발적성 위염의 중증도를 기반으로 한 헬리코박터 파일로리 감염 예측
Prediction of Helicobacter pylori Infection by Endoscopic Severity of Erythematous Gastritis in Asymptomatic Adults
Article information
Abstract
목적
Helicobacter pylori (H. pylori) 감염은 시드니 분류 시스템의 내시경적 소견 중 하나인 발적성 위염과 연관성을 가지고 있다고 알려져 있다. 본 연구는 발적성 위염의 내시경적 중증도에 따른 H. pylori 감염률을 평가하고자 하였다.
방법
이 연구는 전향적 연구로 검진 목적의 위 내시경으로 발적성 위염을 진단받은 무증상의 성인을 대상으로 하였다. H. pylori 감염을 진단하기 위해 급속 요소분해효소 검사가 시행되었다. 발적성 위염의 중증도는 시드니 분류 체계를 사용하여 내시경 소견을 평가하였다. 연구의 일차 결과 지표는 경도 또는 중등도 발적성 위염을 중증 발적성 위염과 비교하여 H. pylori 감염률이 차이가 있는지로 하였다.
결과
총 131명의 환자가 포함되었다. 발적성 위염 환자 전체에서 H. pylori 감염률은 45.8%였다. 131명의 환자 중 45명은 경도, 43명은 중등도, 43명은 중증이었다. H. pylori 감염률은 경도-중등도와 중증 발적성 위염 간에 유의하게 차이를 보였다(20.5% vs. 97.7%, p = 0.000). 혼란 변수를 보정한 뒤에도, 발적성 위염의 중증도는 H. pylori 감염률과 연관이 있었다. 카파 계수는 0.563, 관찰자 간 차이는 14.43%였다.
결론
H. pylori 감염은 발적성 위염에서 중등도로 관찰되었다. 그리고 발적성 위염의 중증도에 따라 H. pylori 감염률이 차이가 있었다.
Trans Abstract
Background/Aims
Helicobacter pylori (H. pylori) infection is correlated with erythematous gastritis, which is one of the endoscopic findings of the Sydney classification system. The present study evaluated the association between the endoscopic severity of erythematous gastritis and H. pylori infection.
Methods
We prospectively enrolled asymptomatic adults who were diagnosed with erythematous gastritis during screening esophagogastroduodenoscopy. A rapid urease test was performed in all participants to diagnose H. pylori infection. The severity of erythematous gastritis was determined based on the Sydney classification system. The primary endpoint was the H. pylori infection rate according to the severity of erythematous gastritis (mild to moderate vs. severe).
Results
In total, 131 patients with erythematous gastritis were included. The rate of H. pylori infection was 45.8% across all patients. Of the 131 included patients, 45 had mild gastritis, 43 had moderate gastritis, and 43 had severe gastritis. The H. pylori infection rate was significantly different between patients with mild to moderate erythematous gastritis and those with severe erythematous gastritis (20.5% vs. 97.7%, respectively; p = 0.000). After adjustment for potential confounding variables, the severity of erythematous gastritis was associated with the H. pylori infection rate. The kappa value was 0.563, and interobserver variation was 14.43%.
Conclusions
H. pylori infection is observed to a moderate degree in patients with erythematous gastritis. The severity of erythematous gastritis is associated with the H. pylori infection rate.
서 론
헬리코박터 파일로리(Helicobacter pylori)는 만성 위염, 위궤양과 위암의 주요한 원인 인자로, 인간의 위 점막에서 상부위장관 내시경 조직 검사로 검출이 가능하다고 규명되었다[1,2]. 따라서 헬리코박터 파일로리에 대한 제균 치료는 헬리코박터 양성 위궤양 환자에서 재발률을 낮추고[3], 일반 인구 집단에서 위암을 예방하는 데 효과가 있음이 밝혀졌다. 한 메타 분석에 의하면 건강하고 무증상인 인구 집단에서 헬리코박터 제균을 하지 않은 군에 비해 제균한 군에서 위암을 약 50% 예방하는 것이 가능하다고 보고되었다[4]. 우리나라 성인의 헬리코박터 파일로리의 혈청학적 양성률은 1998년에 66.9%, 2005년에 59.6%, 2011년에 54.5%로 감소 추세이지만 여전히 높은 수준으로, 헬리코박터 파일로리 감염을 적극적으로 진단하고 치료할 필요가 있다[2,5-7].
위염의 분류는 1939년 루돌프 쉰들러가 제안한 분류 체계가 기본적으로 사용되고 있다. 그는 만성 표층성 위염(chronic superficial gastritis)을 수개월 또는 수년 동안 지속된 위염이라고 정의하였고, 위염이 더욱 진행되면 만성 위축성 위염(chronic atrophic gastritis)으로 진행한다고 하였다[8]. 이후 상부위장관 내시경의 사용이 활발해지면서 다양한 분류법이 제시되었다가 1990년 헬리코박터 파일로리가 위염의 원인으로 밝혀진 뒤 이를 적극적으로 위염의 분류에 도입한 시드니 분류 체계가 발표되었다[9]. 이 분류 체계는 유럽 의사들 위주로 마련된 분류법으로, 이후 1996년 미국 병리 의사들이 참여한 updated Sydney system이 발표되었다[10]. 이후 2015년에는 일본 의사들을 중심으로 헬리코박터 파일로리 감염의 위염 소견이 강조된 교토 분류 체계가 발표되어 사용되고 있다[11].
교토 분류 체계(Kyoto classification)는 내시경적 위염의 소견과 헬리코박터 파일로리 감염 사이의 관련성을 더욱 강조한 분류법이다[11]. 하지만 19개의 소견이 나열식으로 되어 있어 분류 체계가 다소 복잡하기 때문에 빈도나 의미가 적은 소견을 정리할 필요가 있다[12]. 예를 들어 미만성 발적(diffuse redness), 점상 발적(spotty redness), 반상 발적(patchy redness), 측선상 발적(red streak)과 같은 소견이 어떻게 다른지 명확한 설명이 부족하여 보완이 필요하다. 그리고 내시경적 위염 소견과 헬리코박터 파일로리 감염과의 관련성에 대한 국내 데이터가 부족한 실정이다. 이에 본 연구에서는 내시경적 위염에 대한 분류가 체계적으로 되어 있는 시드니 분류 체계(Sydney classification)의 내시경적 위염 소견과 중증도가 헬리코박터 파일로리 감염을 예측하는 데 얼마나 도움이 되는지 알아보고자 하였다[9]. 시드니 분류 체계에는 여러 가지 내시경적 위염 소견이 제시되어 있으나 기존 연구에서 헬리코박터 파일로리 감염과의 연관성이 제시되고 있으면서 연구자가 객관적으로 판단하기에 용이한 지표인 발적성 위염(erythematous gastritis)을 중심으로 헬리코박터 파일로리 감염률을 분석하고자 하였다[13]. 발적과 삼출이 동시에 있는 발적성/삼출성 위염의 중증도에 따른 헬리코박터 파일로리의 감염률은 이미 연구가 된 바 있어 본 연구에서는 발적성 위염만을 대상으로 하였다[14]. 발적성 위염은 시드니 분류 체계에서 경도, 중등도, 중증의 세 단계로 구분하고 있는데, 발적성 위염의 정도가 심할 경우 헬리코박터 파일로리 감염이 있을 가능성이 높을 것으로 예상되어 발적성 위염의 중증도에 따른 감염 빈도의 차이를 조사하였다.
대상 및 방법
연구 집단
본 연구에는 이전의 발적성/삼출성 위염 연구에서 전향적으로 구축한 코호트를 대상으로 하여 2019년 10월부터 2020년 9월까지 한솔병원에 건강 검진을 목적으로 내원한 18-75세의 수검자가 포함되었다. 연구에 동의한 환자를 대상으로 위내시경을 시행하고 내시경 소견을 기술한 뒤 발적성 위염의 소견을 보이는 환자를 대상으로 분석하였다. 내시경 검사를 시행한 환자 중 이전에 위 수술을 받았던 환자, 위암 또는 헬리코박터 파일로리 감염 진단을 받았던 환자, 검사 전 4주 이내에 비스테로이드성 소염진통제, 항혈소판제, 항응고제, 스테로이드, 항생제, 프로톤펌프억제제를 복용한 환자, 이전에 헬리코박터 파일로리 제균 치료를 받았던 환자, 위궤양 또는 십이지장궤양 과거력이 있는 환자, 빈혈, 출혈성 경향의 혈액 질환 환자, 심한 간 질환 환자, 신장 질환 환자, 심폐기능 저하 환자는 연구 대상에서 제외하였다. 이 연구는 한솔병원 임상연구윤리위원회의 승인을 받았다(IRB No. HSHIRB2019002). 검사자(OZK)가 전체 내시경 검사를 진행하였고 내시경 소견에 대한 평가를 하였으며, 다른 평가자(KHR)는 검사 영상을 다시 판독하여 발적성 위염의 중증도를 재평가하였다.
발적성 위염의 내시경 소견을 보인 환자에게 관찰된 발적 주위에서 급속 요소분해효소 검사(Campylobacter-like organism test) (CLO® test; Kimberly-Clark, Roswell, NM, USA)를 시행하여 양성 또는 음성을 판정하였다. 시드니 분류에서 발적(erythema)은 주변 점막에 비해 좀 더 어둡게 붉은 점막이 불균일하게 군데군데(patchy) 구별되어 있는 영역으로 정의된다. 또한 발적만 있을 경우에는 발적성 위염, 발적과 삼출물이 동시에 있을 경우에는 발적성/삼출성 위염이라고 표시한다. 본 연구에서는 발적과 삼출물이 동시에 있는 발적성/삼출성 위염은 제외하고 발적만 있는 발적성 위염만을 대상으로 하였다. 발적성 위염의 중증도는 발적이 약간이지만 명백한 변화(minimal but obvious change)를 보일 때 경도, 식별 가능한 반상의 변색(patchy discolouration)을 보일 때 중등도, 짙은 붉은색(beefy-red)의 변화를 보일 때 중증으로 분류하였다(Fig. 1) [9]. 그리고 헬리코박터 파일로리 양성은 급속 요소 분해효소 검사 양성으로 정의하였다.

Endoscopic findings of erythematous gastritis. (A) Mild erythematous gastritis is characterized by minimal erythema but the presence of obvious change. (B) Moderate erythematous gastritis is characterized by conspicuous patchy discoloration. (C) Severe erythematous gastritis is characterized by a color change that is beefy-red in intensity.
연구 결과 지표
연구의 일차 결과 지표(primary study outcome)는 경도 또는 중등도 발적성 위염을 중증 발적성 위염과 비교하여 헬리코박터 파일로리 감염률이 차이가 있는지를 분석하였다. 이차 결과 지표(secondary study outcome)는 발적성 위염 환자에서 헬리코박터 파일로리 감염에 연관되는 인자를 분석하였다.
통계적 분석
2016년부터 2017년까지 진행한 국내 연구에서 헬리코박터 파일로리 감염률은 약 42%였다[15]. 경도 혹은 중등도의 발적성 위염 환자에서의 헬리코박터 파일로리 감염률을 25%, 중증의 발적성 위염 환자에서의 헬리코박터 파일로리 감염률을 50%라고 가정하고, 검정력을 80%, 유의수준 0.05(양측검정), 중도탈락률은 10%로 설정하였다. 상기 조건을 통해 계산된 표본 수는 128명이었다.
수집된 데이터를 바탕으로 헬리코박터 파일로리 감염 여부에 따라 경도/중등도 대비 중증 발적성 위염이 유의하게 차이가 있는지에 대해 Fisher’s exact test와 다변량 로지스틱 회귀 분석을 시행하였고, p-value가 0.05 미만일 때 통계적으로 유의하다고 평가하였다. 상기 통계적 분석은 SPSS statistics ver. 27.0 (IBM, Armonk, NY, USA)으로 시행하였다.
결 과
연구 대상자들의 특성
총 1,801명의 대상자가 연구 참여에 동의하여 등록되었고, 이 중 참여를 철회한 3명을 제외한 1,798명에 대하여 위 내시경 검사를 통해 스크리닝을 진행하였다. 발적성 위염 소견이 없었던 1,667명은 연구에서 배제되었고, 발적성 위염이 있었던 131명에 대해 연구가 진행되었다. 131명 중 남성은 62명 여성은 69명이었고, 경도 발적성 위염은 45명, 중등도 발적성 위염은 43명, 중증 발적성 위염은 43명이었다. 전체 발적성 위염 환자에서 헬리코박터 파일로리 감염 환자가 차지하는 비율은 45.8%였다. 세 군 사이에 고혈압과 다른 암 과거력이 중증 발적성 위염 환자군에서 유의하게 높은 비율로 나타났으나, 성별, 나이 그리고 다른 기저 특성에 대해서는 군 간 유의한 차이를 보이지 않았다(Table 1).
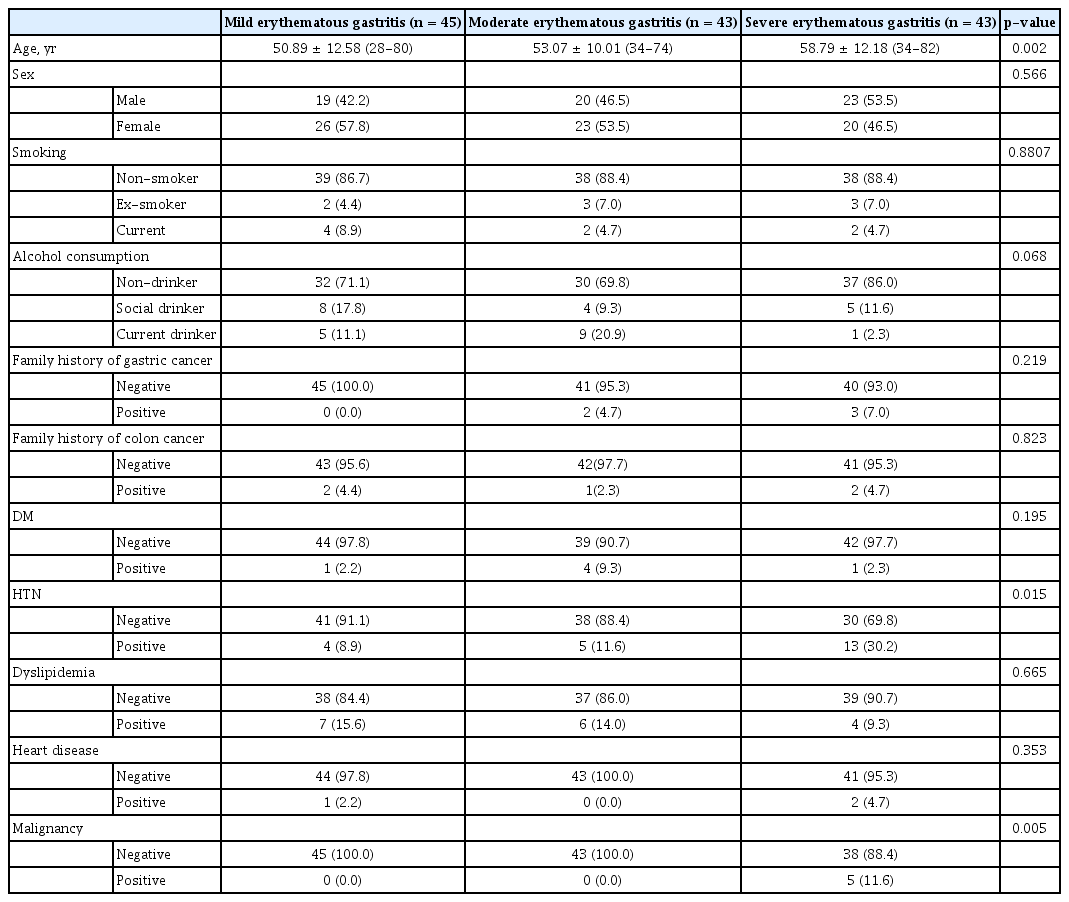
Baseline characteristics of patients with erythematous gastritis
연구 결과
일차 결과 지표인 발적성 위염의 중증도에 따른 헬리코박터 파일로리 감염률을 보기 위해 경도 혹은 중등도 발적성 위염과 중증 발적성 위염을 비교 분석하였다. 그 결과 헬리코박터 파일로리 감염률은 경도 혹은 중등도 발적성 위염에 비해 중증 발적성 위염에서 유의하게 높은 비율로 나타났다(경도 혹은 중등도 발적성 위염 20.5%, 중증 발적성 위염 97.7%, p= 0.000) (Table 2).

Comparison of mild to moderate erythematous gastritis with severe erythematous gastritis
헬리코박터 파일로리 감염에 영향을 미치는 인자를 분석하기 위해 발적성 위염의 중증도를 공변량으로 포함하여 로지스틱 회귀 모델로 분석하였을 때, 발적성 위염의 중증도는 헬리코박터 파일로리 감염과 연관이 있었으며, 다른 기저 특성 중에서는 유의한 인자를 발견할 수 없었다(Table 3).

Logistic regression analysis to identify factors associated with H. pylori infection
두 내시경 의사(OZK, KHR)의 코헨의 카파 계수(kappa value)는 0.563으로 중등도(moderate)로 나왔고 관찰자 간 차이(relative interoberver variation)는 절대적 차이(absolute difference) 가 14.43%, 개인 간 표준분포(individual standard deviation) 가 2.52%로 측정되었다(Table 4).

Comparison of erythematous gastritis assessed by two different endoscopists
고 찰
본 연구에서는 발적성 위염의 중증도에 비례해서 헬리코박터 파일로리 감염 가능성이 높을 것이라 예측하였다. 하지만 경도의 발적성 위염과 중등도의 발적성 위염은 헬리코박터 파일로리의 감염률이 비슷하였고 중증의 헬리코박터 파일로리 감염률은 뚜렷하게 높았다. 발적성 위염이 있는 전체 연구 대상자에서의 헬리코박터 파일로리 감염률은 45.8%로 국내 일반 인구 집단의 감염률인 42%와 큰 차이가 없음을 확인하였고, 경도 및 중등도의 발적성 위염 환자의 헬리코박터 파일로리 감염률은 20.5%인데 반해 중증의 발적성 위염 환자의 헬리코박터 파일로리 감염률은 97.7%였다[15]. 따라서 중증 발적성 위염 환자에서 헬리코박터 파일로리 검사를 적극적으로 시행해야 함을 알 수 있다. 또한 경도 및 중등도의 발적성 위염 환자에서도 20% 이상은 헬리코박터 파일로리 감염 양성이므로 고위험군에서 선택적으로 검사를 해 볼 수 있겠다.
국내 다른 연구에서는 교토 분류의 내시경 소견을 적용하여 헬리코박터 파일로리 감염을 예측할 수 있는 인자를 연구하였다. 점막 부종, 백탁 점액은 상대적으로 높은 양성 예측도를 보였고, 역류성 식도염, 헤마틴(hematin), 측선상 발적(red streak), 십이지장염은 높은 음성 예측도를 보였다[16]. 일본에서 시행된 연구에 의하면 헬리코박터 파일로리 감염을 예측할 수 있는 내시경적 소견은 다음과 같다: 미만성 발적(diffuse rednes), 반상 발적(patchy redness), 두꺼워진/구불구불한 점막 주름(enlarged, tortuous fold), 점막 부종(mucosal swelling), 위소구 부종(swelling of areae gastricae), 결절형 변화(nodular change), 점상 발적(spotty redness), 융기 미란(raised erosion) 등[17]. 이 중에서 미만성 발적은 민감도가 83.4%, 점상 발적은 70.3%로 본 연구의 중증 발적성 위염의 분석 결과와 근접한 수치를 보였고, 반상 발적은 민감도가 30.8%, 측선상 발적은 5.5%로 상대적으로 낮은 수치를 보였다. 이로 보아 반상 발적과 측선상 발적은 반상의 발적을 특징으로 하는 중등도 발적성 위염으로 분류할 수 있을 것이다. 따라서 교토 분류와 같이 발적의 모양으로 판단하기보다는 중증 발적성 위염의 특성인 짙은 붉은색이라는 발적의 색상을 기준으로 헬리코박터 파일로리 감염의 유무를 예측하는 것이 좀 더 용이할 것으로 보인다.
헬리코박터 파일로리 감염이 발적성 위염을 일으키는 기전을 직접적으로 밝힌 연구는 존재하지 않는다. 하지만 급성 염증과 발적과의 관계는 다음과 같이 설명된다. 급성 염증이 발생하면 작은 혈관이 확장되어 혈류가 증가하고, 미세혈관 구조의 투과성이 증가하여 혈장 단백질과 백혈구가 순환계를 나오게 된다. 이후 혈관 밖으로 나온 백혈구가 염증 부위에 축적되어 병원균을 제거하기 위해 활성화된다. 여기서 혈류가 증가하는 과정 때문에 염증이 발적으로 나타나는 것으로 생각된다[13,18]. 이러한 병인론 때문에 중증 발적성 위염에서 헬리코박터 파일로리가 높은 빈도로 발견되는 것으로 추측된다.
본 연구의 제한점으로는 단일 기관의 단일 검사자가 수행한 연구로 시드니 분류를 판정하는 데 있어 코헨의 카파 계수와 관찰자 간 차이를 측정하였으나 카파 계수가 중등도로 높지 않고 관찰자의 수가 2명으로 부족하다는 점을 들 수 있다. 따라서 본 연구 결과를 일반화하기 위해서는 더 많은 검사자가 포함된 더 큰 규모의 다기관 연구가 필요하다. 그리고 발적성 위염의 중증도를 발적 색의 짙은 정도로만 하기에는 객관성이 떨어지기 때문에 관찰자 간 차이를 극복하기 위해서 추후 발적 정도를 평가할 수 있는 객관적 지표의 개발이 필요하다. 또한 발적성 위염이 없는 대상자를 연구에 포함시키지 못했기 때문에 발적성 위염 자체가 헬리코박터 파일로리 감염과 얼마나 연관성이 높은가에 대해서는 평가할 수 없었다는 제한점이 있다. 그리고 과거 헬리코박터 파일로리 감염이 있었던 환자나 이전에 헬리코박터 파일로리 제균 치료를 받았던 환자를 분석에 포함시키지 않았기 때문에 헬리코박터 파일로리 감염 후 변화하는 위염의 중증도를 평가하지 못하였다. 마지막으로 급속 요소분해효소 검사만으로 헬리코박터 파일로리 감염을 판정했기 때문에 급속 요소분해효소 검사의 위음성으로 인해 헬리코박터 파일로리 감염률이 저평가되었을 가능성도 존재한다. 따라서 추후에는 헬리코박터 조직 검사(hematoxylin and eosin stain, Giemsa stain 등), 헬리코박터 항체 혈청 검사, 요소 호기 검사 등을 추가로 시행하여 연구의 정확도를 높일 필요가 있다.
그럼에도 불구하고 본 전향적 연구는 발적성 위염의 중증도가 헬리코박터 파일로리 감염을 예측하는 데 연관이 있는지를 확인한 최초의 연구로, 중증의 발적성 위염에서 헬리코박터 파일로리 감염률이 유의하게 높으므로 해당 소견을 보이는 환자에서 헬리코박터 검사를 적극 고려해야 함을 알 수 있다.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Research design: Z.O.K.
Research method: K.H.R.
Data collection: Z.O.K.
Statistical analysis: Z.O.K.
Manuscript writing: I.H.O.
Manuscript correction: K.H.R., Z.O.K., I.H.O.
Acknowledgements
None.