출혈을 동반한 위 지방종의 내시경적 점막 절제술을 이용한 내시경적 제거
Endoscopic Removal of Gastric Lipoma with Hemorrhage Using Endoscopic Submucosal Dissection
Article information
Trans Abstract
Most upper gastrointestinal lipomas occur in the duodenal second portion, and gastric lipomas are rare. Most lipomas are usually asymptomatic, but symptoms such as abdominal pain, intussusception, ulceration, and intestinal obstruction may occur depending on the size and location and, rarely, can cause bleeding. Endoscopic polypectomy, endoscopic mucosal resection, and surgical resection are the treatments of choice for lipomas with intestinal obstruction or bleeding. Upper gastrointestinal bleeding from lipoma is mostly of duodenal origin and very rarely from the stomach. Here, we report a case of successful treatment of gastric lipoma with massive bleeding by endoscopic resection.
서 론
위장관 지방종은 점막하층에 발생하는 양성 종양으로 전 장관에 걸쳐 발생 가능하며 대장과 소장에서는 공장, 회장에서 주로 발견된다[1,2]. 위장관 지방종에서 위 지방종이 차지하는 빈도는 5% [3,4]이며, 양성 위 종양의 3% [5,6]가 모든 위 종양의 1% 미만을 차지한다[4,7]. 대부분의 위 지방종은 무증상으로 우연히 발견되는 경우가 많으며 검진 위 내시경 중 0.36-0.76%의 발견 빈도로 드물지 않게 발견된다[1,4,8,9]. 지방종의 크기나 위치에 따라 크기가 2 cm보다 작은 경우 무증상인 경우가 많으며, 4 cm보다 큰 경우 소화불량, 복통, 설사, 변비, 궤양, 장 중첩증, 장 폐색증 등 다양한 증상을 보이며 드물게 출혈을 일으키기도 한다[1,2,10-15]. 지방종에 의한 상부위장관 대량 출혈은 대부분 십이지장 지방종에 의한 출혈이며, 위 지방종이 그 원인인 경우는 매우 드물다.
증상을 일으키는 지방종은 내시경적 용종 절제술, 내시경적 점막 절제술, 수술적 절제로 치료하는데[1,2], 본 증례는 대량의 출혈을 동반한 위 지방종을 내시경적 점막 절제술로 성공적으로 치료한 1예를 경험하였기에 문헌 고찰과 함께 보고하는 바이다.
증 례
71세 남자 환자가 내원일 발생한 300 cc가량의 토혈을 주소로 내원하였다. 내원 17개월 전 2014년 6월 2일 일반 건강 검진으로 시행한 상부위장관 내시경에서 위 하체부 후벽에 3 cm 크기의 표면 요철을 동반한 rolling 징후와 cushion 징후를 동반하지 않은 점막하 종양이 발견되어 주기적인 내시경으로 추적 관찰 중이었다(Fig. 1A). 조직 검사 결과 장상피화생을 동반한 만성 위염 소견이었다. 과거력에서 38갑년의 흡연력을 동반한 만성 폐쇄성 폐부전으로 호흡기내과에서 치료력 외 특이 소견은 없었으며 수술력이나 가족력도 없었다.
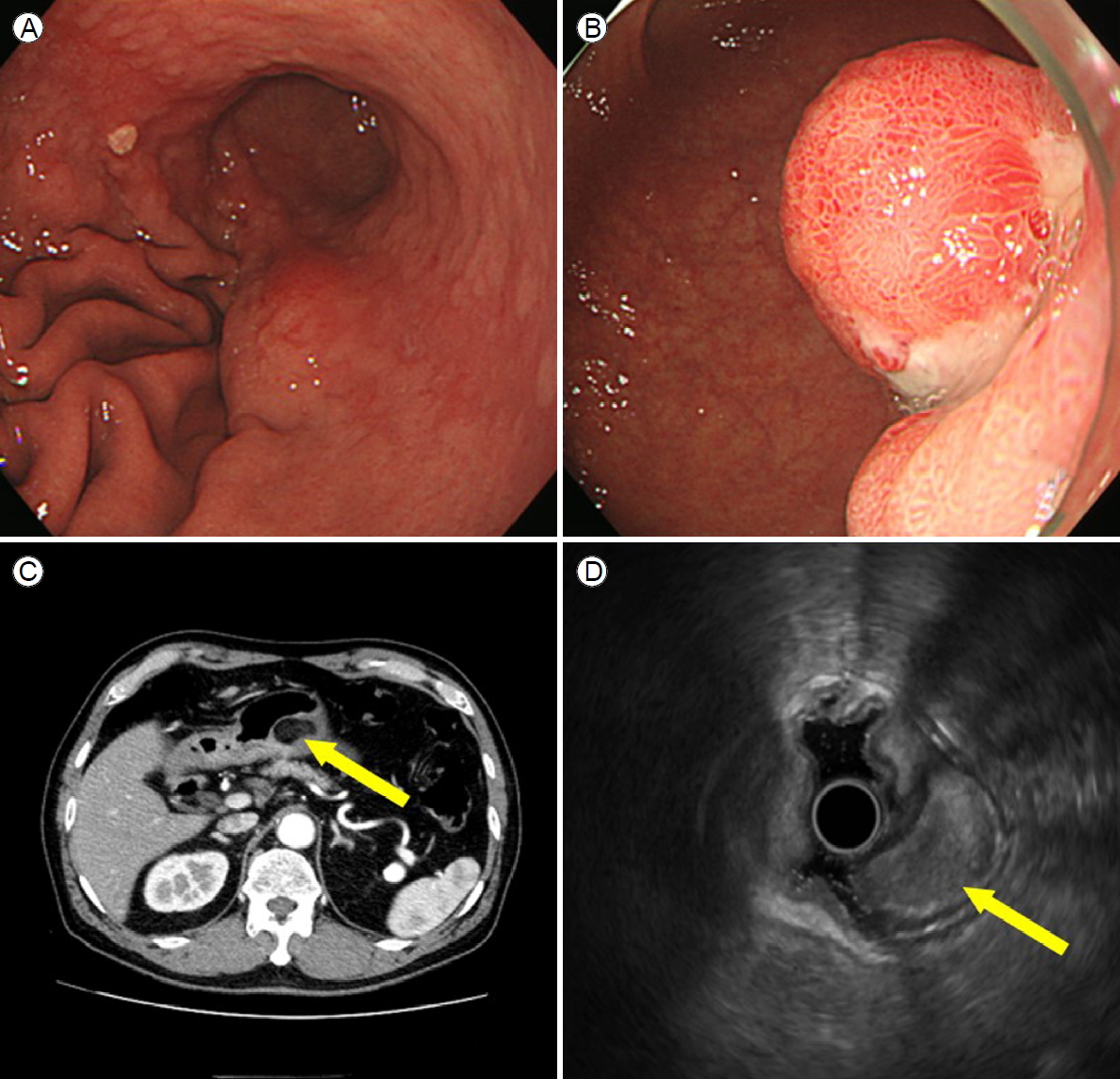
(A, B) Endoscopic findings. A subepithelial lesion measuring 3 cm with ulceration was detected on the basal area at the lower body posterior wall of the stomach. The ulcer was coated with whitish fibrin. (C) Computed tomographic (CT) findings (arrow). Postcontrast abdominal CT images showed a well circumscribed, smoothly margined, ovoid intramural mass of uniform fat attenuation arising from the great curvature of the antrum of the stomach with endoluminal extension. The mass measured approximately 3 cm. (D) Endoscopic ultrasound findings (arrow). Endoscopic ultrasound revealed a relatively echogenic mass measuring 28 × 17 mm seeming to arise from the gastric submucosa in the area of the gastric lesion, most consistent with benign lipoma.
내원 시 생체징후는 70/50 mmHg, 맥박 76회/분, 20회/분, 체온 36.3℃였고, 급성 병색이었다. 의식은 명료하였고 결막은 창백하였고, 공막에 황달은 없었다. 폐음과 심음은 정상이었으며, 복부 촉진에서 종괴는 만져지지 않았고 압통과 반발통은 없었고 직장수지 검사에서 흑색변이 관찰되었다.
내원 당시 검사실 소견으로는 말초 혈액 검사는 백혈구 11,340/mm3, 혈색소 13.1 g/dL, 혈소판 279,000/mm3였다. 생화학 검사에서 AST 26 IU/L, ALT 31 IU/L, ALP 77 IU/L, 총빌리루빈 1.7 mg/dL, 혈당 151 mg/dL, 총단백 7.0 g/dL, 알부민 3.9 g/dL, 혈액요소질소 31.0 mg/dL, 크레아티닌 0.97 mg/dL, Na 138 mEq/L, K 4.5 mEq/L, Cl 108 mEq/L, PT (INR) 1.02였고 요검사는 특이 소견 없었다.
응급 상부위장관 내시경을 시행하였고 위 내부에 대량의 혈괴와 음식물이 남아있었다. 위 하체부 후벽에 이전 내시경에서 관찰되던 점막하 종양이 색조는 적색조에 부드러운 경도를 보였으며 이동성과 pillow 징후, tenting 징후는 동반되지 않았으며 기저부에 궤양이 동반되어 있었고 활동성 출혈은 관찰되지 않았다(Fig. 1B). 전산화단층촬영(computed tomography, CT)에서도 활동성 출혈 소견은 관찰되지 않았으며 위 전정부에 3 cm 크기의 균일한 고음영을 보이는 종괴가 관찰되었다(Fig. 1C). 입원하여 수혈 및 양성자 펌프 차단제를 투여하며 경과 관찰하였고 더 이상 출혈이 없어 퇴원하였다.
7주 후 외래에서 상기 점막하 병변에 대하여 내시경 초음파 검사를 시행하였고 28 × 17 mm 크기의 3층 기원의 매끄러운 변연의 주변 구조와 구분되며 표면에 점막 결손은 없는 단단하고 균등음영과 고음영의 불균질 초음파 소견을 보이는 지방종으로 판단되었다(Fig. 1D). 재출혈의 위험을 낮추기 위해 1개월 후 내시경적 점막 절제술로 지방종 제거를 계획하였다.
퇴원 이후 경구 양성자 펌프 억제제를 복용하고 있었으나 15일 후 흑색변 발생하여 응급실에 다시 내원하였다. 내원 시 생체 징후는 혈압 110/70 mmHg, 맥박 96회/분, 20회/분, 체온 36.3℃였고 급성 병색이었다. 직장수지 검사에서 흑색 변이가 관찰되었고 비위관 세척에서는 오래된 혈괴가 관찰되었다. 내원 당시 검사실 소견으로는 말초 혈액 검사는 백혈구 7,870/mm3, 혈색소 9.9 g/dL, 혈소판 298,000/mm3였다. 당시 활동성 출혈 가능성을 배제하기 어려워 내시경적 평가를 권유하였으나 환자 및 보호자가 이미 알고 있는 병변에서 출혈이 있을 것이라며 추가적인 검사를 거절하였고 혈색소 감소에 대하여 수혈 및 양성자 펌프 차단제 투여 후 자의로 퇴원하였다.
이후 특이 소견은 없었고 1주 후 예정대로 입원하여 지방종에 대하여 내시경적 점막 절제술을 시행하였고 병리 조직학 검사에서 육안적 소견으로 3.0 × 2.6 × 1.8 cm의 크기로 상대적으로 잘 경계되며 음성 절제면을 가진 발육형 병변이었다(Fig. 2A, B). 광학 현미경 소견은 점막하 조직에서 성숙된 지방조직으로 구성된 종괴를 보여 지방종으로 진단되었다(Fig. 2C). 내시경적 점막 절제술로 지방종 제거 후 더 이상 출혈 소견이 없어 식사 개시 후 내원 4일째 퇴원하였다. 이후 증상의 재발은 없었으며 1년 후 추적 내시경 검사에서 절제술을 받은 부위는 궤양 반흔으로 잘 치유되어 있었다(Fig. 2D).
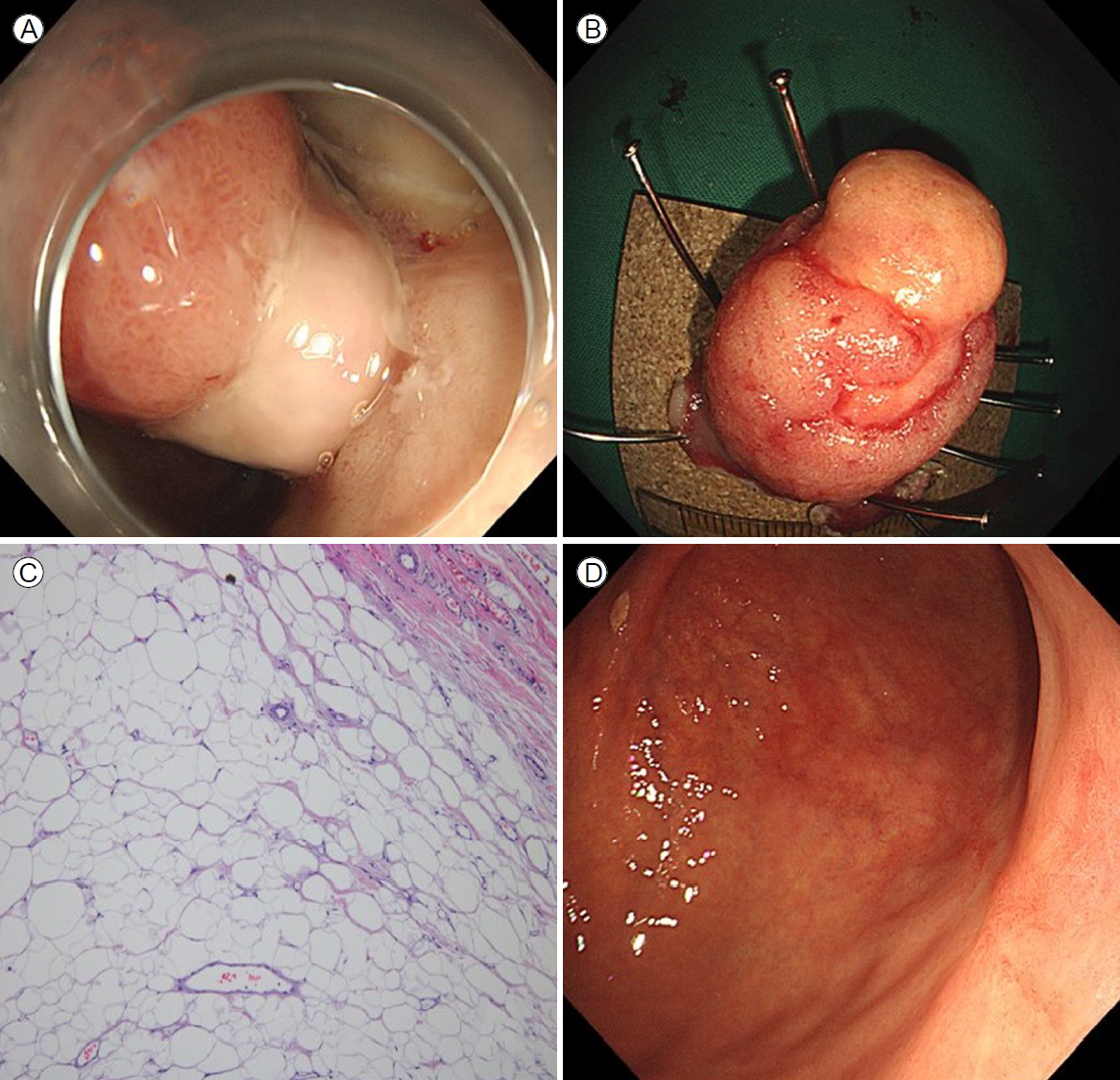
Endoscopic submucosal dissection of the tumor. (A) Endoscopic findings during endoscopic submucosal dissection. Endoscopic findings after submucosal injection. (B) Macroscopic view of the resected tumor. The tumor was well circumscribed and surrounded by a thick fibrous capsule. The tumor measured 2.5 × 1.5 cm. (C) Microscopic examination of the tumor showed mature adipose tissue with a clear resection margin (H&E, ×100). (D) Follow-up endoscopic findings showed a previous endoscopic submucosal dissection scar deformity on the antrum of the stomach. There was no evidence of local tumor recurrence.
고 찰
지방종의 원인은 명확하지 않으나 점막하에 발생학적으로 잘못 위치한 지방 조직에서 유래하는 양성종양으로 알려져 있다. 대부분 점막하 종양 형태로 발견되나 일부는 장막하 종양으로 발견되는 경우도 있으며[1] 독립적으로 1개 발생하는 경우가 대부분이나 10-15%에서는 다발성으로 발생하는 경우도 있다[16,17]. 지방종은 위장관 종양의 5%를 차지하며 주로 대장, 회장, 공장에서 흔히 발생하며, 위나 식도에서는 매우 드물게 발견된다[1,4,7,18]. 위의 지방종은 위의 양성 종양의 1% 미만을 차지한다[4,7,18]. 다른 위장관 지방종과 같이 대부분 독립적으로 단일성이며 점막하 종양의 형태이며 75% 이상이 위의 전정부에서 발견된다[4,7,19]. 대개의 지방종은 악성화 하지 않으나 조기 위암을 동반한 위 지방종의 증례 보고가 있어 추적 관찰 시 지방종의 크기가 크거나(> 3-4 cm) 상부위장관 출혈이 있거나 지방종에 궤양이 형성된 경우 주의가 필요하다[4,6,20-23].
대부분의 지방종은 무증상으로 상부위장관 내시경 검사에서 우연히 점막하 종양의 형태로 발견된다. 지방종의 크기가 2 cm 미만에서는 대개 무증상이나[4,18], 4 cm 이상에서는 75%에서 증상이 나타나며 주요 증상으로는 복통, 설사, 변비, 궤양, 장 중첩증, 장 폐색증, 출혈 등이 나타날 수 있다[1,2,4,7,10-15]. 본 증례에서는 3 cm 크기의 지방종에서 합병증이 발생하였다. 지방종 표면의 점막은 정상이지만 점막하 종괴로 인해 팽창되어 압박을 받으면서 괴사가 진행되어 궤양이 발생하고 출혈이 발생한다. 대개 만성 실혈로 인해 철 결핍성 빈혈로 나타나나 일부 심한 경우 간혹 응급 내시경 및 지혈술 또는 수술적 치료가 필요한 대량 출혈을 보일 수 있다[1,2,11]. 궤양은 종양의 크기가 클수록 발생 가능성이 높아지므로 증상 없이 우연히 상부위장관 내시경에서 발견된 위 지방종에서도 2 cm 이상의 크기를 보이는 경우 내시경적 혹은 수술적 절제를 고려할 수 있으며, 절제를 하지 않더라도 환자에게 출혈의 가능성에 대해 설명이 필요하다.
진단은 병력이나 신체 검사만으로는 어려우나 종괴가 매우 큰 경우 신체 진찰에서 상복부 종괴를 촉진하여 발견할 수 있으며 상부위장관 조영술, 복부 CT, 복부 자기공명영상촬영, 상부위장관 내시경, 내시경 초음파 등을 이용할 수 있다. 상부위장관 조영술에서 위장 내 원형의 충만 결손 또는 유경성 종괴를 보인다[1,3,6,11,20]. 복부 CT에서는 지방의 흡수 밀도인 -50 to -100 Hounsfield units를 보이는 주변 조직과 구별되는 종괴를 관찰할 수 있으나 크기가 작은 경우 진단이 안 될 수도 있다[1,3,6,11]. 상부위장관 내시경 상 넓은 기저부의 명확한 경계가 관찰되는 반구형 용종양 병변으로 흔히 관찰되며[5,10], 표면에는 둥글고 매끄럽고 용종의 첨부는 대개 황색조 또는 적색조를 띄고 기저부는 황색조를 띄며 점막에 혈관이 분포하는 양상으로 관찰된다. 또한 압박 시 압박흔이 보이는 pillow sign 또는 cushion sign, 겸자로 지방종 점막을 견인하였을 때 쉽게 당겨지는 tenting sign, 여러 번 생검을 같은 자리에 시행하여 점막 사이로 노출되는 지방조직이 관찰되는 naked fat sign 등을 이용하여 진단에 도움을 받을 수 있다[3,5,10]. 내시경 초음파 검사에서 지방종은 점막하층 즉, 제3층에서 균질한 고에코성 종괴로 관찰된다. 내시경 초음파는 내부 구조 파악에 도움이 되어 이소성 췌장이나 낭종과 같은 타 점막하 종양을 감별하는 데 도움이 된다. 조직 병리 검사에서는 성숙된 지방 조직이 명확한 경계를 보이는 점막하 조직이 관찰된다.
무증상의 크기가 작은 지방종은 치료 없이 경과 관찰할 수 있으나 악성 종양과 감별이 안되는 경우이거나 종괴의 크기가 크거나 출혈, 폐색 등 증상이 발생하는 경우에는 절제가 필요하다. 이때 내시경 초음파 검사에서 점막하에 국한되어 고유근층까지 침윤되지 않은 지방종의 경우 내시경적 점막 절제술을, 유경형인 경우 올가미 용종 절제술을 시도해 볼 수 있다. 내시경적 점막 절제술은 점막하종양의 제거에 86-95%에 달하는 성공률을 보인다[7]. 무경형이며 고유근층을 침범하거나 장막하 위치를 보이거나 4 cm 이상이면서 출혈 및 폐색 증상이 반복되는 경우 수술적 절제를 고려하게 된다.
본 증례는 재발성 대량 출혈을 보이는 위 지방종에 대하여 내시경적 점막 절제술로 치료한 예이다. 십이지장 지방종의 내시경적 절제술 치료는 드물게 보고되었지만, 위 지방종 출혈을 내시경적 점막 절제술로 치료한 증례는 매우 드물다[1,11,24]. 지방종이 증상을 유발하여 절제를 필요로 하는 지방종의 경우 비수술적 치료법으로 내시경적 점막 절제술을 적극적으로 고려해야 할 것으로 생각된다[7].
Acknowledgements
This study was supported by a 2020 research grant from Pusan National University Yangsan Hospital.