간문부 담관암: 영상의학적 진단의 최신 지견
Hilar Cholangiocarcinoma: Recent update of radiologic assessment
Article information
Trans Abstract
Hilar cholangiocarcinoma is an adenocarcinoma of the bile duct arising from the large bile ducts near the hepatic hilum. In this manuscript, radiologic findings and preoperative assessment techniques are described according to morphologic classification proposed by Liver cancer study group of Japan. Also, pros and cons of each imaging modalities are discussed. (Korean J Med 79:605-612, 2010)
서 론
담관암(cholangiocarcinoma)은 담관 상피세포에서 기원하는 선암(adenocarcinoma)으로 간세포암에 이어 간에서 발생하는 두 번째로 흔한 원발암이다1). 담관암은 간내담관암과 간외담관암으로 분류되며 이 중 간내담관암은 다시 주변부담관암과 간문부 담관암으로 나눠진다. 주변부담관암과 간문부담관암은 종괴가 어디에서부터 시작되었는지에 따라 구분하며 그 기준은 간내담관 2차 분지부이다. 그러나 간내담관 2차 분지부 근처 담관의 어느 한 곳에서 발생하여 양쪽에 걸쳐 있는 종괴의 경우 앞서의 두 담관암 중 어느 쪽인지 명확하게 밝히지 못할 수 있다. 마찬가지로 총간관 분지부나 좌우간내담관 1차 분지에서 발생하는 간문부 담관암도 간외담관암과 명확하게 구분되지 않는 경우가 종종 있다.
발생빈도를 보면 주변부담관암이 전체 담관암의 10%를 차지하며 간문부 담관암은 25%, 간외담관암은 65%를 차지한다2). 형태학적으로는 다양한 분류가 사용되는데, 일본간암연구회(Liver Cancer Study Group of Japan)에서는 종괴의 성장 특성에 따라 종괴형성형(mass-forming type), 담관내 발육형(intraductal-growing type), 담관주위 침윤형(periductal-infiltrating type)으로 구분하는 분류법을 제안했다(그림 1)3). 이들이 제시한 분류는 종괴의 육안 소견, 성장 양상, 생물학적 행태, 환자의 예후 등과 잘 일치하며 영상의학 소견에도 잘 부합하여 가장 합리적인 분류법으로 여겨지고 있다.
Drawings illustrate various types of intrahepatic cholangiocarcinoma as classified by the Liver Cancer Study Group of Japan. (A) Mass-forming intrahepatic cholangiocarcinoma manifests as a round mass with a distinct border in the liver parenchyma. (B) Periductal infiltrating intrahepatic cholangiocarcinoma is characterized by tumor infiltration along the bile duct (arrow). It occasionally involves the surrounding blood vessels or hepatic parenchyma. (C) Intraductal intrahepatic cholangiocarcinoma is characterized by papillary or granular growth within the bile duct lumen. It occasionally demonstrates superficial extension (right arrow) or forms a tumor thrombus in an obstructed duct (left arrow). More than one type of cholangiocarcinoma may manifest in a single patient. In such cases, all of the types involved should be recorded (eg, “periductal infiltrating intraductal”) (reprinted from 8).
담관암의 영상 진단에는 주로 횡단면 영상 기법인 초음파, 전산화 단층촬영(computed tomography, CT), 자기공명영상(Magnetic resonance imaging, MRI) 등이 사용되고 있으며 침습적 방법으로 경피경간담관조영술, 내시경적 역행성 췌담도조영술(Endoscopic retrograde cholangiopancreaticography, ERCP), 수술 중 담관조영술이 사용된다. 일반적으로 초음파는 일차적인 선별검사로 사용되며, CT와 MRI가 병기결정을 위한 검사로 사용된다. 담도조영술은 중재적 시술을 위한 검사 또는 수술 전 정확한 담도의 침범 범위의 판정을 위하여 사용된다.
간문부 담관암은 정의상 간내담관암의 일부로 분류되고 있지만 그 임상양상이나 방사선학적 소견, 수술적 치료방법 등은 간외담관암과 좀더 유사한 양상을 보여 일부 교과서에서는 이 두 질환을 ‘대담관암(large duct cancer)’ 혹은 ‘담관암종(carcinoma of the bile duct)’ 등으로 묶어 기술하기도 한다. 간문부 담관암은 주담관에서 발생하는 악성 종양의 50% 이상을 차지한다. 주담관암의 약 17%와 18%에서 각각 중간 및 원위부 총담관을 침범하며 약 7%에서 미만성 종양침윤을 보인다4-6).
간문부 담관암은 간내담도 분지의 침윤 정도에 따라 Bismuth I형에서 IV형까지 분류한다. I형은 좌, 우담관 합류부의 폐쇄가 없는 형태, II형은 합류부에 폐쇄가 국한되어 있고 2차 분지 이하의 침범이 없는 형태, III형은 합류부의 폐쇄가 있고, 좌, 우 담관분지 중 한 쪽의 2차 분지 이상이 침범된 형태로 우측 침범이면 IIIa형, 좌측 침범이면 IIIb형이다. IV형은 양측 모두 2차 분지 이상이 침범된 형태이다(그림 2). 간내담관암과 마찬가지로 자라는 모양에 따라 종괴 형성형, 주변부 침윤형 및 담관내 발육형의 세 가지로 구분하나 이 세 가지 기본 형태에 다른 형태가 공존하는 복합형 combined을 덧붙여서 분류하기도 한다7,8).
Types of hepatic duct obstruction caused by hilar cholangiocarcinoma. Type I is a nonobstructed primary confluence; type II, obstruction limited to the primary confluence; type III, an obstructed primary confluence with extension to the right (type IIIa) or left (type IIIb) secondary confluence; and type IV, an obstructed secondary confluence of both the right and left hepatic ducts. (Adapted and reprinted, with permission, from reference 7.)
종괴형성형 간문부 담관암
종괴형성형 간문부 담관암은 같은 타입의 주변부담관암의 소견과 유사하게 주변부 테두리가 조영증강된 큰 저음영 종괴로 보이며, 간문부 담도의 폐쇄가 동반되어 있다는 점에서 주변부 담관암과 구별된다. 간혹 종괴가 간문부에서 자랐는지 아니면 주변부담관암이 이차적으로 간문부를 침범하여 폐쇄시킨 것인지를 정확하게 감별하는 것이 쉽지 않거나 불가능한 경우도 있다(그림 3)8).

Exophytic hilar cholangiocarcinoma. Arterial (A) and portal-phase (B) computed tompgraphy (CT) scans show a 4-cm low-attenuation mass with peripheral enhancement at the hepatic hilum, mainly in segment IV. Both intrahepatic ducts are dilated. Two pigtail catheters were inserted for drainage. (C) Cholangiogram reveals obliteration of the hilar ducts. In such case, it is difficult to ascertain whether the tumor originates from the left hepatic duct and demonstrates exophytic growth or originates from a small branch of segment 4 and exhibits subsequent involvement of the hepatic hilum (reprinted from reference 8).
담관내 발육형 간문부 담관암
담관내 발육형 간문부 담관암은 주위 간실질에 비해 저음영을 가진 담관내 연조직성 종괴로 보인다(그림 4)9). 종양은 흔히 담관계 내에 다발성 혹은 파종성으로 존재하며 양측 간내담관이나 간외담관을 동시에 침범하기도 한다. 육안적으로 관찰되는 것보다 현미경 소견상 병변의 침범부위가 훨씬 큰 경우가 흔하므로 수술 전 병기결정 시 담도내시경 등을 이용한 적극적인 종양범위 판정이 필요하다. 병변의 위치에 따라 발현 증상이 결정되는데, 주담관에 위치하면 황달이, 간내담관에 위치하면 우연히 발견된 분절성 담관 확장이 나타난다.
Polypoid hilar cholangiocarcinoma. (A, B) Delayed- phase computed tompgraphy (CT) scans (B obtained at a lower level than A) show a soft-tissue mass (arrow) within a dilated left hepatic duct and common bile duct. (C) Cholangiogram shows a polypoid mass at the confluence level (arrows) (reprinted from reference 8).
ERCP 및 경피경간담관조영술에서는 늘어난 담관내 혹은 담관벽을 따라 유두상 종괴가 불규칙하고, 톱니바퀴 같은 변연을 가진 충만결손으로 나타난다9,10). 최근 담관 내에서 유두상으로 성장하는 종양 중 풍부한 점액 분비가 특징인 변이종, 즉 담관내 유두상 점액종양 intraductal papillary mucinous tumor (IPMT) of the bile duct에 대한 관심이 높아지고 있다. 이 질환은 내시경으로 십이지장 유두의 벌어진 입구를 통해 분비되는 점액을 확인함으로써 진단할 수 있는데, 이 종양은 병리학적 소견, 다량의 점액 분비, 병태생리학적 특성면에서 췌장의 관내 유두상 점액종양과 유사성이 많고, 종괴의 근위부 및 원위부 담관이 모두 심하게 늘어난다. 초음파와 CT에서 점액은 각각 무에코나 물과 같은 정도의 음영을 보여 담즙과 구별되지 않는 게 보통이다. 종괴 자체는 보이지 않거나 초음파성 고에코나 CT상 저음영의 작은 병변으로 보일 수도 있다(그림 5)9-11).
Intraductal papillary mucinous tumor of the bile duct. (A) computed tomography (CT) shows a small papillary tumor in the cystic duct (arrow). (B) Distal common duct is dilated without definite obstructing cause. The patient complained of recurrent right upper quadrant pain and fever. (C) endoscopic retrograde cholangio pancreatography (ERCP) shows amourphous filling defect in distal common duct, suggesting intraductal mucin. Segmental resection of mid common duct revealed papillary adenocarcinoma in the cystic duct.
담관주위 침윤형 간문부 담관암
담관주위 침윤형은 총 간문부 담관암의 70% 이상을 차지하는 가장 흔한 타입이다. 병리학적으로 암조직이 담관벽을 따라 침윤성으로 증식함에 따라 담관벽이 두꺼워지고 담관이 완전 폐쇄되며 주위 혈관이나 간실질을 침범한다.
초음파에서 좌우 간내담관의 확장이 보이며 간문부에서 확장된 좌우담관은 서로 합류되지 않고 분리되어 보인다. 회색조 영상만으로는 종괴 자체를 보기 힘들 수 있으나 미세기포 조영제를 이용한 조영증강 영상에서는 종괴 자체뿐 아니라 근위부 경계와 간실질 침범 등 종양의 범위와 주변 위성 결절 등을 더 잘 보여줌으로써 술전 병기 결정에 도움을 줄 수도 있다12). 조영증강 CT에서 담관주위 침윤형 종괴는 담관을 폐쇄시키는 국소적 담관비후의 형태로 나타나며 동맥기에는 고음영을 보이는 경우가 많고 문맥기에도 등음영 혹은 고음영을 보여 대략 80% 이상에서 동맥기 또는 문맥기에 주변 간실질보다 높은 조영증강을 보인다(그림 6)7,8). 폐쇄 위치와 담관 침범 범위의 정확한 평가는 좌우담관의 2차 합류부를 얼마나 정확히 확인할 수 있느냐에 달려 있다. 초기나선CT는 약 60%의 정확도를 보인다고 보고되었으나 보다 발전된 MDCT와 담도조영술을 혼합하면 84%에서 정확한 진단이 가능하다7,8,13).
Infiltrating hilar cholangiocarcinoma with tumoral involvement of the right secondary confluence and common hepatic duct. (A) CT scan reveals a high-attenuation tumor on the anterior aspect of the right portal vein (arrowheads). (B) On a subsequent computed tomography (CT) scan, the tumor appears as a high-attenuation lesion on the right side of the portal vein (arrowheads). (C, D) CT scans (D obtained at a lower level than C) show the mucosa of the cystic duct with strong enhancement (open arrow), a finding that suggests tumoral involvement. Soft tissue infiltration around the portal vein (arrowheads) and lymphadenopathy (solid arrow) are also noted (reprinted from 8).
담관암의 혈관 침범은 종괴와 혈관 사이의 지방층이 유지되느냐, 혈관 주위에 연부조직 음영이 존재하느냐, 그리고 역동적 CT상 보상성 혈류증가 소견이 있느냐로 진단한다(그림 7). CT는 혈관침범을 예측하는데 비교적 정확하고 유용하여 동맥 및 문맥침범을 모두 90% 이상의 정확도로 판정할 수 있다13,14). 간문부 담관암의 수술적 절제가능성은 혈관침범과 담도침범의 정도에 따라 예측한다. 통상적으로 절제 불가능한 간문부 담관암은 Bismuth IV형 담도침범, 주문맥 또는 고유간동맥 침범, 한쪽의 혈관침범과 반대쪽 담도의 2차분지 이상 침범, 한쪽의 간엽 위축과 동반된 반대측 담도의 2차분지 침범이나 혈관침범 등이 있다. 최근에는 간문부에서 담도나 혈관분지의 정상변이가 매우 많은 점, 또 수술기법이 발전되어 혈관침범시 절제 후 문합(resection and anstomosis)이 가능한 경우가 증가함 감안하여 간문부에서부터 2 cm 이내의 담도침범이나 2 cm 길이 미만의 혈관침범은 절제가능한 암으로 분류한다(표 1)13).

Hepatic arterial invasion is seen as a soft tissue infiltration around the right hepatic artery (arrows).
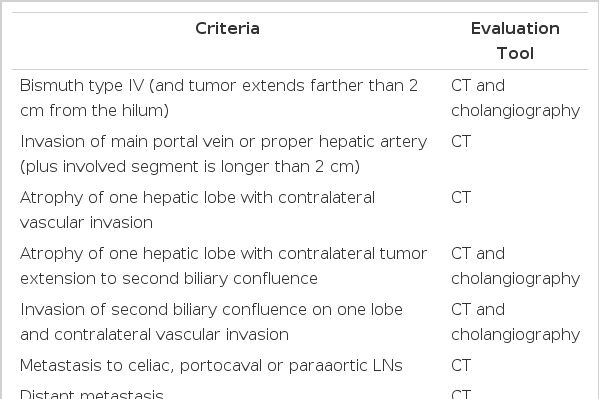
Criteria for unresectability of hilar cholangiocarcinoma (modified from reference 13)
MRI에서 종양은 CT와 비슷하게 동맥기에 고신호강도, 문맥기에 등신호강도 혹은 고신호강도의 조영증강을 보인다. MRCP의 주 소견은 담관의 연결성이 소실되거나 담관 폐쇄, 급격하고 불규칙적인 담관 내경의 감소와 상부 담관의 확장, 담관내 불규칙한 모양의 충만결손 등이다(그림 8). 종양의 담관내 침범 범위 결정에서 MR과 MRCP는 CT 및 담관조영술과 유사하게 85% 이상의 진단 정확도를 보인다14,15). 담관암의 병기결정에 있어 담관주위 침윤형은 담관내 발육형보다 높은 일치율을 보인다16). 이는 담관내 발육형 종양은 다발성이며 점막을 따라 표재성으로 파급되어 병변들 사이사이에 정상 점막이 끼어 있는 양상을 보이기 때문에 병변의 정확한 범위 파악이 힘든데 기인한다. 이처럼 MRCP의 진단정확도는 매우 높으며, 기기의 발전에 따라 검사시간이 단축되고 고해상도의 영상 획득이 가능해짐에 따라 진단적 담관조영술을 대신하고 있다. 침습적인 고식적 담췌관조영술과 비교한 MRCP의 장점은 비침습적이며 조영제 주입이 필요없어 합병증이 전혀 없다는 점, 주담관과의 연결성이 없는 담관도 관찰할 수 있어 소위 ‘missing duct’를 잘 평가할 수 있다는 점, 직접담도조영술에서는 얻을 수 없는 다양한 각도에서 담도 관찰이 가능하다는 점, 고식적 MRI와 같이 시행하여 담관 주위로의 병변의 파급, 예를 들면 혈관 침범, 림프절 비대 등을 동시에 평가할 수 있다는 점 등 이다. 이에 따라 MR은 ‘one-stop service’로서 그 사용이 늘어나고 있다. 그러나 MR은 고해상도 영상이 가능한 기기나 이를 판독할 수 있는 전문인력이 제한적이며, 또 영상획득 범위가 상복부만으로 제한됨에 따라 복강내 다른 부분에 대한 정보가 제한적이라는 단점을 가지고 있다.
A 66-year-old man with Bismuth type IIIb hilar cholangiocarcinoma. (A) Coronal thick slab T2W TSE MRC (T2 weighted turbo spin echo magnetic resonance cholangiogram) image shows separation of the left secondary branches of the intrahepatic duct, suggesting involvement of the left secondary confluence (arrows). (B) Gadolinium-enhanced T1W (T1 Weighted) image shows a mass as a focal enhancement of the thickened ductal wall at the right intrahepatic duct (arrowheads). (C) Axial thin slab T2W HASTE MR (T2 weighted Half-fourier acquisition single shot turbo spin echo magnetic resonance) image shows dilatation of the bile duct (arrows). Mass is not clearly demonstrated inT2 weighted images (reprinted from 15).
결 론
결론적으로 간문부 담관암은 육안적 소견에 따라 종괴형성형, 담관내 발육형, 주변부 침윤형의 세 가지로 분류할 수 있으며, MDCT와 담도조영술의 조합 또는 MRI와 MRCP의 조합에 의하여 비교적 정확한 진단과 절제 가능성을 예측할 수 있다. 그러나 일부 담도암에서는 육안적 소견으로도 식별하기 어려운 표재성 파급을 동반하여 정확한 병변의 범위 예측이 어려운 경우가 있고, 이런 병변에 대해서는 수술 전 혹은 수술 중 담도내시경 및 생검 등의 침습적인 검사가 필요하다.