have nothing to declare.
FUNDING
None.
AUTHOR CONTRIBUTIONS
HY Lee and WJ Song developed the concept of the manuscript. HY Lee, YJ Lee and WJ Song drafted the manuscript. All authors approved the final version of the manuscript.
Acknowledgements
None.