기능성 위장관질환에 있어서 식이 및 영양요법: 위식도역류질환
Diet and Nutritional Management in Functional Gastrointestinal Disorder: Gastroesophageal Reflux Disease
Article information
Trans Abstract
Gastroesophageal reflux disease (GERD) is a common condition with a wide range of clinical manifestations. The clinical epidemiology of GERD is related to diet. It has been speculated that certain dietary factors may play a role in the pathogenesis or course of GERD. Physiological studies have shown a decrease in lower esophageal pressure and an increase in esophageal acid exposure in response to consuming a variety of foods. Subjects with GERD are sensitive to acidic juices, such as orange and tomato juices. Some patients are less tolerant to caffeine including coffee. Fatty foods and chocolate may weaken the lower esophageal sphincter, whereas protein may increase lower sphincter tone. Large meals distend the stomach, increase intragastric pressure, and facilitate gastroesophageal reflux. Alcohol consumption is another important risk factor for GERD. However, a wide-ranging review of the available data revealed conflicting findings regarding the impact of dietary factors on GERD.
서 론
위식도역류질환(gastroesophageal reflux disease, GERD)은 위 내용물이 식도로 역류하여 불편한 증상을 유발하거나 이로 인하여 합병증을 유발하는 질환으로 가슴쓰림이나 신물이 넘어오는 것이 대표적인 증상이다. GERD는 환자의 삶의 질을 저하시키고, 식도염을 일으킬 수 있으며, 다른 여러 가지 합병증을 일으킬 수 있고, 호전과 악화를 반복하는 만성 경과를 보인다. 이러한 GERD는 서양에서는 비교적 흔하지만, 우리나라는 아직까지 서양에 비해서 낮은 빈도로 보고되고 있다. GERD의 치료는 현재 프로톤펌프억제제를 기본으로 한 약물요법이 근간을 이루고 약물요법에 반응하지 않는 일부 환자에서 수술 등이 적용되고 있다. 그 외 생활습관 개선과 식이조절 등이 보조적인 역할을 한다. 생활습관 개선이 GERD 치료에 미치는 영향은 다양한 인자가 상호복합적으로 작용하므로 모든 환자에게 일반화시키기 어렵다. 그러나 생활습관 개선이 GERD 환자의 일부에서는 증상의 호전 혹은 장기적인 증상 재발 방지에 도움을 줄 수 있다.
음식은 GERD를 포함한 상당수의 기능성 위장관질환에서 증상의 시작과 악화에 관여한다. 실제 기능성 위장관질환 환자들은 개인의 주관적 경험을 통해 스스로 특정 음식을 증상 유발인자로 인식해 회피하는 경향이 있다. 최근 매스컴을 통해 특정 음식과 소화기증상의 연관성 및 예방과 치료를 위한 식이 권고들이 넘쳐나고 있다. 그러나 실제 이를 규명할 수 있는 과학적인 근거는 빈약한 실정으로 식이요법은 약물 치료의 보조적인 역할로 권고되고 있다. 음식과 관련된 권고 내용에는 몇 가지 고려해야 할 점이 있다. 한 가지 음식이라도 여러 가지 영양 성분으로 구성되어 있으므로 주된 영양소 별 접근이 필요하다. 같은 주된 영양소를 가진 음식이라도 개인마다 섭취 양이나 속도, 조리 방법이 다를 수 있으므로 일률적인 제한은 적절하지 않을 수 있다. 본고에서는 GERD의 생활습관 중 식이에 관해 특정 음식과 GERD와의 연관성에 대해 알아보고 증상 완화와 악화에 영향을 주는 음식들에 대해 정리해 보고자 한다.
본 문
술
음주는 가스트린 자극을 통해 산분비를 증가시키고, 하부식도조임근(lower esophageal sphincter, LES)의 압력을 낮추고, 자발적인 LES 이완을 증가시키며 식도 연동과 위 배출운동성을 저해하여 GERD를 일으킬 수 있다[1]. 음주는 GERD 증상이 없는 건강한 사람에서 24시간 식도 산도가 정상이더라도 역류증상을 일으키고 식도 산도를 낮춘다[2-5]. 무작위 및 단면연구들에서 음주자들에서 역류증상의 유병률이 증가된다고 보고하였고[6-9], Wang 등[10]의 연구에서는 비음주자의 16%에서 역류증상이 있었고, 주당 210 g의 음주자의 43%에서 역류증상이 발생하였다(odds ratio, 2.85; 95% confidence interval, 1.67-4.49; p < 0.01). 그러나 대규모의 다국적 단면연구는 유사한 연관관계를 보이지 않았다[11]. 환자-대조군연구에서 GERD 증상이 있는 음주 환자를 대조군인 비음주자, GERD가 있는 환자 및 호두까기 식도(nutcracker esophagus)를 가진 환자와 비교하였을 때, 대부분의 음주자들은 6개월 이상 금주를 하였을 경우 식도 산도의 호전 없이도 고압성 LES(LES hypertension), 고진폭 식도 수축(high-amplitude esophageal contractions) 또는 비연동성 식도 수축(nonperistaltic esophageal contractions)이 호전되었다[12]. 따라서 금주가 산도나 GERD 증상에 직접 영향을 준다는 충분한 근거가 없더라도 금주 후에 식도운동성 이상은 호전되는 것으로 확인되었다.
커피와 카페인
산에 민감한 환자에게 커피 혹은 카페인 음료를 식도 내로 주입하였을 때 흉부작열감을 일으킨다고 알려져 있다[13]. 그러나, 두 개의 큰 역학 조사에서는 커피섭취와 GERD와는 연관이 없었고[10,11], 최근 노르웨이의 조사에서 커피섭취와 GERD는 상관관계가 없었다[14]. 몇몇 연구에서는 규칙적으로 디카페인 커피를 마셨을 경우 LES 압력이 증가하였고[15,16], 다른 연구에서는 GERD를 가진 환자에서 대조군과 비교하였을 때 역류 횟수, 총 역류시간, LES 압력에 영향을 주지 않았다[17]. 커피를 제조하는 과정, 로스팅 방법, 공정과정 등이 GERD 변수에 영향을 줄 수 있다는 연구결과가 있다[18-21]. 디카페인 커피를 섭취한 경우를 카페인 커피를 섭취한 경우와 비교하였을 때 일부 연구에서는 산분비가 유의하게 적었다[22]. Salmon 등[23]은 환자들이 커피에 노출되는지 여부에 따라 식후 LES 압력이 낮게 측정될 수 있어 식후에 커피를 자주 마시는 사람들의 경우는 커피와 GERD와의 상관관계에 혼동을 줄 수 있다고 주장했다. GERD 환자에서 금식이나 표준 시험식사를 했을 때 커피가 LES 압력을 낮춘다는 일부 보고도 있다[24]. 상충되는 결과를 감안할 때 카페인이나 커피와 GERD와의 연관성은 아직 명확하게 밝혀지지 않은 상태이다. 따라서, GERD 환자에서 커피나 카페인류를 통상적으로 제한하는 것은 명확한 근거가 없다.
신 과일과 주스
신 과일은 종종 흉부작열감을 일으킨다. 약 400명의 GERD 환자를 대상으로 한 설문조사에서 응답자의 72%가 오렌지나 포도주스를 섭취하였을 때 흉부작열감이 증가하였다[25]. 그러나 Price 등[13]은 산에 민감한 환자(bernstein 검사 결과 양성)에서 식도 내로 오렌지주스를 주입한 후 민감하게 반응했고, 심지어 오렌지주스가 pH 7로 조정되었을 때도 마찬가지였다는 결과를 감안하였을 때 GERD 환자에서 신 과일이 미치는 영향은 산도 때문만은 아니라고 주장하였다. Cranley 등[26]은 오렌지주스를 주입하였을 때 대조군은 LES 압력이 중가한 반면, GERD 환자에서는 LES 압력이 변하지 않았다고 보고하였다. 그러나 GERD에서 신 과일의 회피효과에 대한 연구는 아직까지 보고되지 않았다.
탄산음료
탄산음료가 GERD를 일으킨다는 가정 하에 여러 연구들이 진행되었다[27]. 한 연구에서는 다변량 분석을 통해 탄산음료섭취가 GERD 증상의 예측인자라고 보고하였다[28]. 건강인을 대상으로 한 작은 규모의 연구에서는 탄산수섭취, 카페인이 첨가된 콜라섭취 또는 디카페인 콜라를 섭취한 경우를 물을 섭취한 경우와 비교하였을 때 LES 압력이 동등하게 감소하였다[29]. 그러나 아직까지 탄산음료 중단효과에 대한 연구는 없다.
초콜렛
초콜렛은 자주 GERD의 자극인자로 언급된다. 초콜렛이 식도 산도와 LES에 영향을 준다는 근거는 제한적이다. 한 연구에서 초콜렛시럽 120 mL를 섭취하였을 때 LES 압력이 유의하게 낮아졌다(p < 0.01) [30]. Murphy and Castell [31]은 전형적인 GERD 증상을 가진 7명의 환자에서 검사용 음료(초콜렛과 동일한 삼투압과 칼로리)를 섭취한 경우와 비교하였을 때 초콜렛섭취를 한 경우에 산 분비시간이 유의하게 길었다고 보고하였다(p = 0.04). 그러나, GERD 증상에 대해 초콜렛을 제한하였을 때의 효과를 언급한 연구는 없다.
매운 음식
환자들은 자주 매운 음식을 먹었을 때 흉부작열감을 호소하지만 매운 음식섭취가 LES 압력이나 식도 산도에 영향을 준다고 보고한 연구 결과는 거의 없다. 한 연구에서는 GERD 환자의 경우 대조군과 비교하여 양파섭취로 인해 역류 횟수가 늘어나고(p < 0.01) 식도의 산 노출시간이 증가하였다(p < 0.05) [32]. 많은 환자들은 매운 음식이 자신의 GERD 증상을 악화시킨다고 믿지만 매운 음식을 회피했을 때 GERD 증상에 변화를 일으킨다고 보고는 없다.
기름진 음식
지방이 역류를 증가시킬 뿐만 아니라 식도에 산이 노출되었을 때 민감도를 높인다고 추측하고 있다. 무작위 임상시험에서 GERD를 가진 8명의 환자와 대조군 11명에서 식도 내로 염산을 주입한 후 위 내로 등장성 식염수와 20% 지방 용액을 주입하였을 때 지방 주입과 관련된 산에 대한 민감도와 증상에서는 유의한 차이가 없었다[33]. 두 개의 연구에서는 환자가 십이지장 내로 지방 용액과 등장성 식염수 중 어느 것을 주입했는지 여부와는 상관없이 흉부작열감 증상이나 산 주입에 의한 역류증상 발병까지의 시간이 유의하게 짧아졌다[34,35]. 따라서, 지방 주입이 LES 압력이나 일시적인 LES 이완에는 영향을 미치지 않는 것으로 생각된다. Nebel and Castell [36]은 건강인에서 동일한 열량을 가진 지방과 단백질 식사를 섭취한 후 LES의 반응을 평가한 결과, 단백질 식이를 한 경우에 LES 압력이 증가되었던 것에 비해 지방 식이를 한 경우에는 LES 압력이 유의하게 낮아졌다고 보고하였다. Becker 등[37]은 고지방 및 저지방 식이 후에 식도 산분비를 연구한 결과 지방량은 식도의 산도 이상과는 유의한 연관이 없다고 하였다. 20명의 건강인을 대상으로 한 연구에서 고지방 식이를 한 경우 저지방 식이를 한 경우에 비해 산분비가 유의하게 증가하였고, 많은 용량을 섭취한 환자들은 산분비가 증가하였다[38]. 다른 무작위 연구에서 고지방 식이를 한 경우와 저지방 식이를 한 경우를 비교하였을 때 LES 압력, 일시적인 LES 이완, 역류의 횟수, 식도 산분비 등에 차이가 없었다[39,40]. 지방 함량보다는 음식의 칼로리 함량에 따라 영향을 받는 지에 대한 논의는 여러 상반되는 연구 결과가 있다[39,41]. 앞서 언급한 연구를 바탕으로 식사의 지방 함량이 GERD 결과에 영향을 주는지에 대한 정보는 부족하다. 최근 연구에서도 GERD 환자의 식이에 지방을 제한하도록 하는 근거는 없다.
결 론
지금까지 GERD와 음식에 관련된 연구 결과들을 Table 1에 요약하였다. GERD의 병태생리는 음식 외에도 여러 인자의 복합적인 상호작용으로 이루어지므로 특정 음식의 일률적인 제한이나 권고는 아직까지 제한적이라고 할 수 있다. 음식은 여러 가지 영양소를 포함하고 있으므로 GERD의 식이요법은 주된 영양소에 따른 개별적인 접근이 필요하다. 최근 기능성 위장관질환에서 Fermentable Oligo-, Di-, Mono-saccharides And Polyols (FODMAP) 등 음식의 역할이 주목을 받기 시작하면서 과학적인 증거들이 축적되고 있으나, 대부분의 연구들이 서양인들을 대상으로 한 서양음식에 관한 내용으로 그대로 우리나라 진료에 적용시키기는 무리가 있다. 향후 한국인에 적합한 GERD의 식이요법에 대한 전향적 연구가 필요 하다.
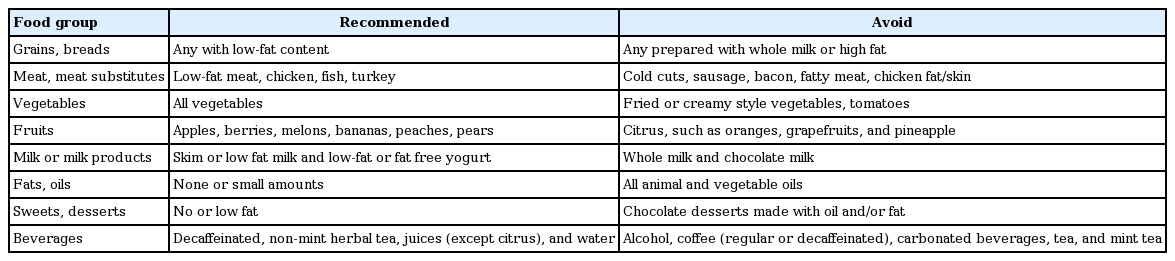
Dietary recommendations for patients with GERD