한국의 비심인성 흉통의 진단 및 치료의 고유한 특징
Distinct Characteristics of Noncardiac Chest Pain in Korea
Article information
Trans Abstract
Gastroesophageal reflux disease (GERD) is the most common cause of noncardiac chest pain (NCCP) and was reported to cause 41% of cases of NCCP in a recent study of Korea. Typical reflux symptoms were reported to be frequent in Korean patients suffering from NCCP. Therefore, a careful history of the symptoms is relatively indicative of GERD diagnosis in Korea. In Korea, contrasting Western countries, patients with NCCP but present no alarm features should undergo endoscopy to exclude gastric cancer or peptic ulcer. In a primary care setting, PPI test is sufficient for the presumptive diagnosis of GERD. Specifically in Korea, the optimal duration of PPI test may be at least 2 weeks because of less frequent or atypical GERD symptoms. In patients diagnosed with GERD-related NCCP, the initial long term therapy (more than 2 months) followed to the maintenance therapy is required to alleviate symptoms. Esophageal dysmotility is relatively uncommon, and pain modulators seem to offer significant improvement in chest pain control in non GERD-related NCCP. Unfortunately, the majority of traditionally available tricyclics or heterocyclics have many undesirable effects. Therefore, newer drugs with fewer side effects may be needed, such as the serotonin-norepinephrine reuptake inhibitors. (Korean J Med 2011;80:649-655)
서 론
흉통을 호소하는 환자들은 관상동맥 질환의 임상적 중요성 때문에 관상동맥조영술 및 운동부하검사 등을 통해 환자의 증상이 심인성인지의 여부를 먼저 평가받게 된다. 이러한 검사 결과 심장의 이상이 없이 반복적으로 흉통을 호소하는 경우를 비심인성 흉통(noncardiac chest pain, NCCP)이라 하며[1-3] 일반인에서 그 빈도가 약 30%까지 이르는 것으로 알려져 있다[3,4]. 이처럼 NCCP는 비교적 드물지 않게 접할 수 있는 임상증상이며 그 예후는 비교적 좋다[5]. 하지만 NCCP 환자는 지속적인 통증 및 불안감으로 인해 업무를 수행하지 못하거나, 일상생활에 지장을 받거나, 혹은 반복하여 병원을 찾는 것으로 알려져 있다[6]. 이들은 심장에 대한 검사를 실시하여 심장 질환에 의한 흉통이 배제되었음에도 불구하고 특별한 원인이 밝혀지지 않을 경우 흉통의 원인에 대해 상당히 불안감을 가지게 되며 따라서 필요 없는 의료 이용을 증가시켜 의료비를 상승시킨다. 그러므로 NCCP의 원인 및 그 기전을 밝히는 것이 매우 중요하다고 할 수 있다. 지속적인 NCCP를 호소하는 환자에서 흉통의 원인 질환을 규명해 줌으로써 환자는 심리적 불안을 덜고 적절한 치료를 통해 보다 안정된 생활을 영위할 수 있을 것이다[7,8].
NCCP를 일으키는 질환은 다양하며, 미세혈관 협심증, 근골격계 질환, 정신과적 질환, 종격동 및 늑막 질환, 결체 조직 질환, 그리고 담도 및 위장관 질환 등 여러 원인이 관여하며[9,10], 최근 그 원인으로 식도 질환이 중요시되고 있고 그중 위식도역류질환(gastroesophageal reflux disease, GERD)이 가장 흔한 원인으로 알려져 있다[1,11,12]. 최근 국내에서 시행된 전향적인 연구에 따르면 NCCP의 원인 중 약 40%가 GERD임이 보고되었고(Fig. 1) [13], 이와 같이 국내에서도 그 원인으로 GERD가 가장 중요하다고 할 수 있다. GERD 이외에 NCCP의 중요한 원인이 되는 식도 질환으로써 내장신경과민증, 식도운동질환 등이 비교적 빈번한 빈도를 차지한다.
Upper gastrointestinal evaluation. GERD-related NCCP was found in 24 (41%) of 58 subjects on EGD and/or ambulatory 24 h esophageal pH monitoring. Esophageal motility disorder was found in 24 subjects (41%) including 18 with ineffective esophageal motility, 4 with nutcracker esophagus, one with hypertensive LES, and one with achalasia. non GERD, non GERD-related NCCP; Hyper LES, hypertensive LES; Nutcracker, nutcracker esophagus; IEM, ineffective esophageal motility.
NCCP의 기전은 명확히 규명되어 있지 않다. 식도 질환에 의한 흉통은 식도가 심장과 공통 신경 지배를 받고 있어 위산, 펩신, 담즙 등이 식도를 자극할 때 식도 상피 세포에 있는 화학적 수용체가 자극되거나, 식도의 확장이나 경련 등에 의하여 물리적 자극 수용체의 자극, 혹은 온도 수용체를 통한 자극 등에 의해서도 일어난다고 알려져 있으며, 또한 통증에 대한 감각 역치가 저하되어 있는 과민성이 관련 있는 것으로 알려져 있다. 이외에 자율신경계, 위심장억제반사, 정신질환(공항장애, 불안, 우울증), 심리적인 요인 등이 흉통의 발생기전으로 지적되고 있다[1,14].
본고에서는 NCCP의 진단 및 치료를 위해 다양한 방법 및 고려해야 할 사항들에 대해 살펴보고 우리나라에서의 고유한 상황 및 특징을 토대로 하여 앞으로 나아가야 할 방향 등에 대해 그간의 경험과 자료를 중심으로 알아보고자 한다.
진 단
NCCP의 가장 흔한 원인 질환으로는 GERD를 들 수 있으며, 서양에서는 그 빈도가 60%에까지 이르는 것으로 보고되고 있다[15]. 한편, GERD와 관계없는 NCCP (non GERD-related NCCP) 환자 중 약 30-40%는 식도운동질환으로부터, 나머지는 식도의 통증의 과감각, 즉 내장 과민성으로부터 나타난다고 여겨진다. 따라서 NCCP의 식도관련 병태생리는 GERD, 식도운동질환 그리고 내장과감각으로 정리할 수 있다. 그러나 NCCP의 병태생리를 명확히 규명하여 임상적으로 적용하는 일은 쉽지 않다. 심장 질환에 의한 흉통이 배제된 NCCP 환자들에서 식도 질환의 가능성을 염두에 둘 때, 현재까지 잘 알려진 검사로는 상부위장관 내시경(esophagogastroduodenoscopy, EGD), 식도내압검사(manometry), 24시간 보행성 식도 pH 검사 및 프로톤펌프억제제(proton pump inhibitor, PPI)를 투여하고 증상의 변화를 관찰하는 PPI 검사가 있으나[16], NCCP의 원인 질환에 대한 gold standard는 없는 실정으로 그 상황에 따라 위의 검사들을 복합적으로 사용할 수 있다. 최근에는 다채널 강내 임피던스-pH 검사(multichannel intraluminal impedance-pH metry, MII-pH), 고해상도 식도내압검사(high resolution manometry, HRM) 등이 소개되어 임상에서 이용되고 있다.
비심인성 흉통과 전형적인 위식도역류질환 증상
NCCP 환자들이 호소하는 증상은 다양한 양상으로 나타날 수 있으며, 흉통 이외에 가슴쓰림(heartburn), 산역류(acid regurgitation) 증상 및 속쓰림, 소화 불량 등의 위장관 증상 외에 인두 불편감, 호흡 곤란 등의 다양한 형태로 나타날 수 있다. 따라서 그 증상에 대한 분석은 매우 중요하다고 할 수 있다. 전형적인 GERD 증상이라고 하면, heartburn과 acid regurgitation을 들 수 있으며, 서양 및 동양의 일부 연구 결과를 보면 그 증상과 원인 질환과의 연관성에 대해 이견이 있으며[12,15], 실제로 증상과 원인 질환과의 관계를 직접적으로 분석한 연구도 드문 실정이다. 저자 등은 NCCP 환자를 대상으로 설문지 및 인터뷰를 통해 그 증상의 양상에 따라 heartburn과 acid regurgitation등 전형적인 GERD 증상을 가지는 군과 그렇지 않은 군으로 나누었고, 두 증상군에서 EGD 와 24시간 식도 pH를 통해 진단된 GERD와 연관된 NCCP (GERD-related NCCP)의 예측도를 조사하였다. 그 결과 전형적인 GERD 증상을 가지는 군에서 GERD-related NCCP의 양성 예측도 및 민감도가 65-70%였다[13]. 이 연구는 이전에 보고되었던 증상과 그 원인 질환과의 연관성에 대한 여러 이견에 대해 국내에서 시행된 연구로서 NCCP 환자들이 호소하는 증상에 대한 분석의 중요성을 나타내었으며 우리 나라 현실에서 일차 의료기관에서도 NCCP 환자의 원인 질환을 예측하는 데 도움이 될 것으로 보인다.
비심인성 흉통 환자에서 상부위장관 내시경검사의 필요성
NCCP 환자의 EGD 결과에서 비정상적인 결과, 즉 역류성 식도염(reflux esophagitis)으로 진단되는 경우는 전세계적으로 약 5-35%로 비교적 낮게 보고되어 왔다[12,16-19]. 따라서 NCCP 환자에서 EGD의 진단적 역할에 대해 의문을 가지게 된다. 우리나라에서는 대체로 심장 질환에 의한 흉통이 배제된 환자들에 대해 EGD를 먼저 시행하는 경향이 있으나 서양의 guideline에서는 NCCP 환자 중 경고 증상이 있는 경우에만 EGD를 먼저 시행할 것을 권고하고 있다[14]. 최근 저자 등은 NCCP 환자의 EGD 결과, reflux esophagitis으로 진단되는 경우가 20%였고 그리 높지 않은 수치임에도 불구하고 EGD를 먼저 시행할 것을 권고하였다[13]. EGD는 식도 및 위, 십이지장의 구부를 육안적으로 직접 관찰할 수 있는 유일한 검사로서 reflux esophagitis 진단의 역할 이외에 그로 인한 합병증을 확인하고, 특히 위암이나 소화성 궤양 등 상부 위장관의 다른 병변을 감별하기 위하여 필요한 검사이다[20]. 따라서 위암이나 소화성 궤양 등의 빈도가 높은 우리나라에서는 경고 증상이 없는 경우라 하더라도, EGD는 필요한 검사라고 할 수 있다.
비심인성 흉통에서 PPI 검사의 기간은 1주로 충분한가?
PPI 검사는 강력한 위산분비 억제제인 PPI를 투여하고 증상의 변화를 관찰하는 방법으로서 현재 서양에서는 GERD 진단에 있어서 일차적으로 사용되고 있는 경향이다. PPI 검사는 간편하고, 비침습적이며, 비용이 절감되고, 민감도가 높으며, 치료 효과의 예측이 직접 가능하다. 반면에 특이도가 낮고, 결과 해석이 통일되지 않는 등의 단점도 가지고 있어 일부 보고에서는 그 진단적 가치가 과장되었다고 평가하기도 하지만, 최근 보고된 메타 분석 등을 통해 보았을 때 역시 PPI 검사는 현재로서는 GERD 및 NCCP의 일차적인 진단 방법으로 인정되는 추세이다(Table 1) [21,22]. PPI 검사의 이론적 근거를 살펴보면, 위산은 GERD의 증상 유발에 주된 작용을 하며 PPI는 강한 위산 분비 억제 작용을 한다[23]. 따라서 PPI는 GERD의 증상 호전에 탁월한 효과를 보이고, 부작용이 거의 없고 안전한 것으로 알려져 있다. PPI 검사에서 PPI 투여 용량은 보통 치료 용량의 두 배가 고려되나, PPI 검사의 적정 기간에 대해서는 다소 이견이 있다[24,25].
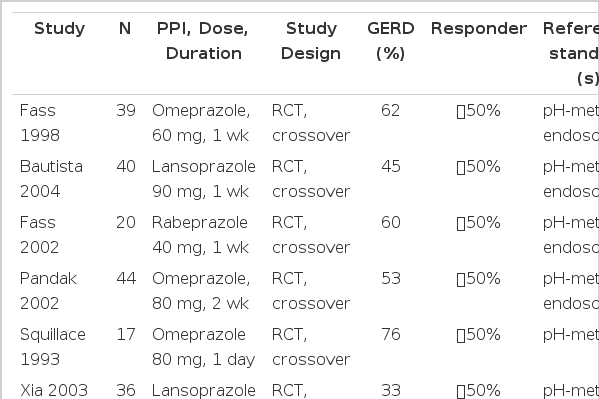
PPI test performance summaries in noncardiac chest pain
Fass 등은 NCCP 환자를 대상으로 한 이중맹검 연구에서 PPI 검사의 진단적 유용성을 처음 보고하였는데, PPI 투여 후 증상 호전에서 위약군과 확연한 차이를 보여 민감도와 특이도가 각각 78.3%, 85.7%로 높았다고 보고하였으며 PPI 투여기간으로는 7일이면 충분하다고 하였다[16]. 그 이후로 많은 연구에서 PPI 검사의 유용성이 입증되어 왔으며[21, 26-29], 국내에서도 Jung 등이 다기관연구를 통해 PPI 검사가 전형적인 증상을 가지는 GERD에 대해 79%의 민감도를 나타낸다고 보고하였다[30].
최근 저자 등은 EGD와 24시간 식도 pH 검사를 통해 GERD-related NCCP로 진단된 환자를 예측함에 있어서 PPI 검사가 83%의 민감도를 보였고, 따라서 국내에서도 NCCP의 진단에 PPI 검사가 유용함을 입증하였다. 하지만 우리나라의 경우, 일반적으로 비전형적인 증상이 동반되는 경우가 흔하고, NCCP의 빈도가 서양만큼 빈번하지 않는 점 등을 고려하여[31-33], 서양과는 달리, 7일로는 충분하지 않고 14일의 기간이 적정함을 보고하였다(Figs. 2 and 3) [34].
A comparison of PPI test between GERD-related NCCP and non GERD-related NCCP groups. During the second week of the PPI trial (B), the percent of positive PPI tests was significantly higher in GERD-related NCCP group (81%) than non GERD-related NCCP group (27%) (p = 0.001). However, during the first week of the PPI trial (A), there was no significant difference between the two groups (GERD vs. non GERD = 50% vs. 23%, p = 0.1).
Receiver operating characteristics (ROC) curve of PPI test for GERD-related NCCP during the first week (A) and the second week (B). The reduction in chest pain corresponded to 0.78 in the area under ROC with an accuracy of 77.1% during the second week of PPI test. Additionally, there was significant difference between the areas under ROC curves of the first and second week of PPI test (p < 0.05).
다른 검사들의 임상적 유용성
식도내압검사
GERD에서 하부식도괄약근(lower esophageal sphincter, LES)의 역할이 매우 중요하며, GERD와 비효과적 식도운동(ineffective esophageal motility)이 직접적 또는 간접적으로 연관 관계가 있다는 것이 알려져 있으나, GERD를 진단함에 있어서 단독으로 LES 압력을 측정하는 것에 진단적 의의를 부여할 수는 없다. 서양의 보고에 의하면 식도운동질환이 NCCP 환자의 30%까지 차지한다는 보고가 있으나 동양에서 그 비율은 보다 낮은 것으로 여겨진다[13]. American Gastroenterological Association guideline에 보면 NCCP 환자에서 처음 시행해야 할 검사로 manometry를 배제하고 있다[2,35]. 최근 HRM이 등장하였고, achalasia나 diffuse esophageal spasm 등 원발성 식도운동질환을 평가하는 데 있어서 기존의 manometry보다 유용함이 보고되고 있으나, NCCP의 진단에 있어서는 향후 더 많은 연구가 필요하다.
24시간 보행성 식도 pH 검사
EGD에서 reflux esophagitis를 보이지 않는 위식도역류의 진단에 널리 사용되고 있는 검사 방법으로 24시간 보행성 식도 pH 검사가 있다. 그 동안의 연구 결과 이 검사는 재현성이 있다고 확인되었고, 컴퓨터를 이용해 위식도역류에 대한 여러 정량 분석이 가능하기 때문에 GERD의 진단에서 유용한 검사로 여겨졌다[36,37]. 그러나 이 검사는 환자에게 불편감을 주고 비용효과적이지 않아 1차 의료 기관에서는 거의 이용되기가 어렵다. 한편, 위음성의 결과가 나오는 경우도 드물지 않으며, 양성으로 나오더라도 그것은 증상과의 연관성을 의미할 뿐 인과 관계를 증명할 수는 없다는 한계점이 있다. 따라서 현재는 그 유용성이 떨어진다고 할 수 있다[1,38].
다채널 강내 임피던스-pH 검사
산의 역류를 측정하기 위한 24시간 보행성 식도 pH 검사는 식도가 위산에 노출된 정도를 평가할 수 있고, 실제 산의 역류를 찾아낼 수 있으며, 식도의 산청소능을 간접적으로 평가할 수 있다. 하지만 실제로 비전형적 증상 및 비미란성 위식도역류질환(nonerosive reflux disease, NERD)을 진단할 때 24시간 보행성 식도 pH 검사는 그 민감도가 낮을 뿐만 아니라 약산 또는 비산 역류 및 역류 중 재역류를 찾아낼 수 없다. 최근 개발된 MII-pH는 여러 개로 구성된 전극 중에서 각각 두 전극 사이에 전류를 보내서 저항변화에 기초한 통과물의 성질을 측정하고, 물질의 이동을 감지할 수 있는 임피던스의 성질과 산도를 결정하는 pH 검사의 조합으로 식도의 음식물 통과와 역류의 성상을 더욱 세분화하여 분석할 수 있도록 고안되었다. 즉 산, 약산, 비산 역류나 재역류를 감별할 수 있고, 기체상이나 액체상 등 역류된 물질의 성상까지도 구분할 수 있다[39,40]. 최근 Kim 등의 국내 연구는 MII-pH를 통해 NCCP의 진단률을 향상시킬 수 있다고 보고한 바 있다[41].
치 료
NCCP의 가장 흔한 원인은 GERD이며 따라서 이에 대한 치료는 위산분비 억제제이다. 한편, non GERD-related NCCP의 경우 식도운동질환 및 내장감각과민성을 고려해야 한다.
GERD-related NCCP의 경우 PPI가 일차 선택 약제이다. GERD-related NCCP에서 적절한 치료 효과를 보려면 PPI를 2개월 이상 투여하여야 하며, 초치료 후 유지 요법이 필요하다. 제산제와 H2 수용체 길항제는 효과가 떨어지며, PPI로 초치료에 성공한 경우라도 H2 수용체 길항제로 step-down 치료를 하면 증상이 재발하기 쉽다[42-44].
Non GERD-related NCCP 중 식도운동질환에 대한 치료로는 평활근 수축을 조절하는 약물 등이 제시되어지나 그 효과에 대한 연구 보고는 드물며, 내장과감각의 조절 등을 위해 trycyclic antidepressants (TCA), trazodone 그리고 serotonin uptake inhibitors (SSRIs) 등이 사용될 수 있는 것으로 보고되고 있다[45,46]. 최근 저자 등은 기능적인 heartburn을 가진 젊은 연령의 환자에서 새로운 정신작용약제인 selective serotonin- norepinephrine reuptake inhibitor (SNRI)와 위약의 효과를 비교하는 전향적 이중 맹검 연구를 시행하였고, SNRI가 효과적임을 보고하였다[47]. SNRI는 기존에 사용되던 약제에 비해 부작용이 거의 없는 약제로써, non GERD-related NCCP 뿐만 아니라, 기능성 위장관 질환에 있어서 향후 치료 전략을 세우는 데 도움이 될 것으로 여겨진다.
맺음말: 우리나라에서의 비심인성 흉통
NCCP는 서양뿐만 아니라 동양에서도 비교적 흔한 질환으로서, 삶의 질이 의미있게 저하된다. 그러므로 이에 대해서 올바르게 이해하는 것은 매우 중요하다. NCCP는 우리나라에서도 흔한 질환임에도 불구하고 아직까지 우리의 현실에 맞는 진단 및 치료에 대한 지침이 없이, 단지 서양의 진단 및 치료의 기준이 도입되어 있는 현실로써, 이를 그대로 적용하기 어려운 경우가 있다. 따라서 보고된 문헌들에 따른 객관적 사실에 근거하여 우리나라의 현실에 맞는 NCCP의 진단 및 치료에 대해 다음과 같은 기준을 제시해 본다(Fig. 4).
Proposed diagnostic evaluation of patients with NCCP in Korea.
첫째, NCCP의 원인 중 GERD가 가장 흔하며 따라서 GERD의 전형적인 증상인 heartburn과 acid regurgitation 및 비전형적인 증상에 대해서도 신뢰성이 높은 설문지 및 적극적인 인터뷰를 통해 증상에 대한 분석이 필요하다. 둘째, 위암이나 소화성 궤양 등의 빈도가 높은 우리나라에서는 경고 증상이 없는 경우라 하더라도, 소수의 예외를 제외한 대부분의 환자에서 먼저 EGD를 시행한다. 셋째, EGD에서 이상이 없는 경우 PPI 검사를 시행하되, 치료 용량의 두 배 용량을 투여하며, 그 적정기간은 서양과는 달리 2주로 한다. 넷째, 24시간 식도 pH 검사 및 manometry는 일차적인 진단검사로써보다는 적응증이 되는 경우에 제한적으로 이용한다. 다섯째, NCCP의 치료로써 GERD-related NCCP에는 PPI를 non GERD- related NCCP에서는 식도운동질환이 배제된다면 새로운 정신작용약제인 SNRI를 고려해 볼 수 있다.