2021 대한부정맥학회 심방세동 환자의 새로운 접근법 및 통합적 관리 지침
The 2021 Korean Heart Rhythm Society Guidelines for a New Approach and Integrated Management of Atrial Fibrillation
Article information
Trans Abstract
The prevalence of atrial fibrillation (AF) is gradually increasing with the aging of the population, and there is also increasing interest in AF with the development of various single-lead electrocardiography measurement methods for diagnosis. Further, the current diagnosis and treatment policies for AF do not reflect its progression and complexity. In addition, the various factors related to AF diagnosis and treatment are not simple due to the diversification of tools, advances in treatment methods, and complex mechanism of AF. Therefore, there are many challenges to developing a simple AF classification system. To overcome these, there have been a number of attempts to systematically characterize AF according to treatment and prognosis rather than using a uniform classification. Further, as mentioned in the previous AF guidelines, further research is being conducted on an integrated patient–physician approach to AF. Such an approach would be the basis for consistent treatment based on the guidelines, and would help to improve patient outcomes. Further, for the integrated management of AF patients, some changes should be made to the current approach to develop a multidisciplinary approach, including changes to the behavior of team members, patients, their family members, and physicians. The Korean Heart Rhythm will introduce an integrated approach to the classification and structure of AF management, and provide guidelines for its application in clinical practice.
서 론
심방세동(atrial fibrillation, AF)은 인구의 고령화에 따라 유병률이 점차 증가하고 있으며, 최근 진단을 위한 다양한 심전도 측정 방법이 출시되면서 이에 대한 관심도 증가하고 있다. 그럼에도 현재까지의 심방세동에 대한 진단 및 치료방침은 심방세동의 시간에 따른 변화를 반영하고 있지 않다[1-4]. 이에 따라 심방세동에 대한 통합적인 접근법은 가이드라인에 근거한 심방세동의 일반적인 치료의 근간이 되며 환자의 치료 성적을 향상시키는 데 도움을 준다. 통합적 치료를 통한 예후 향상에 대해서는 국내 환자를 통한 분석에서도 잘 보고되고 있다[5-7]. 심방세동 환자에 대한 통합 관리에서는 모든 심방세동 팀 구성원과 환자와 가족을 포함한 주요 이해 관계자의 행동 변화를 포함하며, 다학제적 접근을 수행하기 위한 기존의 접근 방식까지도 일부 변경해야 한다.
본 론
심방세동 환자의 새로운 접근법
다양한 심방세동 분류 방법들이 있으나 전통적으로는 임상 양상, 유병 기간, 그리고 저절로 종료되는가의 여부에 따라 표 1과 같이 분류된다. 발작성 심방세동의 경우 7일 이내에 정상 동율동으로 전화되는 형태를 말하며, 지속성 심방세동의 경우 7일 이상 지속되며, 항부정맥제나 전기적 동율동 전환술 등의 방법을 사용해야만 심방세동이 종료되는 경우를 말한다. 그외 “long standing persistent”의 경우 진단 당시 이미 1년 이상의 심방세동이 지속된 경우를 말하며, “permanent”의 경우는 환자와 주치의가 정상 동율동으로 전환하기 위한 시도를 더 이상 하지 않기로 동의한 경우로 정의한다. 그리고 lone AF, valvular AF, and chronic AF의 경우 의료진과 환자에게 혼란을 일으킬 우려가 있으며, 정의가 주관적인 부분이 포함되어 있어 사용을 권고하지 않는다.
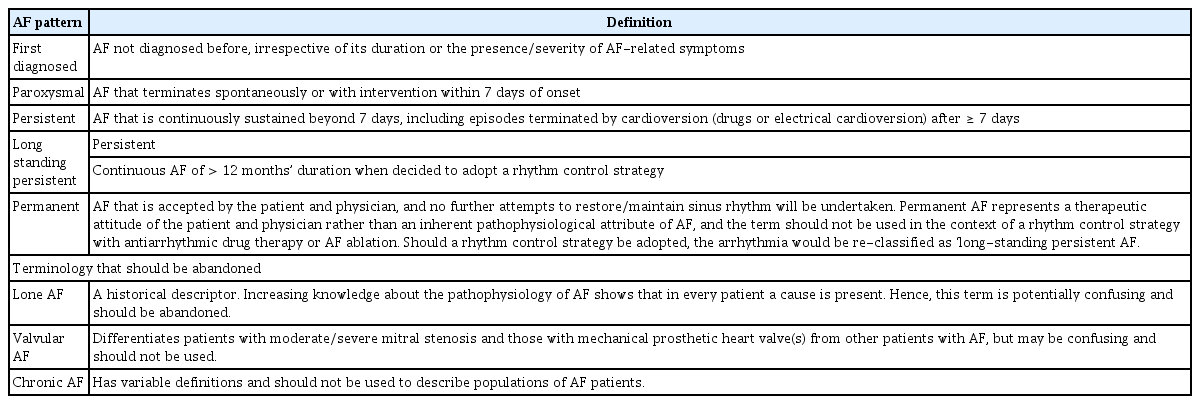
Classification of AF
발작성과 지속성 심방세동이 둘 다 있는 경우, 보다 우세한 표현형을 사용해야 한다. 심방세동의 다른 분류로는 증상의 여부(무증상 심방세동 등)나 심방세동의 원인(수술 후 심방세동 등)에 따라 분류하기도 하며 이러한 분류는 치료 선택에 도움이 될 수는 있으나 임상적 유용성은 높지 않다.
하지만 이러한 심방세동의 분류만으로 리듬 치료 이외에 전반적인 심방세동의 치료 방향을 결정하기는 어렵다. 또한, 심방세동 모니터링의 발전, 위험도 예측 도구의 다양화, 치료의 발전 그리고 심방세동의 복잡성 등으로 인해 간단하면서도 통합된 심방세동 분류 체계를 만드는 데 있어 어려움이 많다. 이러한 한계를 극복하기 위해, 최근에는 심방세동을 치료 및 예후에 따른 영역으로 구분 짓고 구조적 특성화를 이루고자 한다. 2020년 발표된 유럽심장학회 진료 지침에서는 심방세동과 관련된 네 가지 영역을 4S-AF로 제시하였다(Fig. 1) [8]. 개별 심방세동 환자를 뇌졸중 위험도(stroke risk), 증상(symptom severity), 심방세동의 양적 평가(severity of AF burden) 그리고 심방세동 기질(substrate severity)을 측정하게 된다. 일반적으로 심방세동의 처음 진단 당시 환자에게 발생 가능한 뇌졸중의 위험을 평가하고(stroke risk), 질병의 치료에 대한 필요성을 환자에게 설명하는 것이 중요하며, 실제 환자가 느끼는 증상의 심각성(symptom severity)을 객관화해서 보여주는 것은 환자의 치료 순응도를 높이는 데 중요할 것으로 생각된다. 그리고 환자의 심방세동에 대한 양적 평가(severity of AF burden)는 증상 발현의 빈도, Holter 및 심전도를 통한 심방세동의 기간 및 주기에 대한 객관적인 지표를 통해 확인이 가능하며, 심장에 대한 영상학적 검사(cardiac magnetic resonance imaging, computed tomography, 심초음파)와 혈액 검사 등을 통해 이해 대한 추가적인 상태 평가(substrate severity)를 수행할 수 있다.
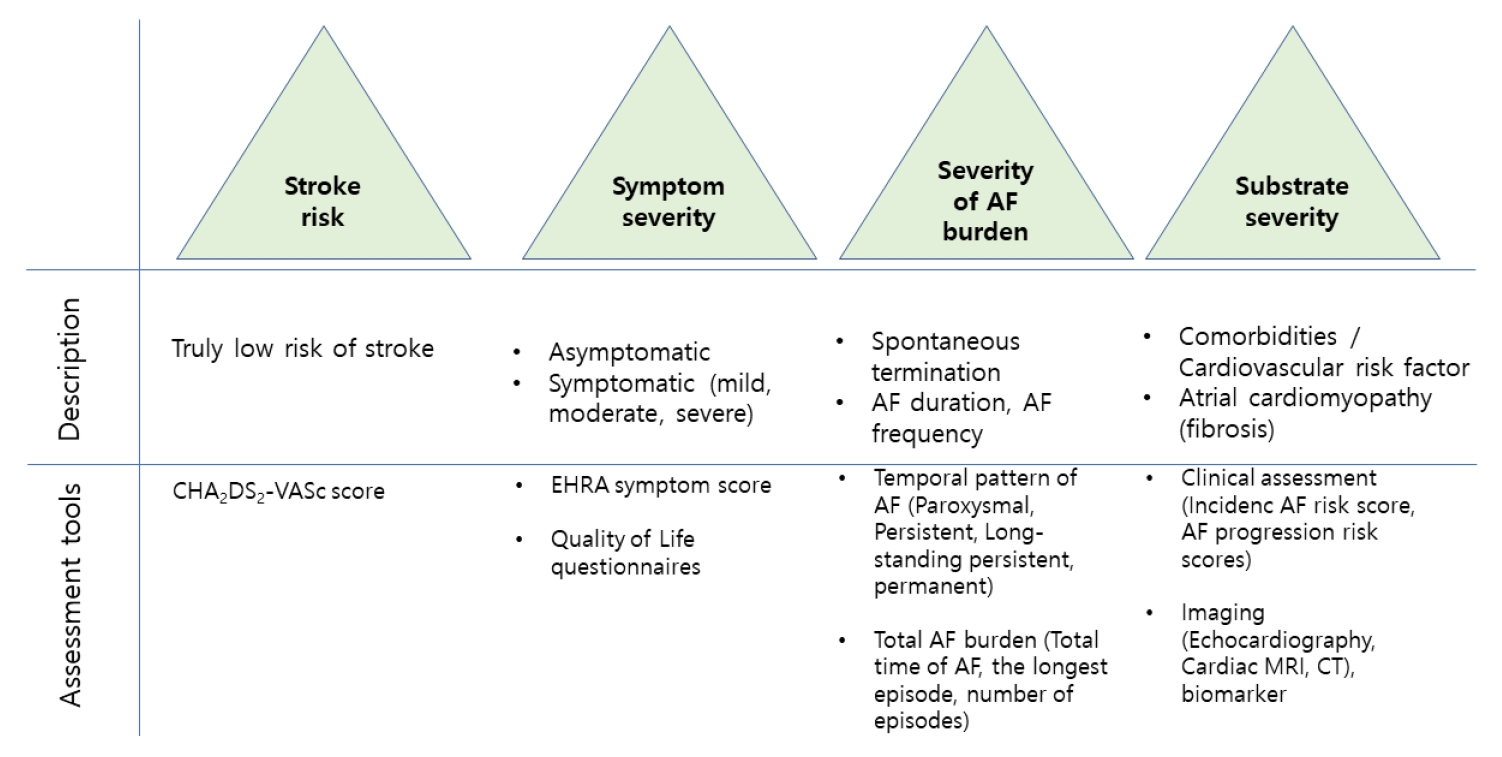
4S-AF scheme as an example of structured characterization of AF. AF, atrial fibrillation; CT, computed tomography; MRI, magnetic resonance imaging.
심방세동의 양적 평가(burden)라는 용어는 다양한 역학적, 경제적 요소들을 포함하고 있다. 연속적인 기기 모니터링에서 측정된 심방세동의 양적인 평가는 모니터링 기간 동안에 심방의 빠른 전기 신호(atrial high rate event) 또는 무증상 심방세동(subclinical AF) 상태로 있던 기간으로 정의한다. 대부분의 연구들이 24시간 모니터링 기간을 보고하고 있으나 가장 적절한 모니터링 방법에 대해서는 아직 논란이 많다[9]. 최근 무작위 배정 연구들에서는 발작성 심방세동이 지속성 심방세동에 비해 혈전 색전증 비율이 낮은 경향을 보이며, 이는 과거 무작위 배정 혹은 관찰 연구들과는 다소 다른 결과를 보이고 있다. 항응고 치료를 하지 않은 환자들에서 발작성 심방세동은 지속성에 비해 뇌경색 위험도가 낮으며, 심방세동의 양적 평가의 증가는 혈전 색전증 위험도의 증가와 독립적인 연관성을 보였다[10,11]. 1주일에 6시간 이상, 특히 24시간 이상 심방세동이 지속될 경우 특히 여성에서 사망률을 증가시킬 수 있다[12]. 그러나 아직까지 심방세동 양적 평가와 관련된 합병증의 증가에 대한 정보는 부족한 편이라 치료 결정에서의 역할은 제한적이며, 심혈관계 위험인자 및 동반 질환에 대한 통합적인 치료를 통해 심방세동에 대한 치료 부담을 줄일 수 있다.
심방세동의 통합적 관리
심방세동의 통합적 관리의 정의 및 구성
심방세동의 통합적 관리 지침은 심방세동 환자 중심의 진단과 치료를 위한 다학제적 팀 접근 방식을 통해 최적의 치료 성과를 만들어 내는 과정을 말한다(Fig. 2). 이러한 접근 방식의 중심에는 환자가 있으며, 새로운 질병의 위험 요인, 증상 발현, 심방세동의 진행과 새로운 치료 방식의 적용에 대한 전문가들의 협진과 토론 과정이 이루어진다(Fig. 3).
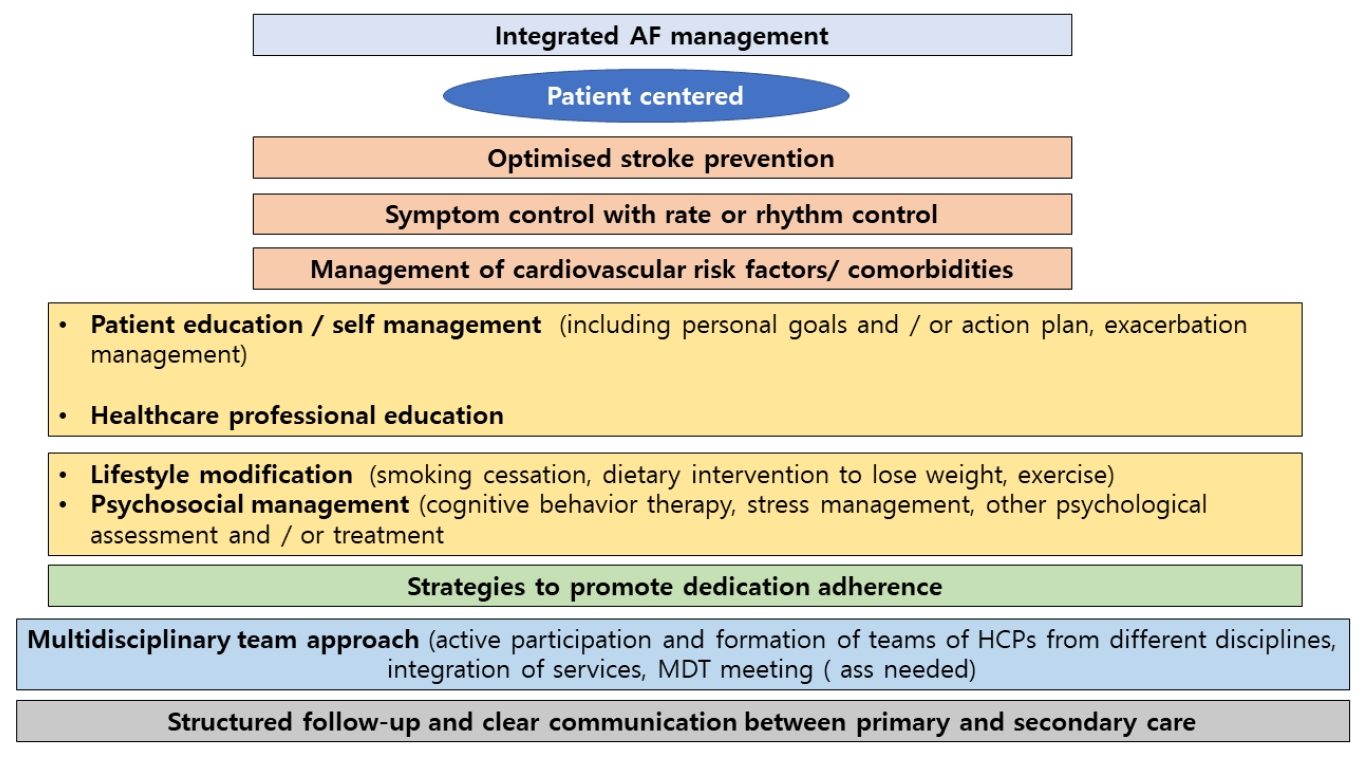
Components of integrated AF management. AF, atrial fibrillation; HCP, healthcare professional; MDT, multidisciplinary team.
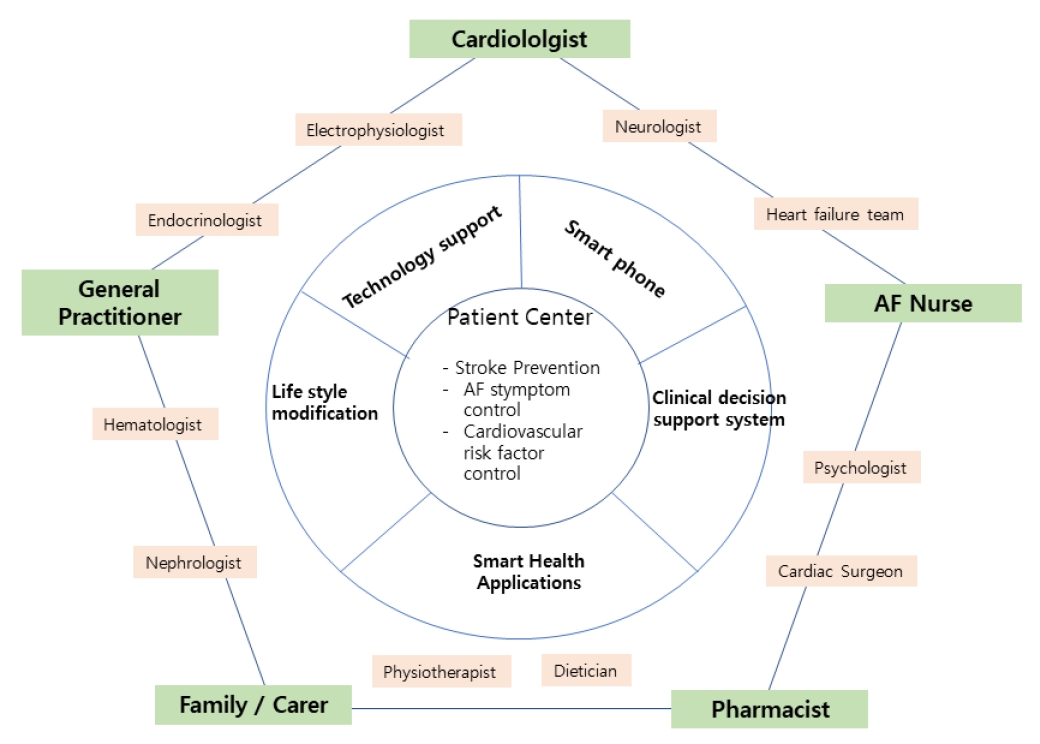
Integrated AF management team. The figure shows an example of the potential composition of AF teams with a variety of different specialists to support individual patients as needed. According to local standards, this could be a general cardiologist with special interest in arrhythmia/AF or an electrophysiologist. AF, atrial fibrillation.
다학제 심방세동 팀
심방세동의 통합적 치료를 위해서는 다학제 팀 접근 방식이 필요하다(Fig. 3). 여러 가지의 위험요인을 가지고 있는 환자일수록 1차 의료인과 관련 의료 종사자 그리고 부정맥 관련 전문가를 포함한 다학제 접근 방식의 혜택을 많이 받게 된다. 최적의 심방세동 치료는 이러한 체계화된 의료 전달시스템과 관련 의료인들 간의 원활한 의사소통을 기본으로 하며, 궁극적으로는 뇌졸중의 감소, 심방세동 증상의 감소 그리고 관련 심혈관 질환을 적절히 관리하는 데 그 목적이 있다.
환자 참여 및 공유된 의사 결정
환자 참여 의사 결정을 위해서는 환자의 가치, 목표, 그리고 선호 사항을 먼저 확인해야 한다[13,14]. 이전의 연구에 따르면 의사 중심적인 의사 결정 과정을 경험한 환자들과 보호자들 사이에 의견 불일치가 있어 왔고, 많은 환자들이 치료를 위한 의사 결정에 관여하지 않고 오히려 그 결정을 의사에게 미루기도 한다[8]. 의사 결정을 공유하기 위해서 환자가 뇌졸중 예방과 리듬 조절에 두는 의미와 그에 상응하는 사망, 뇌졸중 그리고 출혈 위험 및 치료에 대한 부담이 철저하게 평가 및 고려되어야 한다.
환자가 가진 심방세동 질병과 치료에 대한 지식 수준은 특히 진단 초기에 가장 낮을 수밖에 없는데, 이 시기에 주로 치료 방침이 논의되고 결정된다. 심방세동에 대한 다양한 일반인 교육 자료를 대한부정맥학회 홈페이지(http://www.k-hrs.org/)에서 다운로드 받을 수 있다.
의료 전문가 교육
통합적 치료를 위해서는 의료인의 교육도 중요하다. 스마트 기술을 이용하거나 온라인 소스를 이용하기도 하며 대면 워크숍을 하기도 하는 등 개개인의 요구도에 따른 맞춤형 교육이나 트레이닝이 복합적이고 다양한 방법이 있다[15]. 심방세동과 관련하여 개원의 및 전문가를 위한 각종 교육 자료를 대한내과학회 혹은 대한부정맥학회 홈페이지(http://www.k-hrs.org/)에서 다운로드 받을 수 있다. 하지만, 단지 교육만으로 의료 전문가들의 치료 행태를 변화시키기는 어렵다[16]. Integrated Management Program Advancing Community Treatment of Atrial Fibrillation (IMPACT-AF) 연구[17]에 따르면, 의료 전문가를 대상으로 교육과 피드백을 포함하는 다각도의 교육 개입을 하게 되었을 때 항응고 치료를 받는 환자의 비율이 크게 증가하였다는 것이 확인되었다.
치료 순응도
치료 순응도에 영향을 미치는 요소는 크게 환자 요인(나이, 성별, 동반 질환, 인지기능, 다약제 복용, 치료 부작용, 정신 건강, 치료 방침에 대한 환자의 이해도), 의사 요인(지식, 가이드라인 숙지, 다학제 팀적 접근법) 그리고 의료 시스템 요소(업무 환경, 의료 접근성, 비용) 등이 있다[18]. 여러 치료 옵션, 어떻게 치료에 순응할지, 치료에 순응하지 못할 때 발생할 수 있는 결과에 대해서 환자에게 적절한 정보를 제공하는 것은 치료 목표에 대한 환자의 기대치를 충족시켜주는 것에 더하여 치료 순응도를 올리는 데에도 무척 중요하다. 다학제 팀의 정기적인 검토를 통하여 순응도가 낮은 경우를 식별해내고 이를 개선하기 위한 전략을 짜도록 노력해야 한다.
디지털 기술의 도입
임상 진료 지원 시스템은 시기에 맞는 환자 맞춤형 근거 중심 치료를 용이하게 해주는 알고리즘과 임상 진료 과정 및 가이드라인을 디지털화하고 제공해주는 지능형 시스템이다. 많은 나라에서 이러한 모바일 프로젝트[19]와 몇 가지 애플리케이션들은 환자 교육을 강화하고 환자와 의료 전문가 사이의 의사 소통을 원활하게 하며 환자 참여를 활발히 할 목적으로 활용되고 있다. 이렇게 환자의 의사 결정을 보조하는 기술이 발전하게 되면 치료 방침 결정 시 발생할 수 있는 의사 충돌을 줄여준다고 알려져 있다[20]. 그럼에도 불구하고, 이러한 개입과 실제 환자 예후의 관련성에 대해서는 아직 명확한 결론이 나지 않은 상태이므로[21], 향후 보다 주의 깊게 디자인된 연구가 필요할 것이다.
심방세동 통합적 관리의 장점 및 구현 방법
지금까지 심방세동의 통합적 관리 효과에 대한 발표된 연구들은 적용된 통합 관리의 내용과 수가 매우 다양하여 비교가 어려우며 다양한 결과를 보여주고 있다. 심방세동의 일반적 관리보다 간호사 주도의 전문적 통합 관리를 하거나 심방세동 클리닉으로 보내서 간호사와 의사의 관리를 받는 것이 심혈관 관련 입원 및 사망률이 통계적으로 의미 있게 낮아진다고 보고한 임상 연구와 메타분석 연구가 있다[22-24]. 반면, 다른 연구에서는 통합 치료가 이러한 결과에 미치는 영향이 없다고 보고하였다[25]. 한 무작위 연구에서는 다각적이고 다면적 환자 교육의 개입이 뇌졸중의 위험이 있는 심방세동 환자의 경구용 항응고제 치료 비율을 의미 있게 높인 결과를 보여주었다[17]. 그러나 IMPACT-AF 연구는 응급실 방문 혹은 심혈관 관련 입원 또는 주요 출혈 위험 결과에서 중재 그룹과 일반 치료 사이에 유의한 차이가 없음을 보고하였다[26].
심방세동 통합 관리는 모든 심방세동 팀 구성원(간호사, 순환기 전문의, 일반의, 약사)과 환자와 가족을 포함한 주요 이해 관계자의 행동 변화를 포함하여, 스마트폰 애플리케이션을 활용한 다양한 소프트웨어 및 병원 검사 기구 등의 다양한 기술적인 지원이 이루어져야 한다(Fig. 3). 그리고 다학제적 접근을 수행하기 위해서는 환자 치료의 현재 접근 방식을 근본적으로 변경해야 한다[27,28]. 심방세동의 통합 관리가 임상 진료에 적용되고 이러한 접근법으로 인해 사망, 뇌졸중, 입원, 삶의 질, 증상 감소 등의 주요 임상 결과에 어떠한 영향을 미쳤는지 이해하기 위해서는 국제 표준 결과에 대한 측정이 동시에 이루어져야 한다.
치료 부담(treatment burden)
환자가 인지하는 치료 부담(patient-perceived treatment burden)은 특정 치료 부작용과는 별도로 환자의 기능과 삶의 질에 미치는 영향으로 치료 과정에서의 부담으로 정의 내릴 수 있다. 여기에는 환자가 건강을 위해 수행하는 약물 관리, 자가 모니터링, 의사 방문, 혈액 검사, 생활습관 변화 등이 포함된다. 또한 입원이나 생존율 등의 치료 결과와 치료 순응도 및 삶의 질에 영향을 주는 잠재적 사회적 관계에 대한 치료 과정의 영향도 포함된다. 환자가 인지하는 치료 부담은 질환에 대한 지식의 영향을 받는다.
여러 만성 질환을 가진 환자들의 치료 부담은 가중될 수 있다. 최근 심방세동에 대한 비용 부담에 대한 대한민국의 연구 자료는 2006년 이후 환자가 부담하는 입원을 비롯한 전체 의료 비용 부담이 지속적으로 증가하는 것으로 나타났다[4,29]. 특히, 심방세동 환자는 치료 관련 측면의 병원 방문과 생활습관 변경의 요구에 대한 치료 부담이 가장 높은 비율을 차지하였다. 여성과 젊은 연령 및 영구형 심방세동일수록 높은 치료 부담과 관련이 높은 것으로 나타났으며, 비 비타민 K 길항제 경구 항응고제(non-vitamin K oral anticoagulant) 및 전기적 동율동 전환술은 치료 부담을 50% 이상 감소시켰다[30]. 치료 부담에 대한 논의는 치료 의사 결정에 공유되어야 하고 검증된 설문지를 사용하여 평가할 수 있다.
환자 보고 결과(patient-reported outcomes)
환자의 관점에서 치료를 개선하고 치료 성공을 평가하기 위해 환자 보고 결과(patient-reported outcomes)가 일상적 데이터로 수집되어야 하고 임상의 최종 결과로 포함시켜야 한다는 의견이 증가하고 있다. 심방세동에 대한 환자의 경험 및 관리는 매우 주관적이다. 심방세동의 관리는 점점 복잡해지고 있어 잠재적으로 상당한 치료 부담과 건강 관련 삶의 질의 저하를 초래할 수 있다. 사망, 뇌졸중, 주요 출혈 등의 임상 평가 변수와 함께 환자에게 중요한 결과를 측정하면 심방세동 관리에 도움이 될 수 있다. 심방세동 환자들과 헬스케어 전문가들로 구성된 국제 컨소시엄에서는 건강 관련 삶의 질, 신체 및 정서 기능, 인지 기능, 증상의 정도, 운동 능력, 작업 능력과 같은 심방세동의 측정에 중요한 환자 보고 결과를 확인하였다. 건강 정보 시스템은 환자 보고 결과 데이터를 획득하는 데 도움이 될 수 있다. 의료 관리에서 환자보고 결과 측정의 역할에 대한 지지가 증가함에도 불구하고 검증된 도구를 사용하여 환자 보고 결과 데이터를 수집하는 연구 및 레지스트리는 거의 없는 실정이다[31].
결 론
심방세동 환자의 통합적 관리 지침은 환자 중심의 심방세동에 대한 다학제적 팀 접근 방식을 통해 최적의 치료 성과를 만들어 내는 데 목적이 있다. 이를 위해서는 환자의 질병에 대한 인식과 교육이 필요할 것으로 보이며, 다학제적 팀에 속해 있는 전문가 집단들 간의 원활한 의사소통과 협진을 통한 의료 결정을 위한 시스템의 개발도 필요하다. 심방세동의 관점에서는 단순한 질병의 분류를 넘어 치료 및 예후에 따른 구조적 특성화를 위한 4S-AF 체계화가 중요하며, 환자의 치료 부담에 대한 자가 보고 결과를 활용한 임상적 적용과 연구가 필요할 것으로 보인다.
Acknowledgements
본 연구는 대한부정맥학회 및 보건복지부의 재원으로(환자중심 의료기술 최적화 연구사업[Patient-Centered Clinical Research Coordinating Center, PACEN])의 지원을 받았다(과제고유번호: HI19C0481, HI19C0622).